
Abstract
November marks Lung Cancer Awareness Month, and reminds us that lung cancer is the leading cause of cancer death among women in the United States. In this brief report, we highlight CDC resources that can be used to examine the most recent data on lung cancer incidence, survival, prevalence, and mortality among women. Using the U.S. Cancer Statistics Data Visualizations tool, we report that in 2015, 104,992 new cases of lung cancer and 70,073 lung cancer deaths were reported among women in the United States. The 5-year relative survival among females diagnosed with lung cancer was 22%, and as of 2015, ∼185,759 women were living with a lung cancer diagnosis. We also describe ways CDC works to collect and disseminate quality cancer surveillance data, prevent initiation of tobacco use, promote cessation, eliminate exposure to secondhand smoke, identify and eliminate disparities, promote lung cancer screening, and help cancer survivors live longer by improving health outcomes.
Introduction
T
This report presents recent data on lung cancer incidence, survival, prevalence, and mortality among U.S. women, and describes selected lung cancer surveillance research and programmatic activities at the U.S. Centers for Disease Control and Prevention (CDC) Division of Cancer Prevention and Control.
U.S. Cancer Statistics
The U.S. Cancer Statistics (USCS) are the official federal statistics on cancer.
1
This data resource includes cancer incidence data from CDC's National Program of Cancer Registries (NPCR) and the National Cancer Institute's (NCI) Surveillance, Epidemiology, and End Results (SEER) Program, as well as mortality data from CDC's National Center for Health Statistics' National Vital Statistics System (NVSS). The data are available through multiple data products, and are accessible at the USCS website (
In 2015, the most current year available, the combined data from NPCR and SEER registries provide cancer information on the entire U.S. population—all 50 states and the District of Columbia. In this report, we report cases of invasive lung and bronchus (lung) cancers, identified using the International Classification of Diseases for Oncology, Third Edition (ICD-0-3) site codes C34.0-C34.9.
5
Mortality data in this report also cover 100% of the U.S. population. USCS data on cancer deaths were based on death certificates registered in 2015 and compiled into a national file through NVSS. Cancer mortality data for 2016 are also available (
Survival and prevalence estimates were calculated using data from NPCR-funded central cancer registries that met USCS publication criteria and conducted active case follow-up or linkage with CDC's National Center for Health Statistics National Death Index. 8 In this report, 39 states met these criteria, covering 81% of the U.S. population. The 5-year relative survival proportion was defined as the proportion of persons surviving ≥5 years after a lung cancer diagnosis compared with the proportion of survivors expected in a group of cancer-free persons. The 5-year relative survival proportion was calculated using the Ederer II actuarial method for cases of lung cancer diagnosed during 2001–2014 with follow-up through 2014, accounting for shorter follow-up time of cases diagnosed in more recent diagnosis years. 9 NPCR prevalence proportions were calculated for each combination of age and race group. Cancer prevalence counts on January 1, 2015 for the U.S. population were estimated by multiplying the age- and race-specific NPCR prevalence proportions by the corresponding U.S. population estimates based on the average of the 2014 and 2015 population estimates from the U.S. Census Bureau.
Incidence
Between January 1 and December 31, 2015, a total of 104,992 new invasive lung cancer cases were reported among women in the United States, with an age-adjusted incidence rate of 51 cases per 100,000 women. Each day in 2015, 288 women were told that they had lung cancer.
The lung cancer incidence rate increased with age, with the highest rate (347.3) among women aged 75–79 years. The apparent downturn in the rate among women aged ≥80 years is likely an artifact of birth cohort patterns of smoking; as birth cohorts with the heaviest lifetime history of smoking advance in age, this artifactual downturn disappears. 3 Smoking behaviors, including age at initiation and years smoked, are more similar between women and men in contemporary cohorts than in older cohorts; 10 unfortunately, as a consequence, lung cancer incidence rates are also now similar between young women and men. 11,12 This is one gender gap that unfortunately has narrowed. Notably, 7 of 10 lung cancer cases occur among women aged 55–79 years (Table 1), the age group for which lung cancer screening is recommended for those at high risk of developing lung cancer. 13
Data are from cancer registries meeting U.S. Cancer Statistics data quality criteria, covering 100% of the U.S. population. Cancer registries are supported by CDC's NPCR and the NCI's SEER Program. Rates are the number of cases per 100,000 women and are age adjusted to the 2000 U.S. standard population.
NCI, National Cancer Institute; NPCR, National Program of Cancer Registries; SEER, Surveillance, Epidemiology, and End Results.
Among racial groups, the rate was highest (52.5) among white women. Hispanic women have lower rates of invasive lung cancers (24.0) than non-Hispanic women (53.5) (Table 1). Historically, white women have had higher prevalence of cigarette smoking than black women, and non-Hispanic women have had higher prevalence of cigarette smoking than Hispanic women. 4 Currently American Indian/Alaska Native women have the highest prevalence of cigarette smoking, 14 although this differs widely by region of the country, which is reflected in the sixfold difference between the lowest lung cancer death rates in the Southwest versus the highest in the Northern Plains. 15
By state, in 2015, age-adjusted incidence rates for lung cancers ranged from 22.1 per 100,000 women in Utah to 77.5 in Kentucky (Fig. 1). The five states with highest lung cancer incidence rates among women were Kentucky (77.5), Rhode Island (66.1), Maine (64.3), Tennessee (64.1), and West Virginia (63.9). The five states with the lowest incidence rates were Utah (22.1), New Mexico (33.9), Hawaii (34.3), California (37.1), and Colorado (37.9). Variations among states in lung cancer incidence are influenced by variations in smoking behavior, providing compelling evidence of the value of tobacco control efforts in reducing lung cancer risk. 16

Rate of new invasive lung cancer cases by state, females, United States, 2015. Data are from cancer registries meeting U.S. Cancer Statistics data quality criteria, covering 100% of the U.S. population. Cancer registries are supported by CDC's NPCR and the NCI SEER Program. Rates are the number of deaths per 100,000 women and are age adjusted to the 2000 U.S. standard population. NPCR, National Program of Cancer Registries; SEER, Surveillance, Epidemiology, and End Results.
Mortality
Between January 1 and December 31, 2015, a total of 70,073 deaths among women in the United States were attributed to lung cancer, with an age-adjusted death rate of 34 lung cancer deaths per 100,000 women (Table 2). Each day in 2015, 192 women died from lung cancer. Similar to incidence rates, deaths from lung cancer were highest among white women (34.9/100,000 women) and non-Hispanic women (35.5). The rate of lung cancer deaths among women by states ranged threefold, from 15.6 deaths per 100,000 women in Utah to 51.0 deaths per 100,000 women in Kentucky (Fig. 2).
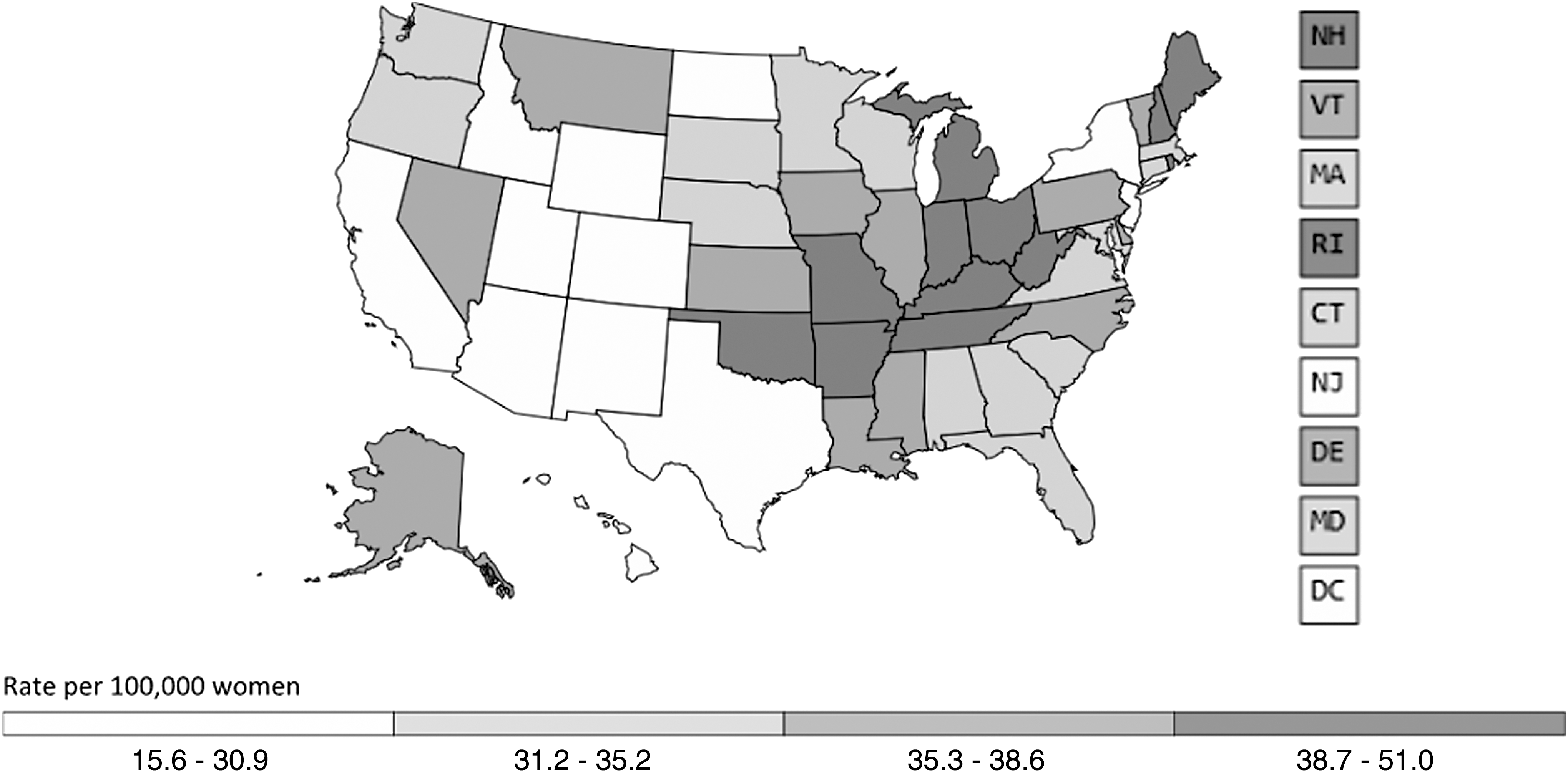
Rate of lung cancer deaths by state, females, United States, 2015. Data are from CDC's National Center for Health Statistics National Vital Statistics System and cover 100% of U.S. population. Rates are the number of deaths per 100,000 women and are age adjusted to the 2000 U.S. standard population.
Data are from CDC's National Center for Health Statistics National Vital Statistics System and cover 100% of U.S. population. Rates are the number of deaths per 100,000 women and are age adjusted to the 2000 U.S. standard population. Rates and counts are suppressed if fewer than 16 deaths were reported in a specific category, such as age, race, and ethnicity. Some counts were suppressed as complementary cell suppression.
Survival
Among women with a lung cancer diagnosed during 2001–2014, the 5-year relative survival proportion was 22% (Table 3). This is higher than that in men (15%) but lower than other common cancers among women such as breast cancer (89%), cervical cancer (68%), and ovarian cancer (46%). 1 Across all racial groups, survival decreased with increasing age. For women younger than 45 years, estimated 5-year relative survival was 33%, while for women 75 years and older it was 16%. Black women had lower 5-year relative survival (19%) than white women (22%) and women of other races (26%).
Estimates are based on cases reported by CDC's NPCR from 2001 to 2014 and follow-up of patients through 2014.
The “other” races group contains IHS-linked American Indian, Alaska Native, and Asian/Pacific Islander cases.
IHS, Indian Health Service-linked; USCS, U.S. Cancer Statistics.
Among women with a lung cancer diagnosed during 2001–2014, half were diagnosed when the cancer had already spread throughout the body (distant stage), a quarter when the cancer had spread to regional lymph nodes or directly beyond the primary site (regional stage), and a fifth at an early (localized) stage. 17 A 5-year relative survival was higher when lung cancer was found early (57%) than at a regional stage (28%) or distant stage (6%). 17 The marked disparity in survival by stage at diagnosis underscores the importance of early detection and effective treatments.
Prevalence
In 2015, there were an estimated 185,759 women alive in the United States who were diagnosed with lung cancer from January 1, 2010 to December 31, 2014 (Table 4). Surviving lung cancer has physical, mental, emotional, social, and financial aspects that start after being diagnosed, and continue through treatment and beyond.
Estimates are based on cases reported by CDC's NPCR from 2001 to 2014 and follow-up of patients through 2014. Prevalence for the United States was estimated by multiplying NPCR prevalence proportions by the U.S. population.
The “other” races group contains IHS-linked American Indian, Alaska Native, and Asian/Pacific Islander cases.
CDC Activities Related to Lung Cancer
CDC is a leader in nationwide efforts to ease the burden of cancer. The CDC Division of Cancer Prevention and Control works with national cancer organizations, state health agencies, and other key groups to develop, implement, and promote effective strategies for preventing and controlling cancer. CDC provides funding and assistance to help states, tribes/tribal organizations, and territories to collect data on cancer incidence and deaths, cancer risk factors, and the use of cancer screening tests. Public health professionals can use these high-quality data to identify and track cancer trends, strengthen cancer prevention and control activities, and prioritize the use of resources. CDC develops communication campaigns and materials to educate health professionals, decision makers, and the public about cancer prevention and control.
Established by Congress through the Cancer Registries Amendment Act in 1992, and administered by CDC, NPCR collects data on cancer occurrence (including the type, extent, and location of the cancer), the type of initial treatment, and outcomes.
18
CDC supports central cancer registries in 46 states, the District of Columbia, Puerto Rico, the U.S. Pacific Island Jurisdictions, and the U.S. Virgin Islands (
CDC funds 50 states, the District of Columbia, Puerto Rico, 6 U.S.-affiliated Pacific Islands, and 8 tribes/tribal organizations through the National Comprehensive Cancer Control Program (NCCCP) to form or support coalitions to fight cancer in their communities.
20
Comprehensive cancer control is a strategic approach to preventing the impact of cancer in communities. For 20 years, CDC's NCCCP has been bringing together stakeholders (i.e., organizations that have an interest in keeping community members healthy) in places throughout the country to create cancer control plans that help lower the number of people affected by cancer. Cancer control plans are developed by cancer programs, and include evidence-based strategies and activities that are tailored to and implemented in high-burden populations (
CDC is one of 18 members of the Comprehensive Cancer Control National Partnership (
CDC improves the health and wellness of cancer survivors through research and practice initiatives, which utilize effective translation, high-quality data, and multisectorial partnerships.
22
For ∼15 years, CDC has supported public-health-driven efforts to improve health outcomes of cancer survivors living with, through, and beyond cancer. The CDC Division of Cancer Prevention and Control has led and partnered research focused on cancer survivors, including those with a history of lung cancers. The prevalence of smoking among cancer survivors stratified by demographic characteristics
23
–25
and mental health status
26
has been examined using population- and state-based survey data, including the National Health Interview Survey (
What increases a woman's risk of developing lung cancer (risk factors)? What can be done, particularly at the community level, to prevent lung cancer?
At least 7 occupations and 18 exposures such as smoking, secondhand smoke, radon gas, diesel exhaust, and particulate air pollution are considered by the International Agency for Research on Cancer to cause lung cancer in humans. 28
Cigarette smoking
Cigarette smoking is an important cause of all types of lung cancers 10 ; women who smoke cigarettes are ∼25 times more likely to get lung cancer or die from lung cancer than women who do not smoke. 29 Lung cancer can also be caused by using other types of tobacco, such as cigars or pipes. 30 Even smoking a few cigarettes a day or smoking occasionally increases the risk of lung cancer. 31 The more years a woman smokes and the more cigarettes smoked each day, the higher the risk of lung cancer. 32 Women who quit smoking have a lower risk of lung cancer than if they had continued to smoke, but their risk is higher than the risk for women who never smoked. 33 Quitting smoking at any age can lower the risk of lung cancer among women. 34
Lung cancer is a family of different cancers, with >30 different histologic variants, which grow differently and are thus treated differently. 35 The National Comprehensive Cancer Network (NCCN) publishes clinical guidelines for two major categories of lung cancer histology: small cell carcinoma (∼14% of lung cancer cases) 36 –38 and non-small cell carcinoma (∼85% of lung cancer cases). 39,40 Adenocarcinoma, a type of non-small cell lung cancer, is the most common type of lung cancer among women. 41 Adenocarcinoma is also the most common type of lung cancer among women who have never smoked. 42 This does not mean, however, that most adenocarcinomas occur among never smokers. 3 A recent study estimated that three-quarters of lung adenocarcinomas in women were found in those who smoked. 10 Changes in the design and composition of cigarettes since the 1960s have increased the risk of lung adenocarcinoma among smokers. 31
Emphasizing primary prevention of cancer is a key priority of the NCCCP, and through collaboration with the CDC Office on Smoking and Health, programs are provided with technical support to combat this disease. These programs have the greatest impact when they are comprehensive, sustained, and accountable and when they combine educational, clinical, regulatory, economic, and social strategies.
43
Proven population-based interventions, including tobacco price increases, comprehensive smoke-free policies, hard-hitting tobacco education media campaigns, and barrier-free access to tobacco cessation counseling and medications are effective in reducing cigarette smoking and smoking-related diseases, including lung cancer among U.S. adults.
31,43,44
Data from the 2015 National Health Interview Survey show that more than half (56%) of women who smoked tried to quit, but only 8% succeeded.
45
Research shows that use of cessation counseling and medication increases quit rates.
46
CDC summarized Federal guidance on insurance coverage of tobacco cessation as a preventive service, including the types of health plans that are required to provide this coverage (
Secondhand smoke
Smoke from other people's cigarettes, pipes, or cigars (secondhand smoke) causes lung cancer. 47,48 Tobacco smoke, including secondhand smoke, contains thousands of toxic chemical compounds, including at least 70 carcinogens. 31,49 In the United States, 1 of 4 nonsmokers are exposed to secondhand smoke, 50 and ∼3,000 women who never smoked die from lung cancer due to secondhand smoke every year. 31
Nonsmokers can be protected from secondhand smoke exposure through comprehensive statewide and local laws prohibiting smoking in workplaces and public places, voluntary smoke-free rules prohibiting smoking in homes and vehicles at all times, and smoke-free policies in multiunit housing. 47 As of July 2018, 27 states and the District of Columbia have passed comprehensive smoke-free laws. 51 As of November 2017, at least 2,082 U.S. colleges and universities had smoke-free policies, twice as many as in 2012. 52 Continued efforts to monitor, promote, implement, and enforce smoke-free laws are critical to protect nonsmokers in the places they live, work, and gather. Smoke-free laws can also prevent the initiation of tobacco use, and motivate and help tobacco users quit.
Exposure to secondhand smoke is high (37%) among those who rent their housing, a proxy for living in multiunit housing. 50 In February 2017, a new Smoke-Free Housing Rule from the U.S. Department of Housing and Urban Development (HUD) went into effect, specifying that all public housing agencies must have a smoke-free policy in place by July 31, 2018. 53 This change was made to improve the health of public housing residents by providing a smoke-free environment. In 2017, ∼10 million people received housing assistance from HUD, and 3 of 4 households were headed by a woman. 54 One-third of women receiving housing assistance from HUD during 2007–2012 were current smokers. 55 CDC and the American Cancer Society, in collaboration with HUD, sponsored a workshop in 2017, and are providing follow-up technical assistance to enhance the capacity of states to implement the Smoke-Free Housing Rule.
Radon
According to the U.S. Environmental Protection Agency (EPA), radon causes ∼21,000 cases of lung cancer each year, making it the second leading cause of lung cancer. 56 EPA estimates that 1 in 15 residences, or ∼7 million homes, in the United States exceed the radon level at which mitigation is recommended to reduce radon exposure. 57 The EPA recommends testing all homes for radon and using proven ways to lower high radon levels.
As of 2017, 39 states and the District of Columbia had radon-related laws that require testing, mitigation, or disclosure of radon levels in real-estate transactions and 11 states require radon-resistant features in new homes.
58
There are federal and state programs to help fund radon reduction in homes that are affordable to limited income families. EPA funds state and tribal radon control programs to subsidize or encourage radon testing in residences and schools, mitigate residences with high radon levels, encourage radon-resistant building practices, and develop professional licensure programs.
59
Many state radon programs offer free radon test kits, and there are inexpensive ways to fix and prevent high radon levels in homes. CDC published Policies and Practices for Cancer Prevention: Reducing Household Radon, which describes how to reduce radon in homes, and what states and comprehensive cancer control programs can do about radon (
Diet, nutrition, and physical activity
The World Cancer Research Fund/American Institute for Cancer Research found that there is strong evidence that arsenic in drinking water and high-dose beta-carotene supplements taken by smokers increase lung cancer risk. 60 Evidence for benefits or risks of other nutritional factors such as physical activity, alcohol use, and vegetable intake is limited. 60
In a recent analysis of NCCCP cancer plans, all programs recognized the importance of nutrition and physical activity in cancer prevention, and most plans included goals and strategies to address these factors for cancer prevention, some of these efforts may help prevent lung cancer. 61
Can lung cancer be detected early?
The U.S. Preventive Services Task Force recommends yearly lung cancer screening with low-dose computed tomography (LDCT) for people between 55 and 80 years old who have a history of heavy smoking (a smoking history of ≥30 pack years), and are either current smokers or have quit within the past 15 years. 13 Lung cancer screening is not a substitute for quitting smoking. The best way to reduce the risk of lung cancer is to not smoke or quit smoking and avoid secondhand smoke. Lung cancer screening does not prevent the development of lung cancer but enables the detection of lung cancer at a localized stage when treatment may be more effective. Lung cancer screening will lead to improved survival rates and reductions in lung cancer mortality, as well as an increase in the number of persons who have survived lung cancer. Lung cancer screening is recommended only for adults who have no symptoms but who are at high risk of developing the disease because of their age and smoking history. Lung cancer screening is not recommended for people who do not meet the age and smoking criteria, such as women who have never smoked, even if they lived with a smoker for many years.
As a preventive service recommended by the U.S. Preventive Services Task Force, lung cancer screening with LDCT is covered under most health insurance plans at no additional cost to the patient. 62 Lung cancer screening is also covered under Medicare, with a requirement that before a program of lung cancer screening is started, a beneficiary must receive a written order for LDCT screening during a lung cancer screening counseling and shared decision-making visit. 63 To facilitate shared decision making, the Agency for Healthcare Quality Research has developed decision aids for patients and clinicians. 64 In a Medscape CDC Expert Commentary, Dr. Lisa Richardson, the director of the CDC Division of Cancer Prevention and Control, discussed the importance of lung cancer screening recommendations, and offers tips for clinician checklists and reimbursement aids. 65
CDC supported a National Academy of Sciences, Engineering and Medicine Workshop on issues related to implementation of lung cancer screening, such as the incorporation of shared decision-making and smoking cessation services into screening. 66 In 2017, the American Cancer Society convened the first National Lung Cancer Roundtable to promote lung cancer awareness, prevention, early detection, and assurance of optimal therapy through public education, provider education, targeted research, and health policy initiatives; representatives from CDC participate in the Tobacco Treatment Task Group. 67
Based on data from the 2015 National Health Interview Survey, nationally only 4% of women smokers eligible for lung cancer screening received it in 2015.
68
CDC developed an optional module for the Behavioral Risk Factor Surveillance System about lung cancer screening, including three questions about pack-year smoking history and one question about use of CT scans for lung cancer screening (
NCCCP awardees can partner with healthcare providers, clinics, and medical associations to increase lung cancer screening and cigarette smoking cessation among persons at high risk of lung cancer; with state and local health departments, who can provide crucial support by identifying, tracking, and providing data (outcome measures) and mapping community problems and by providing forums for community planning and conduct and sponsoring education of community leaders; and with state and local tobacco control programs to provide unified messages about the importance of tobacco control to prevent lung cancer and lung cancer screening to reduce lung cancer deaths. CDC published Policies and Practices for Cancer Prevention: Lung Cancer Screening Programs, which describes how NCCCP awardees and other community partners can increase awareness about lung cancer screening among people who are at high risk (
What can women diagnosed with lung cancer do to improve their prognosis?
Lung cancer is treated in several ways, depending on the type of lung cancer and how far it has spread. Women with small cell lung cancer are usually treated with radiation therapy and chemotherapy. 37,38 Women with non-small cell lung cancer can be treated with surgery, chemotherapy, radiation therapy, targeted therapy, or a combination of these treatments. 39,40 The selection of treatment has been improved by the development of laboratory tests for molecular or genetic markers (e.g., EGFR mutation, ALK fusion) to better identify specific characteristics of a patient's lung cancer cells. 39 Targeted therapy, sometimes referred to as precision medicine or personalized therapy, is designed to selectively target molecular or genomic pathways responsible for the characteristics of a patient's lung cancer cells. New types of treatment are being tested in clinical trials. CDC Division of Cancer Prevention and Control is examining racial-ethnic disparities in the receipt of lung cancer staging procedures. 69
Surviving lung cancer has physical, mental, emotional, social, and financial aspects that start after being diagnosed, and continue through treatment and beyond. A survivorship care plan is a record of a person's cancer and treatment history, as well as any checkups or follow-up tests needed in the future. 70 It may also list possible long-term effects of treatments and ideas for staying healthy. One of the most important ways to stay healthy is avoiding tobacco use and tobacco smoke. Even after lung cancer diagnosis, smoking cessation can reduce the risk of dying. 31 Cancer survivors who quit smoking experience lower risks of dying from their cancer or of developing subsequent cancers compared with those who continue to smoke. 31 Cancer survivors who receive advice about cessation from their healthcare provider are more likely to quit tobacco use. 46
How can healthcare providers and communities help women diagnosed with lung cancer?
Healthcare providers can help women diagnosed with lung cancer by talking with them about the risks of tobacco use after a cancer diagnosis, asking them whether they use tobacco products, encouraging those who do to quit, assessing their willingness to quit, and assisting them to quit using evidence-based cessation treatment. 44 Individual, group, and telephone cessation counseling and seven FDA-approved cessation medications are each effective in helping people quit tobacco use. 46,71 Cessation counseling and pharmacotherapy are even more effective when they are combined than when either is used alone. 46,71 Understanding when and if specific types of cessation treatments are used can help with planning interventions and development of survivorship care plans to enhance the length and health-related quality of life. Healthcare providers could also follow up with lung cancer survivors regularly about their tobacco use, and identify and address psychosocial issues as part of recommended distress screening, as indicated.
Addressing cancer survivor needs is the central goal of the CDC Division of Cancer Prevention and Control and of the NCCCP. 22,72 CDC supports awardee and stakeholder efforts for survivorship activities related to surveillance, research translation and evaluation, survivorship care plans, patient navigation, and provider education.
Conclusion
Through varied partnerships and activities, CDC works to collect and disseminate quality lung cancer surveillance data, prevent initiation of tobacco use, promote cessation, eliminate exposure to secondhand smoke, identify and eliminate disparities, promote lung cancer screening, and help cancer survivors live longer and healthier lives by developing good behaviors.
Footnotes
Acknowledgment
Work for this article was done by federal employees. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.