
Abstract
Background:
Spontaneous preterm delivery (sPTD) is associated with a twofold increased risk of future maternal cardiovascular disease. We hypothesized that women with sPTD would demonstrate greater vascular dysfunction postpartum compared to women with term delivery.
Materials and Methods:
In a case-controlled, matched pilot study, we enrolled 20 women with sPTD (gestation ≤34 weeks), and 20 term control women (gestation ≥39 weeks) were matched for age (±5 years), parity, ethnicity, and route of delivery. Vascular function, serum lipids, C-reactive protein, and interleukin-6 were completed within 24–72 hours postpartum. Statistical analysis included paired t-tests based on match and mixed effects linear regression models and adjusted for potential confounders.
Results:
The mean age for sPTD and term controls was 33 ± 6 years and 32 ± 6 years, respectively. Women with sPTD had significantly lower augmentation index-75 (24.1% ± 16.1% vs. 39.9% ± 15.2%, p = 0.001) and central pulse pressure (29.1 ± 5.4 mmHg vs. 34.6 ± 4.7 mmHg, p = 0.004), but no difference in pulse wave velocity (5.1 ± 1.6 m/s vs. 5.6 ± 1.5 m/s, p = 0.12) compared to controls. Women with sPTD had significantly lower high-density lipoprotein cholesterol (59.4 ± 12.5 mg/dL vs. 67.6 ± 13.1 mg/dL, p = 0.035) compared to controls. Analysis of chorioamnionitis and magnesium sulfate did not alter the results.
Conclusions:
Women with sPTD have signs of lower smooth muscle tone in the early postpartum period compared to women with term delivery. Further research is required to understand mechanistic pathways in sPTD and future maternal cardiovascular disease risk.
Introduction
Atherosclerotic cardiovascular disease (ASCVD) remains the leading killer of women worldwide, 1 surpassing all cancer deaths combined. In fact, one in three women die from ASCVD. 1,2 Although many ASCVD risk factors have been well established, less is known about whether a woman's adverse response to pregnancy can be interpreted as an early marker for later maternal ASCVD risk. 2 –5
Studies indicate that the type of preterm delivery a woman experiences can predict the magnitude of risk for future ASCVD (i.e., spontaneous preterm delivery (sPTD) vs. medically indicated preterm delivery). 3,5 –8 For example, women with iatrogenic preterm delivery following a diagnosis of preeclampsia have more than an eightfold higher risk for CVD-related death than those women who delivered at term without preeclampsia. 9 In contrast, women with sPTD have a 2.95-fold increased risk of death from cardiovascular causes than those women who delivered full term without complication. 9 These data support the concept that preclinical vascular dysfunction, such as the increased arterial stiffness associated with adverse pregnancy outcomes (APOs), may predispose these women to subsequent development of future ASCVD. 3,4,10 –14
Our hypothesis is that women who experience sPTD will have abnormal cardiovascular markers compared to those term women postpartum. Our aim is to compare markers of ASCVD risk (vascular function, cholesterol levels, and inflammatory markers) between women who experienced sPTD ≤34 weeks of gestation and control women who delivered at term ≥39 weeks of gestation.
Materials and Methods
Design and study population
We performed a pilot study with case–control design, in which we prospectively enrolled women with sPTD and matched term controls by age (±5 years), parity, route of delivery, and self-reported race/ethnicity to women with a term delivery (term controls) to compare risk factors for ASCVD 24–72 hours postpartum. Women with sPTD (≤34 weeks gestation) and women with term deliveries (≥39 weeks gestation) were considered eligible if they met the following inclusion criteria: age ≥18 years; English and/or Spanish speaking; singleton birth; no medical indication for delivery or significant medical problem, such as hypertensive disorders of pregnancy, diabetes; nonsmoker; no prior history of ASCVD, including ischemic heart disease, acute myocardial infarction, acute coronary syndrome, coronary or peripheral revascularization, stroke, trans-ischemic attack, or diabetes.
Women were recruited from the labor and delivery unit at a large urban academic medical center, which draws from a diverse metropolitan population, and has ∼6700 deliveries per year. The study was approved by the internal review board at Cedars-Sinai Medical Center (IRB No. 32089).
Vascular measurements
Augmentation index 75 beats per minute
A measurement of pulse wave analysis, augmentation index 75 beats per minute (AIx75) is defined as the ratio of augmentation pressure to central pulse pressure (CPP) and expressed as a percentage. Augmentation index assesses for arterial stiffness by vascular smooth muscle tone in the smaller vascular beds. 15 Measuring AIx75 records the brachial pulse waveform through measurements taken by an arm cuff and is noninvasive, accurate, and reproducible. 15,16
Increased AIx75 is associated with the presence and extent of coronary artery disease 17 and may be a useful marker of ASCVD risk. 18 Research has demonstrated that AIx75 may be indicative of ASCVD risk when utilized in younger populations. 18,19 During pregnancy, AIx75 values decrease in the first and second trimesters and increase during the third trimester, relative to prepregnancy values, and may even exceed prepregnancy levels in the postpartum period. 13,20 –22 Augmentation index was assessed using the noninvasive cuff-based SphygmoCor Xcel system (AtCor Medical, Australia). 23,24
Central pulse pressure
We calculated CPP with cuff-based oscillometry at the brachial artery, defined as the difference between systolic and diastolic blood pressure (BP). CPP is a superior predictor of future adverse cardiovascular events than peripheral pulse pressure. 15,25
Pulse wave velocity
Carotid-femoral pulse wave velocity (PWV) is an independent predictor of cardiovascular risk and mortality in diseased, mid-life to older adults. It is considered the gold standard for measuring arterial stiffness. 26 PWV is a direct measurement of arterial stiffness by the aortoiliac pathway. The aortoiliac pathway is a more elastic, larger vessel and measures the speed of a pressure wave along a length of artery over time. 15,23 The stiffer the artery, the higher the PWV. 27 To control for operator variability and accuracy, all testing was completed by a single investigator (M.B.M.) trained in performing these measurements and the data were reviewed by a vascular core laboratory.
Serum lipids and inflammatory panels
During the first 24–72 hours postpartum and before hospital discharge, nonfasting peripheral blood draw was performed. The lipid panel included total cholesterol, high-density lipoprotein cholesterol (HDLc), low-density lipoprotein cholesterol, and triglycerides. Interleukin-6 (IL-6) was measured by sandwich enzyme-linked immunosorbent assay using a commercially available kit (R&D Systems, Inc., Minneapolis, MN). Highly sensitive C-reactive protein was measured by high-sensitivity sandwich ELISA (Dade Behring Diagnostics, Marburg, Germany). Samples were transferred in batches every 2 weeks to LabCorp for analysis.
Patient approach
Women on labor and delivery, who met the above inclusion criteria and were anticipated to deliver ≤34 weeks or ≥39 weeks, were referred to the study team by their treating physician. The study team contacted the patient either before the delivery or within the first 24 hours after delivery to explain the study, offer participation, and obtain informed consent from those who chose to participate. Informed consent was obtained before any research procedures.
After enrollment and between 24–72 hours postdelivery, all vascular testing was conducted in the patient's private room at a time when minimal visitors were present and no other health care activities were scheduled. Vascular procedures (AIx75, CPP, and PWV) were completed while the patient was in bed and took no more than 1 hour. All serum samples (lipids and inflammatory markers) were drawn on the same day as the vascular procedures.
A prospective review of the electronic medical record was conducted to record clinical data, including medications such as magnesium and antibiotics given to the participant during delivery. As per our protocol, for any woman expected to deliver before 33 weeks gestation, magnesium sulfate was administered antepartum for neonatal neuroprophylaxis. None of these women were on magnesium postpartum. Each participant completed a self-report questionnaire to obtain demographic data. All women in the sPTD group had their placentas sent to pathology for potential confirmation of chorioamnionitis and were included in the study. Chorioamnionitis was considered to be present if the diagnosis was made clinically and documented in the medical record or if there was a pathologic diagnosis made.
Data analysis
Data were analyzed using SPSS release 21 for Windows (Chicago, IL), SAS version 9.3 (Cary, NC), and R version 3.2. For all analyses, the significance level was set at p < 0.05. Unmatched baseline sociodemographic and unmatched clinical variables and cardiovascular risk markers (prepregnancy body mass index (BMI) and family history of ASCVD) were compared using conditional logistic regression models where the outcome was the group (sPTD vs. term control) and the models were adjusted for the variable in question and stratified by match. Mixed-effects linear regression models with a random effect for match were used to compare outcomes of interest (AIx75, CPP, and PWV) between the two groups and adjust for potential confounding effects among other variables measured. For post hoc pairwise comparisons of groups in these outcomes, a Tukey–Kramer adjustment was made to the p-values.
Results
A total of 42 women, 22 with sPTD and 20 with term delivery, enrolled in the study. Two of the women with sPTD declined participation after signing consent because of emotional stressors surrounding their preterm delivery. Therefore, 40 women (20 sPTD and 20 term controls) completed AIx75 and CPP measurements. Of the 40 women, 34 completed PWV measurements. One woman in the term control group and five women in the sPTD group did not have PWV calculated due to the inability to capture a quality waveform. One woman in the sPTD group did not complete the blood draw. Mean gestational age at delivery was 30.8 ± 2.9 weeks for the women with sPTD and 39.6 ± 1.1 weeks for the term controls. Eighty percent (16/20) of the women with sPTD experienced premature rupture of membranes (PROM), while 20% had preterm labor as the etiology of their preterm delivery.
Women who received magnesium (n = 10) for neuroprophylaxis had an administration mean time of 81 hours before vascular function testing. There were no significant differences in demographics, clinical variables, or delivery route between the groups (Table 1).
Demographic and Clinical Characteristics of Term Controls and Spontaneous Preterm Delivery
SD, standard deviation; sPTD, spontaneous preterm delivery. mg/L, milligrams per liter; #, number; %, percent.
Vascular function
Women with sPTD had significantly lower AIx75 (24.1% ± 16.1% vs. 39.9% ± 15.2%, p = 0.001) and CPP (29.1 ± 5.4 mmHg vs. 34.6 ± 4.7 mmHg, p = 0.004), respectively, compared to term controls. There were no differences between sPTD and term controls in PWV (5.1 ± 1.6 m/s vs. 5.6 ± 1.5 m/s, p = 0.12), respectively (Table 2).
Vascular Function in Term Controls versus Spontaneous Preterm Delivery
AIx75, augmentation index 75 beats per minute; CPP, central pulse pressure; PWV, pulse wave velocity, otherwise as prior.
Bold represents statistical significance.
In addition, women with sPTD and chorioamnionitis (n = 8) had significantly lower AIx75 than term controls (13.5% ± 13.7% vs. 39.9% ± 15.2%, p = 0.001), respectively, while women with sPTD without chorioamnionitis had a trend toward lower AIx75 than term controls (26.6% ± 15.9% vs. 39.9% ± 15.2%, p = 0.065), but did not reach statistical significance. Of note, all eight women with a diagnosis of chorioamnionitis experienced PROM (Table 3).
The Association Between Chorioamnionitis and Vascular Function in Spontaneous Preterm Delivery versus Term Controls
Post hoc pair-wise Tukey–Kramer adjustment. The comparison listed is to term controls.
Bold represents statistical significance.
Among sPTD women who received magnesium sulfate (n = 10), their infant's gestational age was significantly less than sPTD women who did not receive magnesium sulfate (n = 10) (30 weeks ±15 days vs. 32.50 weeks ±19 days, p = 0.002), respectively. In post hoc Tukey adjusted tests for pair-wise comparisons of the groups, there were no differences in AIx75 between women with sPTD who received magnesium versus women with sPTD who did not receive magnesium. However, there was significantly lower AIx75 in women with sPTD who received magnesium and had chorioamnionitis versus their matched term control (7.6% ± 13.1% vs. 39.9% ± 15.2%, p = 0.002) (Fig. 1).
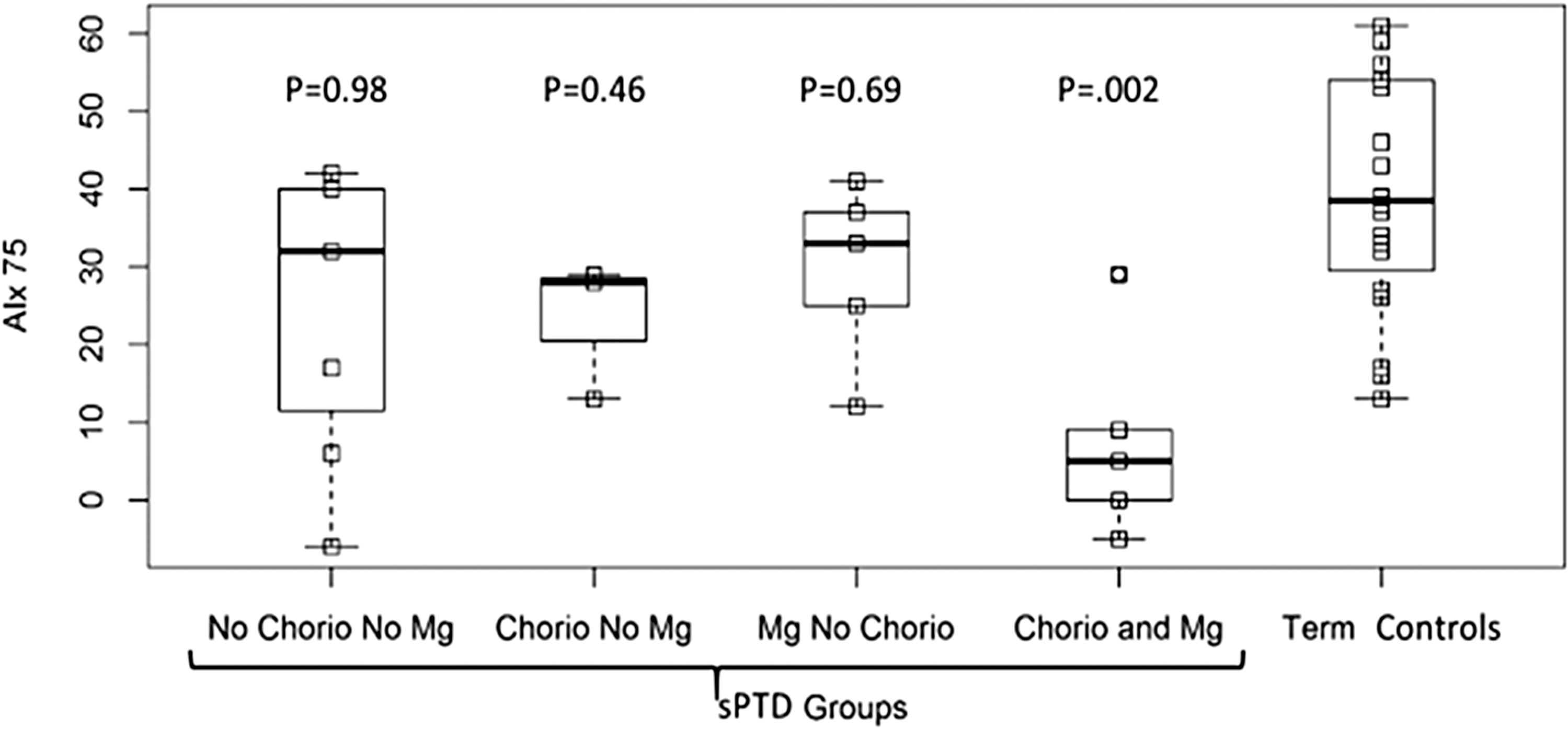
Women with sPTD with or without chorioamnionitis or magnesium versus term controls and AIx75. Model of adjusted tests for pair-wise comparisons of arterial stiffness measures across five groups (term control [n = 20], sPTD without chorioamnionitis and no magnesium [n = 7], sPTD with chorioamnionitis and no magnesium [n = 3]), sPTD with magnesium and no chorioamnionitis [n = 5], and sPTD with chorioamnionitis and magnesium [n = 5]) significantly differed for AIx75 (p = 0.002) compared to term controls. AIx75, augmentation index controlled for a heart rate of 75 beats per minute; Chorio, chorioamnionitis; Mg, magnesium; sPTD, spontaneous preterm delivery.
Serum lipid and inflammatory markers
The only lipid or inflammatory marker that was significantly different between the groups was HDLc (Table 4). Compared to term controls, women with sPTD had significantly lower HDLc (59.4 ± 12.5 mg/dL vs. 67.6 ± 13.1 mg/dL, p = 0.035), respectively. After adjusting BMI, systolic BP (SBP) at baseline, educational level, and marital status, the HDLc difference between groups remained significant (p = 0.005).
Results from Lipid and Inflammatory Markers in Spontaneous Preterm Delivery versus Control Groups
HDL, high-density lipoprotein calculated, hsCRP, highly sensitive C-reactive protein; IL-6, interleukin-6; LDL, low-density lipoprotein calculated; TC, total cholesterol, TRG, triglycerides; mg/dL, milligrams per deciliter; pg/mL, picograms per milliliter.
Bold represents statistical significance.
Discussion
In a matched prospective pilot study of women with sPTD compared to term controls, women with sPTD have significantly lower smooth muscle tone measured by AIx75 and CPP, but not lower arterial stiffness measured by PWV, compared to matched term controls 24–72 hours postpartum. Our subgroup and modeling analyses suggest the hypothesis that these findings are likely related to timing of the delivery rather than related to chorioamnionitis or magnesium sulfate. 29 The most likely explanation for our finding of lower smooth muscle tone is gestational age related and the known lower AIx75 has been previously observed mid-pregnancy. 30,31 Notably, we did not find an elevated AIx75 such as preeclampsia, as we hypothesized, suggesting that sPTD mechanistically is different from hypertensive disorders of pregnancy APOs.
Differences in vascular function between controls versus sPTD
Many investigators have assumed that sPTD would have increased arterial stiffness to a degree similar to that which was described in the preeclampsia literature and therefore have collected sPTD and medically indicated preterm delivery together in their data collection processes. 32,33 Our results concur with Khalil's findings that women with sPTD have lower arterial stiffness than matched controls. However, Khalil et al. 34 studied arterial stiffness in women with all-cause preterm delivery (sPTD and medically indicated preterm delivery) compared to controls at a single time point (11–13 weeks of gestation). They found that women with medically indicated preterm delivery had significantly higher arterial stiffness than women with sPTD and term delivery during early pregnancy. 34 Interestingly, they saw a decreased systemic arterial response in early pregnancy (AIx75) to sPTD <34 weeks compared to controls. 34 This may be an important finding as these women have not yet been exposed to medications and/or infection. They also did not see differences in PWV between groups. 6
Our findings provide evidence that the three measures of arterial stiffness we examined (AIx75, CPP, and PWV) are not interchangeable, 35 and provide a more detailed picture of vascular function that includes large artery elasticity and smaller artery tone. Furthermore, we do not understand if lower vascular measures indicating decreased arterial stiffness equate to healthier blood vessel function. More research is needed in this area to fully discern the idea that women with sPTD are potentially more vasodilated and possibly not fully augmenting their vascular tone compared to term controls immediately postpartum.
Exposures to external and internal environmental factors
A potential explanation for relatively lower arterial stiffness in women with sPTD compared to controls may be related to chorioamnionitis. Infection such as chorioamnionitis accounts for 10% of all preterm births, 36 although the mechanisms behind its implications for preterm birth are not fully understood. 28,36 Our data suggest that women with sPTD and chorioamnionitis had a lower AIx75 compared to those women who did not have clinical symptoms diagnosed by their physician or placental pathological evidence of chorioamnionitis.
Differences in HDLc in sPTD versus controls
Women with sPTD demonstrated HDLc levels below those considered protective against ASCVD risk, while women who experienced a term delivery had HDLc levels similar to those of young adult, nonpregnant women. 37 This relationship remained significant after adjustment of potential confounders, including BMI, SBP, education level, and marital status. HDLc is an important risk predictor for ASCVD. Future work is needed to replicate this finding, and investigate potential mechanistic links between HDLc, sPTD, and future ASCVD.
Inflammation in sPTD
Approximately 75% of all preterm deliveries are the result of sPTD as opposed to medically indicated preterm delivery. The etiology of sPTD is roughly split between spontaneous preterm labor and preterm premature rupture of membranes. There are multiple hypothesized etiologies of sPTD, including inflammation or infection, 28 which may account for at least 25% of such deliveries and may not be clinically manifested. 39 Understanding the relationship of inflammation alone to sPTD is complicated because birth itself has been described as an inflammatory process and many women with sPTD may have multiple etiologies, including overdistension of the uterus and chronic abruption. 36,38 Although we did not find group differences in CRP and IL-6, other investigators have reported elevated CRP and IL-6 levels in women with unspecified preterm delivery compared to controls. 8,40,41
Strengths and limitations
Our study has several strengths. Most notably, it is the first of the kind to compare measures of arterial stiffness immediately (i.e., 24–72 hours postpartum) in women with sPTD and term controls. It was performed in a large tertiary care medical center in a diverse metropolitan city, which supports its external validity. Our use of matched controls likely ameliorated the potential effects of age, self-reported race/ethnicity, parity, and route of delivery.
The use of a single operator increases intrarater reliability in their ability to obtain arterial stiffness measures; in addition, quality control software verifies accuracy between three measurements and is verified by a vascular core laboratory. 42 Despite the fact that the study measures were taken during an often hectic time in the lives of new mothers, our retention rate was strong (95%), which further supports internal validity.
We acknowledge several limitations. Unexpectedly, 80% of the women with sPTD had PPROM, which was more than would be expected since PPROM usually accounts for approximately half of women with sPTD. The only explanation of this is chance and the small n planned for this pilot study. However, we cannot exclude the possibility that our findings may be generalizable largely to women with PPROM. Another potential limitation is that all our women who delivered ≤32 weeks received magnesium for neonatal neuroprophylaxis; therefore, it is difficult to differentiate if magnesium played a significant role in decreased arterial stiffness. Although we found group differences in AIx75 and CPP, we are unable to generalize based on these data for the following reasons: we were limited with a one-time, immediate postpartum measure, which may not be a representative of later measures because unique physiological changes occur at that time point.
In addition, there are changes in the renin-angiotensin-aldosterone system within the first 3 days postpartum, which may affect arterial compliance. Furthermore, our inability to obtain quality PWV waveforms in all women is a limitation. This was related mostly to positioning and the hectic hospital room environment. Controlling the patient room environment such as noise, the inability for some women to fast due to breastfeeding, temperature, and interruptions such as a baby crying during vascular testing may have maternal physiologic implications. Women in the two groups had inherently different postpartum experiences (possible differences in maternal stress), which may have affected their testing. Most notably, women in the sPTD group did not have their infants in their rooms, while most of the women in the normal control group had infants and spouses in their rooms during testing. This potentially allowed for group differences due to different clinical environments between the two groups.
Conclusions
Women with sPTD have significantly lower smooth muscle tone measured by AIx75 and CPP, but not lower arterial stiffness measured by PWV, compared to matched term controls. In addition, women with sPTD have lower HDLc compared to matched term controls. These results suggest physiological differences between the two groups, which may result from timing of the delivery or compounding of vasodilatory effects in smooth muscle tone. Analysis of chorioamnionitis and magnesium sulfate did not alter the results. Future research is required to both understand these results as well as to elucidate how sPTD differs mechanistically from other APOs, in association with increased maternal ASCVD risk.
Footnotes
Acknowledgments
Research reported in this study was supported by the National Institutes of Health under the award No. F31NR015725. CTSI support UL1TR000124 and UL1TR001881-01, and the Preventive Cardiovascular Nurses Association through the American Nurses Foundation (No. 5362). Additional support was provided by the Cedars-Sinai Department of Obstetrics and Gynecology, the Cedars-Sinai Brawerman Nursing Institute, Department of Nursing Research, and the Cedars-Sinai Barbra Streisand Women's Heart Center. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.