
Abstract
Objective:
Poor prenatal oral health has implications for maternal, fetal, and infant health. Studies have shown an association between periodontal disease and adverse pregnancy outcomes, such as preterm delivery, low birth weight, and pre-eclampsia. The objective of this study was to identify the factors associated with preventive dental visits before and during pregnancy and examine the relationship of dental insurance with those visits among Virginia women.
Methods:
The Virginia Pregnancy Risk Assessment Monitoring System (2012–2014) cross-sectional data were used to explore the use of dental cleaning visit among women. The bivariate and multivariate analyses included sociodemographic variables, health risk factors, chronic conditions, oral health knowledge, and oral health promotion variables. All estimates were weighted; p < 0.05 was considered statistically significant.
Results:
A total of 1,344 weighted respondents represented ∼293,608 women in Virginia. Overall, 56% of women reported a before pregnancy dental cleaning visit, and 47% of women reported a during pregnancy dental cleaning visit. Nearly 60% of women were non-Hispanic white, 78% were between 20 and 34 years of age, and 67% reported having dental insurance. Dental insurance (odds ratio [OR] = 3.5; 95% confidence interval [95% CI] = 2.17–5.67) and oral health knowledge (OR = 2.8; 95% CI = 1.42–5.48) were associated with before pregnancy dental visit. During pregnancy dental visit was strongly associated with dental insurance (OR = 5.8; 95% CI = 2.80–11.97), before pregnancy dental visit (OR = 20.72, 95% CI = 11.14–38.54), and oral health promotion by health provider (OR = 12.37, 95% CI = 7.31–20.93).
Conclusions:
Overall, the use of a preventive dental visit before and during pregnancy was low among Virginia women. Improving the use of routine dental visits before pregnancy, increasing access to dental insurance, and engaging health care providers to promote oral health can impact the use of dental care during pregnancy.
Introduction
Pregnancy is a unique period in women's lives characterized by complex physiological changes that can adversely affect oral health. 1 Bleeding gums, gingival inflammation, and periodontal disease are some of the commonly reported problems during pregnancy. According to the American Academy of Periodontology, periodontal disease is an inflammatory disease that affects the soft and hard structures that support the teeth. 2 During pregnancy, the inflammatory response is promoted due to change in hormone levels leading to increased risk of gingivitis and periodontitis.
Numerous researchers have found linkages between periodontal disease and poor pregnancy outcomes, such as preterm birth, low birth weight, and pre-eclampsia. 3 –5 A 2012 study by Guimaraes et al. using data on more than 1,200 postpartum women found that women who presented with periodontitis were twice as likely to have low birth weight (<2,500 g) or very low birth weight babies (<1,500 g) at birth. 6 Another study using the Pregnancy Risk Assessment Monitoring System (PRAMS) data from 10 states found that women who did not have a dental cleaning during pregnancy were 23% more likely to deliver prematurely. 7
The significance of addressing oral health among pregnant women has been highlighted by the Institute of Medicine and the U.S. Surgeon General Report. 8,9 A large body of evidence shows that routine preventive and restorative dental procedures are safe throughout pregnancy and can prevent progression of dental diseases. 10,11 However, the use of dental services before and during pregnancy is quite low, and disparities exist in the use of dental services. 12,13 A recent report based on West Virginia data found that only 47% of women had a pre-pregnancy dental visit. The report found that women who were non-white, between 20 and 29 years of age, less educated, and uninsured or had Medicaid were less likely to have a dental visit during the preconception period compared with their counterparts. 14
Dental insurance plays a vital role in access and use of oral health services. A 2015 survey by Cigna found that one in every three women reported a financial barrier to a dental visit, and pregnant women who lacked dental insurance were two times less likely to visit dentist compared with those with dental insurance. 15 The same survey found that 45% of pregnant women reported poor oral health and 76% had an oral health problem such as bleeding gums or toothaches during pregnancy.
According to the 2012–2013 Virginia Behavioral Risk Factor Surveillance System data, 69% of adult women (18–44 years of age) reported a dental visit in the past year. 16 However, the prevalence of a dental visit among Virginia women during pregnancy was only 43.6% in 2011. 17 There are considerable gaps in dental utilization, and to our knowledge, no information is available at the state level to understand these differences and associated factors. This study used Virginia PRAMS data to explore the prevalence of a preventive dental cleaning visit before and during pregnancy. Our primary objective was to identify the factors associated with a preventive dental visit before and during pregnancy and examine the relationship of dental insurance with those visits among women.
Methods
Data source and population
The study included Virginia PRAMS data from 2012 to 2014. Virginia PRAMS data are de-identified survey data collected annually by the Virginia Department of Health (VDH) in collaboration with the Centers for Disease Control and Prevention (CDC). It is designed to monitor selected self-reported maternal behaviors, conditions, and experiences before, during, and after pregnancy among women who deliver live-born infants. Details on the PRAMS methods are available on the PRAMS website (
The PRAMS questionnaire consists of three parts (core, optional, and state-specific questions). Survey data are linked to selected birth certificate data and weighted for sample design, nonresponse, and noncoverage. For this study, the PRAMS data were requested directly from the VDH, a state public health agency.
This study was approved by the Virginia Commonwealth University (VCU) Institutional Review Board (IRB) and by the VDH IRB as an exempt study. A data sharing agreement was completed between the VDH and VCU. Three years of data were pooled together, and average estimates for the 2012–2014 period were calculated. In 2012, there were 316 Virginia PRAMS participants, and the weighted response rate was 53%. In 2013 and 2014, there were 505 and 523 participants, respectively, and the weighted response rate for both years was 45%.
Outcome variables
Two preventive dental visit utilization outcomes were defined based on the timing of the dental visit. For the first outcome, respondents were asked, if they had their teeth cleaned by a dentist or dental hygienist at any time during the 12 months before they became pregnant with their new baby, hereafter referred to as “before pregnancy dental visit.” For the second outcome, respondents were asked, if they had their teeth cleaned by a dentist or dental hygienist during their most recent pregnancy, hereafter referred to as “dental visit during pregnancy.”
Dental insurance
Dental insurance was the primary variable of interest. Respondents were asked if during their most recent pregnancy they had insurance to cover their dental care. Since the dental insurance question was not asked during the pre-pregnancy period, we assumed that women who reported having dental insurance during pregnancy also had dental insurance before pregnancy. In Virginia, Medicaid did not provide a dental benefit to pregnant women during the study period; thus, it is less likely that dental insurance status varied by pregnancy status.
Other variables
Sociodemographic variables included age in years (younger than 19, 20–34, and 35 and older), race/ethnicity (Hispanic, non-Hispanic [NH] white, NH black, NH other), marital status (married, other), educational level (less than high school [HS], high school graduate, some college and college graduate or more), and annual household income ($26,000 or less, $26,001–$37,000, $37,001–$67,000, and $67,001 and above). Health-related risk factors included the mother's body mass index (BMI; underweight, normal, overweight/obese), tobacco use, and alcohol use. Tobacco use and alcohol use were assessed by inquiring if the women smoked any cigarettes or had any alcoholic drinks during the 3 months before getting pregnant.
Dichotomous variables for oral health knowledge and oral health promotion by health provider were included. Women were asked if during their most recent pregnancy (1) they knew it was important to care for teeth and gums during pregnancy and (2) if a dental or other health care worker talked with them about how to care for their teeth and gums. Chronic health conditions included diabetes (type 1, type 2, or gestational diabetes), pre-pregnancy report of high blood pressure/hypertension, and depression.
Statistical analyses
To account for the complex multistage sampling design of PRAMS, SAS callable SUDAAN version 9.0.1 (Research Triangle Institute, Research Triangle Park, NC) was used to calculate weighted estimates and 95% confidence intervals (95% CIs). Chi-square tests assessed bivariate associations of the pre-pregnancy dental visit and the dental visit during pregnancy with other variables. Two multivariate logistic regression models were developed to obtain adjusted odds ratios (ORs). The Wald F tests were used to determine the association of both dental utilization outcomes with dental insurance and other correlates. In addition to other variables, the model examining a dental visit during pregnancy also included the pre-pregnancy dental visit measure and the oral health promotion variable.
Results
Our total sample size was 1,344 women representative of 293,608 women who had live births during the 2012–2014 year in Virginia. Overall, 56% of women (n = 788) reported a before pregnancy dental visit, and 47% of women (n = 645) reported a dental visit during pregnancy (Fig. 1 and Table 2).
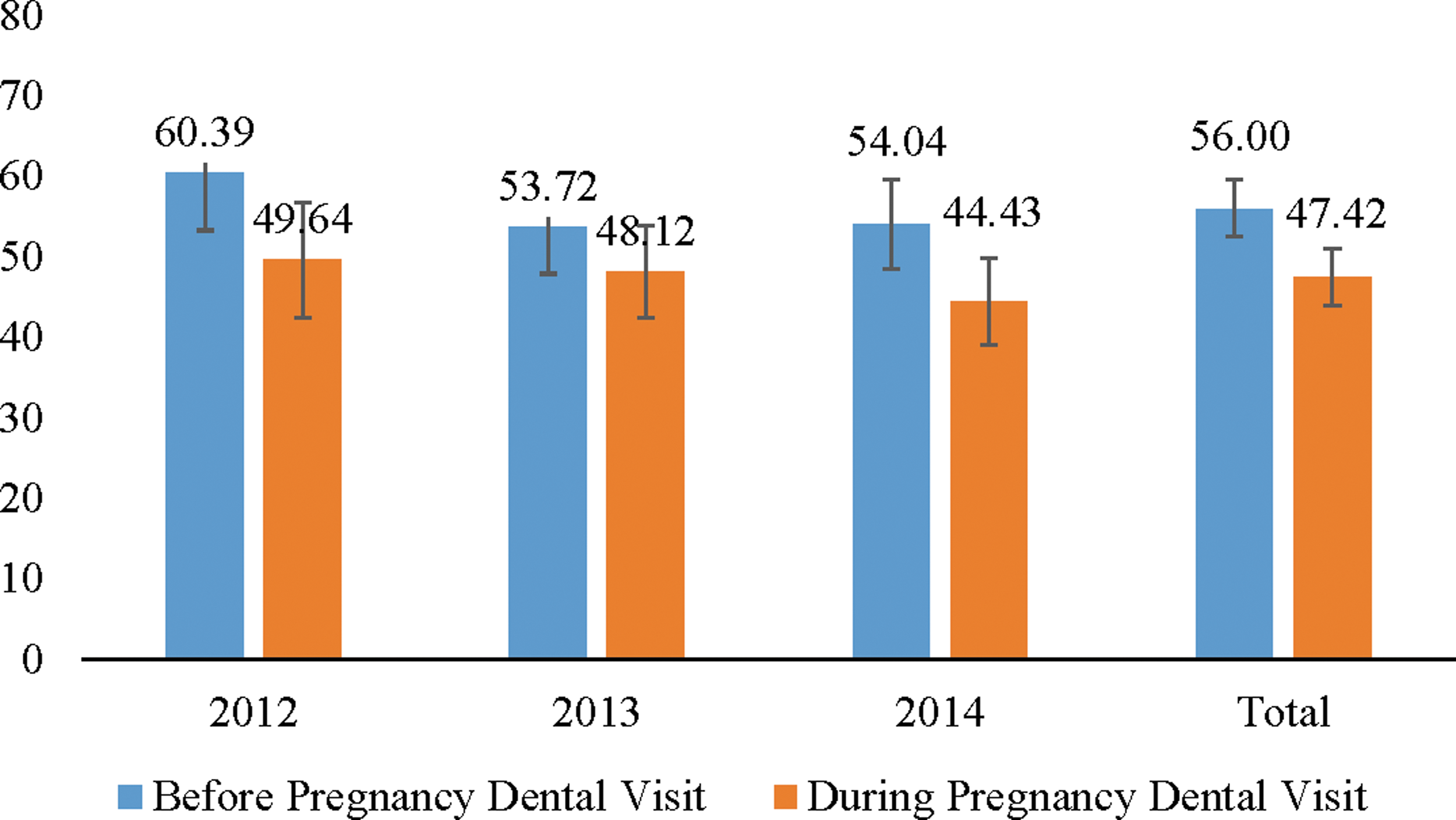
Distribution of a before pregnancy and during pregnancy dental visit by yeara—Virginia PRAMS data. aCochran–Armitage trend test significant for before pregnancy and during pregnancy dental visit at p < 0.001. PRAMS, Pregnancy Risk Assessment Monitoring System.
In the study population, two in every three women reported having dental insurance (78%) were between 20 and 34 years of age, 16% Hispanic, 59% NH white, 15% NH black, 37% had HS or less education, 70% married, and 33% with family incomes $26,000 or less. Nearly 50% of women were overweight or obese with a BMI of 25 or above, 60% reported alcohol use, and 22% reported tobacco use during 3 months before pregnancy. Oral health knowledge was high with 88% knowing that it was important to take care of their teeth and gums during pregnancy. Less than half (47.5%) of women reported that a health provider had talked with them about oral health during their most recent pregnancy (Table 1).
Characteristics of the 2012–2014 Virginia Pregnancy Risk Assessment Monitoring System Survey Population (n = 1344)
BMI, body mass index; HS, high school; SE, standard error.
In the stratified analyses, we found that the prevalence of a before pregnancy dental visit varied significantly by dental insurance status, race/ethnicity, education, marital status, family income, tobacco use, alcohol use, and oral health knowledge. Women who reported having dental insurance were more likely to have a dental visit before pregnancy (71%) compared with those who did not have dental insurance (26%). Among women who knew the importance of oral health, 60% had a dental visit compared with 27% who lacked oral health knowledge. Only 32% of Hispanic women had a before pregnancy dental visit compared with 64% NH white, 54% NH other, and 50% of NH black women. More than 75% of women who were highly educated and had higher family income had a before pregnancy dental visit compared with their less than HS educated (29%) and low-income (31%) counterparts, respectively (Table 2).
Distribution of a Before Pregnancy and During Pregnancy Dental Visit Among Virginia Women—Pregnancy Risk Assessment Monitoring System 2012–2014
Estimate is statistically unstable (denominator n < 50).
Oral health knowledge was determined by yes/no answer to following statement. “I knew it was important to care for my teeth and gums during my pregnancy.”
The prevalence of a dental visit during pregnancy varied significantly by dental insurance, race/ethnicity, education, marital status, family income, tobacco use, alcohol use, and oral health knowledge. Additionally, the prevalence of dental visit during pregnancy also varied by BMI, depression, diabetes, and oral health promotion by a health provider. Dental insurance was strongly associated with the dental visit during pregnancy, 64% of women with dental insurance had a dental visit during pregnancy compared with only 16% of those without dental insurance. One in every two women (51%) with oral health knowledge had a dental visit compared with one in five women who lacked oral health knowledge.
Overweight and obese women were less likely to have a dental cleaning during pregnancy compared with their normal weight counterparts (55% vs. 44%, respectively). The prevalence of dental visit during pregnancy was lower among women with diabetes (37.8%) or depression (35.6%) than among women without these conditions (no diabetes, 48.8%; no depression, 49.2%) (Table 2). Women who have spoken about oral health with their provider were much more likely to have a dental visit (78%) compared with those who did not (19%). Similarly, women who had a dental visit before pregnancy were more likely to have a dental visit during pregnancy (76% vs. 12%) (Fig. 2).
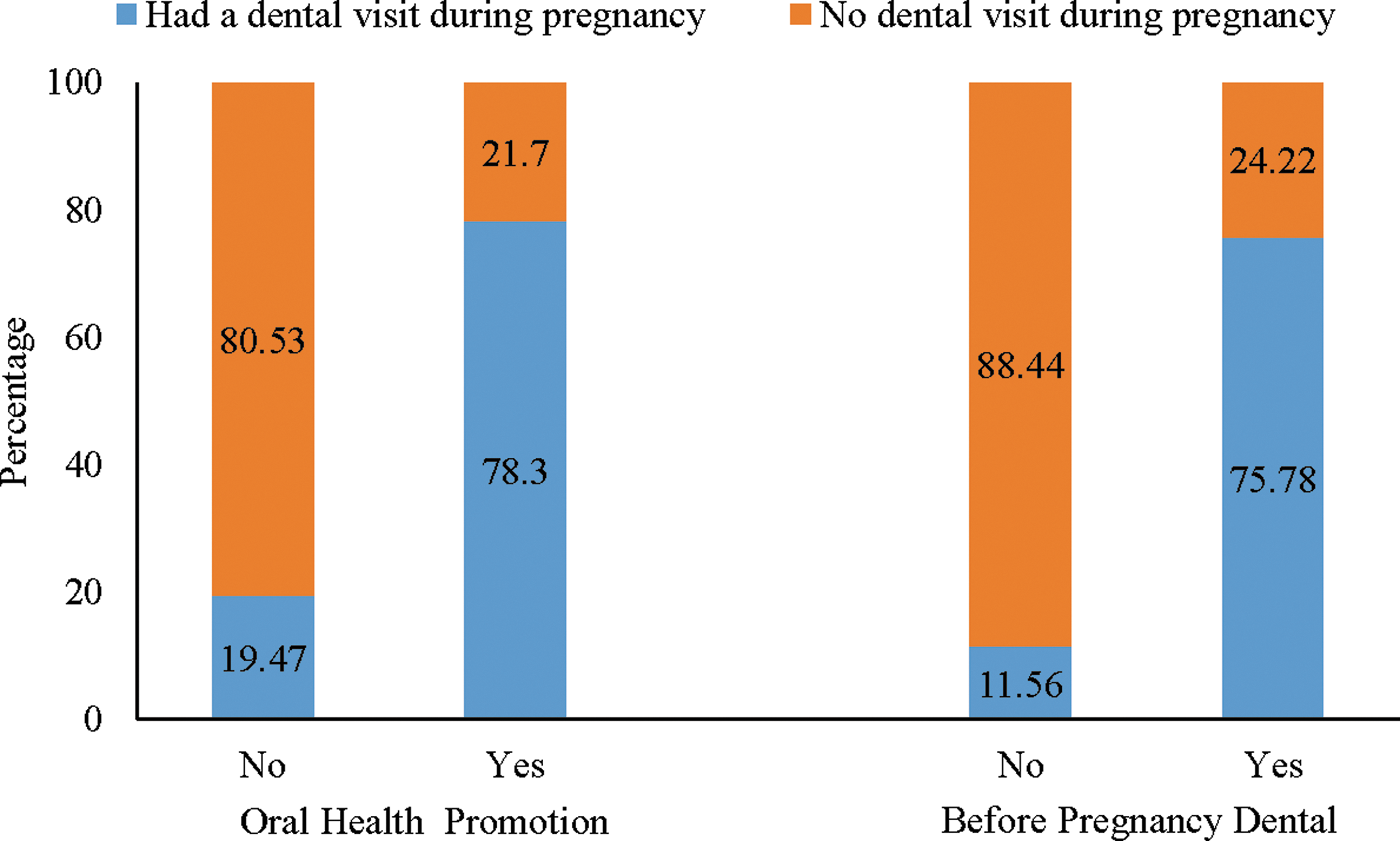
Distribution of a during pregnancy dental visit by oral health promotion and before pregnancy dental visit—Virginia PRAMS 2012–2014.a aBoth variables were statistically significant at p < 0.0001. Oral health promotion variable was based on yes/no answer to the statement, “A dental or other health care worker talked with me about how to care for my teeth and gums.”
Multivariate logistic regression models showed similar relationships for both outcomes. Before pregnancy dental visit was strongly associated with dental insurance, oral health knowledge, and family income after controlling for sociodemographic variables, health risk factors, and chronic conditions. Women with dental insurance had 3.5 times higher odds of a before pregnancy dental visit compared with those without dental insurance (OR = 3.5, 95% CI = 2.17–5.67). Being knowledgeable about oral health was associated with increased odds of a before pregnancy dental visit (OR = 2.79, 95% CI = 1.42–5.48). Women with higher family incomes had 2.4 times higher odds of dental visit compared with those with family incomes of $26,000 or less (Table 3).
Adjusted Multivariate Logistic Regression Models for a Before Pregnancy and During Pregnancy Dental Visit—Pregnancy Risk Assessment Monitoring System 2012–2014
Both models were controlled for age, marital status, alcohol use, tobacco use, diabetes, and hypertension.
Oral health knowledge was determined by yes/no answer to the statement, “I knew it was important to care for my teeth and gums during my pregnancy.”
Variables not included in before pregnancy dental visit model.
Oral health promotion variable was based on yes/no answer to the statement, “A dental or other health care worker talked with me about how to care for my teeth and gums.”
95% CI, 95% confidence interval; OR, odds ratio.
Dental insurance had a strong relationship with a dental visit during pregnancy and was associated with increased odds of a dental visit during pregnancy (OR = 5.79, 95% CI = 2.80–11.97). However, the most significant factor associated with a dental visit during pregnancy was a before pregnancy dental visit. Women who had visited a dentist 12 months before pregnancy had 20.7 times higher odds of visiting dentist during pregnancy (OR = 20.72, 95% CI = 11.14–38.54). Oral health knowledge was no longer significant in the adjusted model for a dental visit during pregnancy. However, oral health promotion by health provider was associated with increased odds of a during pregnancy dental visit (OR = 12.37, 95% CI = 7.31–20.93). Chronic conditions and health risk factors were associated with women's dental visit during pregnancy. Women with depression had 66% lesser odds (OR = 0.34, 95% CI = 0.14–0.81) compared with those without depression. Compared with overweight/obese women, normal weight women had twice the odds of a dental visit during pregnancy (OR = 1.95, 95% CI = 1.18–3.24).
Discussion
Among Virginia women, the prevalence of preventive dental visit during pregnancy and in the 12 months before pregnancy was low, 47% and 56%, respectively, during the 2012–2014 period. Dental insurance was strongly associated with a dental visit at both times. Beyond dental insurance, we found that a before pregnancy dental visit and oral health promotion by health provider were strongly associated with a dental visit during pregnancy.
The prevalence of dental care use among women varies depending on the data source, the population studied, and the life stage of women such as before or during pregnancy. According to 2011 PRAMS data, overall 43% of pregnant women had a dental cleaning visit during pregnancy, ranging from 31% in West Virginia to 50% in Massachusetts 18 and 43.6% in Virginia. 17 Given 2011 Virginia estimates, utilization of dental care among Virginia women during pregnancy increased during the 2012–2014 period. However, when data were examined by individual year, during pregnancy dental visits in Virginia showed significant declining trend during 2012–2014 (p < 0.001), with 49.6% in 2012, 48.1% in 2013, and 44.4% in 2014 (Fig. 1).
The 2004 PRAMS data from 10 reporting areas found the mean prevalence of a before pregnancy dental visit at 77.8% (range: 68.3% [Arkansas] to 84.2% [Vermont]). 19 We found that the prevalence of a pre-pregnancy visit was lower in Virginia compared with 2004 estimates from other states. Before pregnancy dental visits showed a decline from 2012 to 2013 (60.4%–53.7%), but the prevalence was relatively stable in 2013–2014 (53.7%–54%). We are not sure why dental visits declined during 2012–2014. To the best of our knowledge, there were no policy changes or change in questionnaire design that could have led to this declining trend in before and during pregnancy dental visits.
Consistent with other studies, 14,20,21 we found that dental insurance was positively associated with the use of dental services both before and during pregnancy. It is important to note that not all women who had dental insurance had a preventive dental visit before or during pregnancy, suggesting a complex interplay of various factors that inform health care utilization at different life stages. Previous studies have found disparities in dental care use by age, 14,22 race/ethnicity, 7,21 education level, 20,21 income level, 20,21 health risk factors such as smoking 7,23 and alcohol, 24 and marital status. 22 In this study, we found that associations of race/ethnicity and education with before pregnancy dental visit in multivariate models were marginally significant. This finding had a weak association in Virginia data compared with other states data. 7,19 One of the reasons for this finding could be different population characteristics in Virginia as well as small sample size.
Dental visit before pregnancy was associated with oral health knowledge and family income. Whereas a preventive visit during pregnancy was not associated with oral health knowledge or sociodemographic factors, but it was associated depression and BMI, both of which are common during pregnancy and are associated with severe health risks for the mother and child. 25 Pregnancy is a busy period in a woman's life with a lot of physiological and emotional changes that can overtake some of the women's personal health needs and care. 21,26,27 Women face additional barriers during pregnancy such as low priority for dental care and misconceptions about the safety or appropriateness of dental care, which may also explain some of these findings. 28 Association of depression and obesity with dental care use during pregnancy needs to be explored further as lower use of dental care among this high-risk group can further intensify the associated health risks.
We found that a before pregnancy dental visit was significantly associated with a dental visit during pregnancy. Women who had a dental visit before pregnancy were more than 20 times likely to have a dental visit during pregnancy. This association was found much stronger in this study than what other studies have reported previously. 20,21 One of the reasons for this strong relationship could be the improved knowledge and awareness about oral health from routine dental visits, which may reduce misinformation and myths around pregnancy and oral health. 28 Interventions to promote the use of routine dental care, improve oral health knowledge, and reduce barriers to access dental care among all childbearing age women can be useful in increasing the use of dental services during pregnancy.
Pregnancy is a great time to encourage and instill healthy behaviors as women are in touch with the health system through frequent prenatal visits. Studies have shown that a provider recommendation has a high influence on the use of health services and decreasing high-risk behaviors. 29 We had similar findings, oral health promotion by health providers had a substantial effect on a dental visit during pregnancy. This finding has several policy implications for health providers and policymakers. For the majority of women, health care providers such as obstetricians, gynecologist, nurse practitioners, and midwives are the more frequently seen health care professionals compared with dental providers. This creates unique and early opportunities for woman's health providers to educate and advise women about the importance of oral health through various life stages.
Studies show that many health professionals are aware of the importance of routine dental care during pregnancy, but often they do not address it. 30,31 Dental and national medical organizations such as the American Dental Association and the American College of Obstetricians and Gynecologists (ACOG) have provided clinical guidance and recommend oral health care during pregnancy. The ACOG guidelines suggest that the providers should conduct an oral health assessment, counsel women about the importance of dental care and good oral hygiene, and refer them to dental care providers for routine and needed care. 10 Collaborative models of care, effective communication, and consistent messaging from both dental and medical providers that oral health care and dental procedures are safe during pregnancy and that oral health care is a part of prenatal care can influence the use of dental services among childbearing age women. To the best of our knowledge, this is the first population-based study to examine the use of dental care before and during pregnancy among Virginia women, with a few limitations. First, all measures in this population survey data are self-reported and are subjected to recall and reporting bias. However, women completed these surveys within a few months of delivery, so recall bias should be minimal. Second, since the data are cross-sectional, we cannot derive causal inferences. For example, we do not know if the women talked about oral health care with their health provider first and then had a dental visit or vice versa or if a dental provider talked with them during the dental visit. The oral health promotion question combines dental and other health providers in the same question making it hard to determine which provider talked with them. Nevertheless, it is important to educate women about oral health and pregnancy and knowing that provider's recommendation has an influence on health care use is significant. Further research is warranted to understand the oral health recommendation practices among women's health providers in Virginia. Third, Virginia data from years 2012 to 2014 were not reported by CDC due to low response rates and small sample size. However, we overcame this limitation partially by combining 3 years of data and reporting combined estimates on a larger sample size with a comparatively smaller variance. In addition, Virginia PRAMS data are weighted to adjust for sample design, nonresponse patterns, and omissions from the sampling frame. Fourth, these data only include women who had live births and represent estimates on that population only. Finally, our findings are at the state level and therefore may not be generalizable to other states due to the difference in population characteristics, size, and local determinants. Despite these limitations, Virginia PRAMS 2012–2014 data provide rich and distinct information on the use of dental services among women before and during pregnancy along with its relationship with other factors.
To conclude, this study examined preventive dental care use among women during and before pregnancy. The study findings provide the VDH and other health policymakers with valuable information about the factors related with dental services use among women. Our results highlight the importance of resources such as dental insurance, oral health knowledge, and the strong association of oral health guidance and promotion by a health provider in increasing dental visits among women. Promoting and providing accessible and affordable preventive dental care to women before pregnancy can significantly improve dental visits during pregnancy. This information can guide future efforts and public health interventions to advance the oral health of pregnant women. Further research is needed to determine women's health provider practices in promoting oral health knowledge among childbearing age women.
Footnotes
Acknowledgments
This publication was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under award No. H47MC28478 for the Perinatal and Infant Oral Health Quality Improvement in the amount of $12,000 over 2 years with no funding from nongovernmental sources. This information or content and conclusions are those of the authors and should not be construed as the official policy of HRSA, HHS, or the U.S. Government, nor should any endorsements be inferred.
Disclaimer
The results and conclusions presented in this report are authors' views and do not represent official CDC or VDH position or opinion.
Author Disclosure Statement
No competing financial interests exist.