
Abstract
Introduction:
Dysmenorrhea (period pain) and associated symptoms are very common in young women <25 years. This time corresponds with a significant stage in adolescents and young women's academic lives at both school and in higher education. Dysmenorrhea may cause absenteeism from class or result in reduced classroom concentration and performance. Owing to cultural and economic differences, any impact may vary by country. This systematic review and meta-analysis examines the prevalence of dysmenorrhea in young women and explores any impact it has on their academic performance and other school-related activities.
Materials and Methods:
A search in Medline, PsychINFO, EMBASE, and Cumulative Index to Nursing and Allied Health Literature was carried out in June 2018.
Results:
Thirty-eight studies including 21,573 young women were eligible and included in the meta-analysis. Twenty-three studies were from low-, lower middle-, or upper middle-income countries, and 15 studies were from high-income countries. The prevalence of dysmenorrhea was high 71.1% (N = 37, n = 20,813, 95% confidence interval [CI] 66.6–75.2) irrespective of the economic status of the country. Rates of dysmenorrhea were similar between students at school (N = 24, 72.5%, 95% CI 67.5–77.0) and at university (N = 7, 74.9%, 95% CI 62.9–84.0). Academic impact was significant, with 20.1% reporting absence from school or university due to dysmenorrhea (N = 19, n = 11,226, 95% CI 14.9–26.7) and 40.9% reporting classroom performance or concentration being negatively affected (N = 10, n = 5126, 95% CI 28.3–54.9).
Conclusions:
The prevalence of dysmenorrhea was high, irrespective of country, with dysmenorrhea having a significant negative impact on academic performance both at school and during higher education.
Introduction
Menstrual disorders are highly prevalent among adolescent girls, and commonly feature period pain, fatigue, and mood changes. 1,2 Dysmenorrhea (period pain) affects around three quarters of all women during their reproductive life, and is especially common in young women in their teens and early adult life. 3
Primary dysmenorrhea is defined as menstrual pain in the absence of underlying pathology, with the pain commonly starting within 3 years of menarche (the first menstrual period) 4,5 and is the most common cause of dysmenorrhea in young women <25 years of age. 3 Secondary dysmenorrhea is menstrual pain associated with an identifiable cause. 6 The most common identifiable cause of secondary dysmenorrhea is endometriosis. 7
A previous systematic review describing the prevalence of dysmenorrhea in women during their reproductive lifespan reported rates ranging from 16.8% to 81%. 8 In 2010, a review of younger women <20 years of age found higher prevalence rates of 43%–91%. 9
Since the publication of earlier reviews, 8,9 there has been a significant number of observational surveys published. The majority of this literature is from low- and middle-income countries, where menstrual rates and the subsequent impact may be significantly different due to cultural taboos around menstruation and lack of support structures at school. This lack of support includes not being able to access facilities to change sanitary products without humiliation or embarassment. 10 Cultural and social factors are also likely to influence the prevalence and reporting of dysmenorrhea. 11 For instance, there is variance in the prevalence of dysmenorrhea reported in surveys between different cultural groups, even when geographical locations are similar. 12,13 It is currently unclear whether the differences in prevalence rates are due to biological or cultural factors; however, it is possible that the difference may be due, at least in part, to the presence of a public “culture of silence” around menstrual issues in some traditional cultures, demonstrated by women under-reporting primary dysmenorrhea in surveys, but showing similar rates across cultures in physicians' consultations. 11
The availability of new data from these countries may give more insight into the impact of menstruation worldwide. Previous studies have reported that among school-age adolescents and young women across a wide spectrum of social and cultural groups, dysmenorrhea causes educational absences, 13 –18 as well as reducing young women's capacities to concentrate, participate, and apply test-taking skills, thereby adversely impacting on overall grades. 16 It is often suggested that the severity of dysmenorrhea reduces with age, 19 so women at university may experience less negative impact than those at school; however, data on this comparison are currently lacking.
Owing to the potential impact that dysmenorrhea and the associated symptoms have on young women's academic performance at a critical stage in their academic lives, 17 an accurate understanding of the prevalence worldwide and how this affects young women in different countries are vital to identify the potential impact on young women's future prospects.
The aim of this systematic review and meta-analysis was to determine the overall rate of dysmenorrhea in young women globally and to explore the impact of dysmenorrhea on attendance and classroom performance at school, university, or other higher educational institutes. Furthermore, any differences in the prevalence and/or impact between countries with different economic status were explored.
Materials and Methods
Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were adhered to throughout this review. 20
Search strategy and selection criteria
A literature search was performed on Cumulative Index to Nursing and Allied Health Literature, Medline, Embase, and PsycINFO databases. All databases were searched from 1980 till June 1, 2018 using the following main keywords: “impact,” “symptoms,” “dysmennorhoea,” “adolescen*.” The search and selection process are outlined in Figure 1. The detailed search strategy is enclosed in Supplementary Data. Only English language articles published in peer-reviewed journals were included.
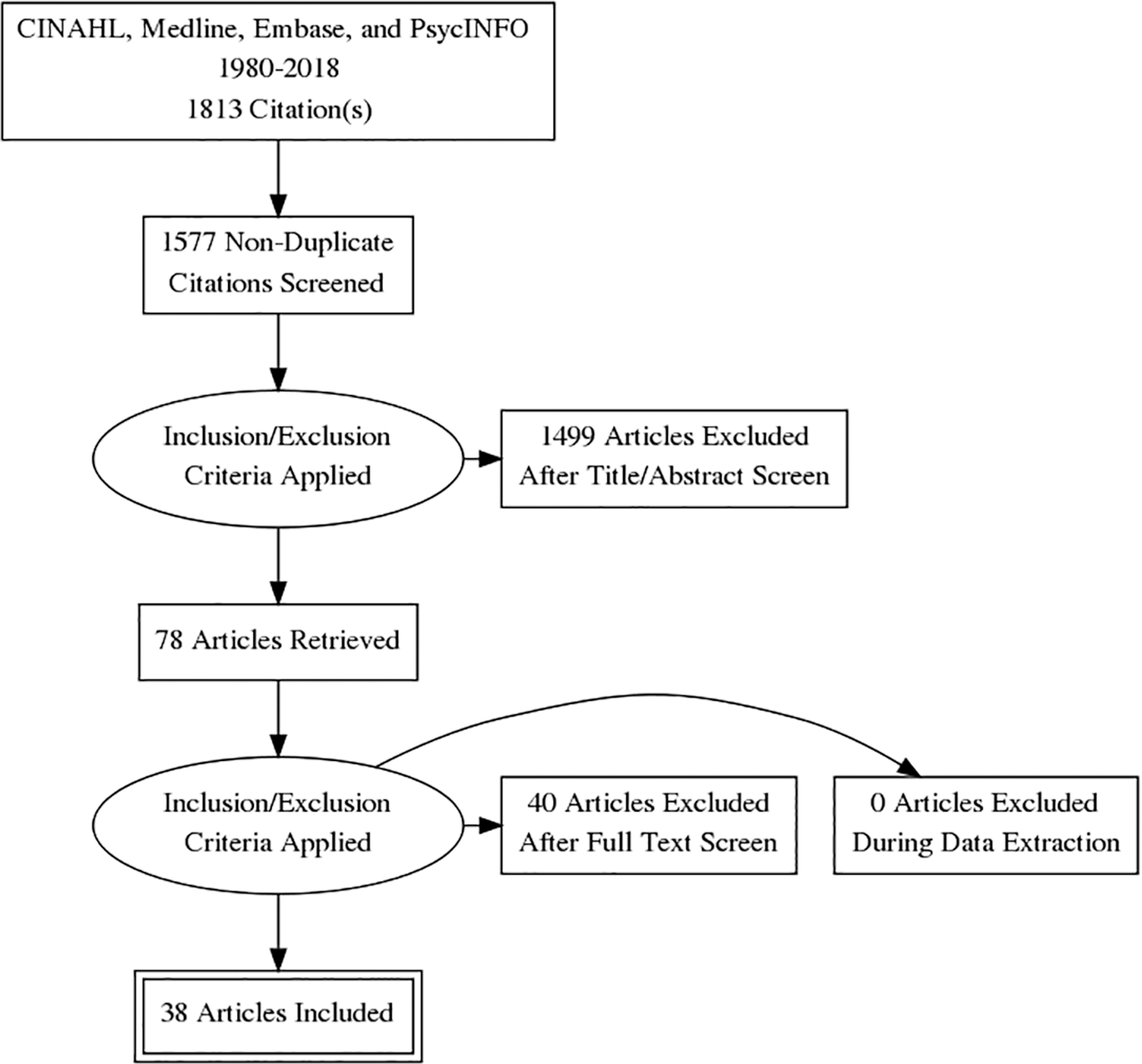
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Observational studies (including cohort, cross-sectional, and case–control) were included. Studies that specified that the participants were either at school or university or if the mean age of the young women in the sample was <18 years were included. Eligible studies were those that included either the outcome of prevalence of dysmenorrhea or academic absenteeism. Studies that reported on secondary dysmenorrhea only were excluded as these would not represent the true prevalence rate or impact of dysmenorrhea. Studies that only reported qualitative data were not eligible for inclusion.
Data extraction
Two authors (N.M. and M.A.) assessed eligibility, whereas three authors (M.A., N.M., and K.P.) and a research assistant (T.J.) extracted the data independently, and any disagreements were resolved by discussion. Where data were missing or unclear, the study authors were contacted via e-mail to request the data. Authors were contacted twice for a 6-week period, and if no response was received within that period, the data were marked as missing. A systematic tool for data extraction was developed to extract all relevant data from eligible studies. The tool is given in Supplementary Table S1.
Data were extracted on all of the following outcomes (if reported): Prevalence of dysmenorrhea. Severity of dysmenorrhea via numeric rating scale (NRS) or visual analogue scale (VAS). Symptoms of dysmenorrhea (bloating, emotional changes, fatigue, and breast tenderness). Absenteeism from school. Reduced classroom performance. Reduction in other school activities. Reduction in other social activities.
Study characteristics (location and demographics) were also extracted.
Quality assessment
Quality assessment of the included studies was performed independently and in duplicate by C.A.S., C.C., M.A., N.M., and K.P., with any disagreements resolved by a third party. Quality was assessed using a condensed version of the Strengthening the Reporting of Observational Studies in Epidemiology guidelines that have been used in previous reviews. 21,22
Data synthesis and meta-analysis
A random effects meta-analyses were conducted using Comprehensive Meta-Analysis software (Version 3). Data were pooled for each outcome where there were data from at least three independent studies.
A random effects model was used to account for expected heterogeneity between studies. Statistical heterogeneity between studies was quantified using Cochran's Q and I 2 statistic, both of which provide estimates of the degree of heterogeneity resulting from between-study variance, rather than by chance. Cochrane's Q with p-value of <0.05 was classified as significant heterogeneity, and I 2 of >75% was considered to indicate high-level heterogeneity, I 2 of 50%–75% as indicative of substantial heterogeneity, and an I 2 of <40% as low heterogeneity.
A priori mean age at the time of the survey was used in a meta-regression to explore any difference in dysmenorrhea rates with age. Preplanned subgroup analyses were conducted to examine whether there was a difference in prevalence or impact in high-income versus low-income, lower middle-income, and upper middle-income economies (as classified by the World Bank 23 ) due to differences in access to suitable medical and/or social support. A postori a subgroup analysis exploring prevalence and impact in students at school or university was undertaken.
Results
Thirty-eight studies with 21,573 young women were included in the meta-analysis. Figure 1 outlines the search and selection process. Nine studies were undertaken in Nigeria, 24 –32 four in Australia, 1,17,33,34 three in India, 35 –37 two each in Ethiopia, 38,39 Iran, 40,41 Taiwan, 42,43 and the United States, 16,44 and one each from Belgium, 45 Brazil, 46 Egypt, 47 Finland, 48 Ghana, 49 Hong Kong, 50 Italy, 51 Japan, 52 Malaysia, 53 Mexico, 13 Palestine, 54 Poland, 55 Sri Lanka, 56 and Turkey. 57 Study publication dates ranged from 1985 to 2018. Eighteen studies had publication dates in the past 5 years (from 2013 onward). The mean age of participants ranged from 1345 to 23 years, 49 with a median age of 17.15 years old at the time of the survey.
There were 23 studies from low-, lower middle, or upper middle-income countries (termed LMIC in the analysis) and 15 studies from high-income countries (termed HIC). Twenty-three studies reported on young women at school, nine reported on young women at university or higher education, one recruited from both school and university, and five recruited from a community population. Table 1 summarizes the included studies.
Characteristics of Included Studies
NR, not reported.
Quality assessment
The results of the quality assessment for the 38 studies are summarized in Supplementary Table S2. Seventeen studies clearly reported their eligibility criteria. Eighteen studies used a form of random sampling. Response rates ranged from 15.7% to 100%. Eight studies did not report response rates. Thirteen studies reported no conflict of interest, with one study reporting a potential conflict that was disclosed. Only six studies reported on the reliability and validity of their measures, with one additional study reporting that the questionnaire was validated but did not provide any details. Most studies used composite scoring methods, where a VAS or NRS was embedded as part of a larger questionnaire that had been developed by the authors, so although the VAR or NRS was valid and reliable, the rest of the questionnaire was generally not validated. All studies were susceptible to self-reporting bias.
Prevalence of dysmenorrhea
Across 37 studies with a total of 20,813 women, the overall prevalence of dysmenorrhea was 71.1% (N = 37, n = 20,813, 95% confidence interval [CI] 66.6–75.2, Q = 2344, p < 0.001, I 2 = 98.5). Figure 2 shows the forest plot for the complete data set. Subgroup analysis found there was no difference (p = 0.881) in the prevalence of dysmenorrhea between LMIC (N = 24, 70.6%, 95% CI 65.6–75.2) and HIC (N = 13, 73.2%, 95% CI 62.2–82.0), or between students at school (N = 24, 72.5%, 95% CI 67.5–77.0) and university (N = 7, 74.9%, 95% CI 62.9–84.0). There was no effect of age at the time of the survey on the prevalence of dysmenorrhea (β = 0.0874, Z = 1.45, p = 0.1245).
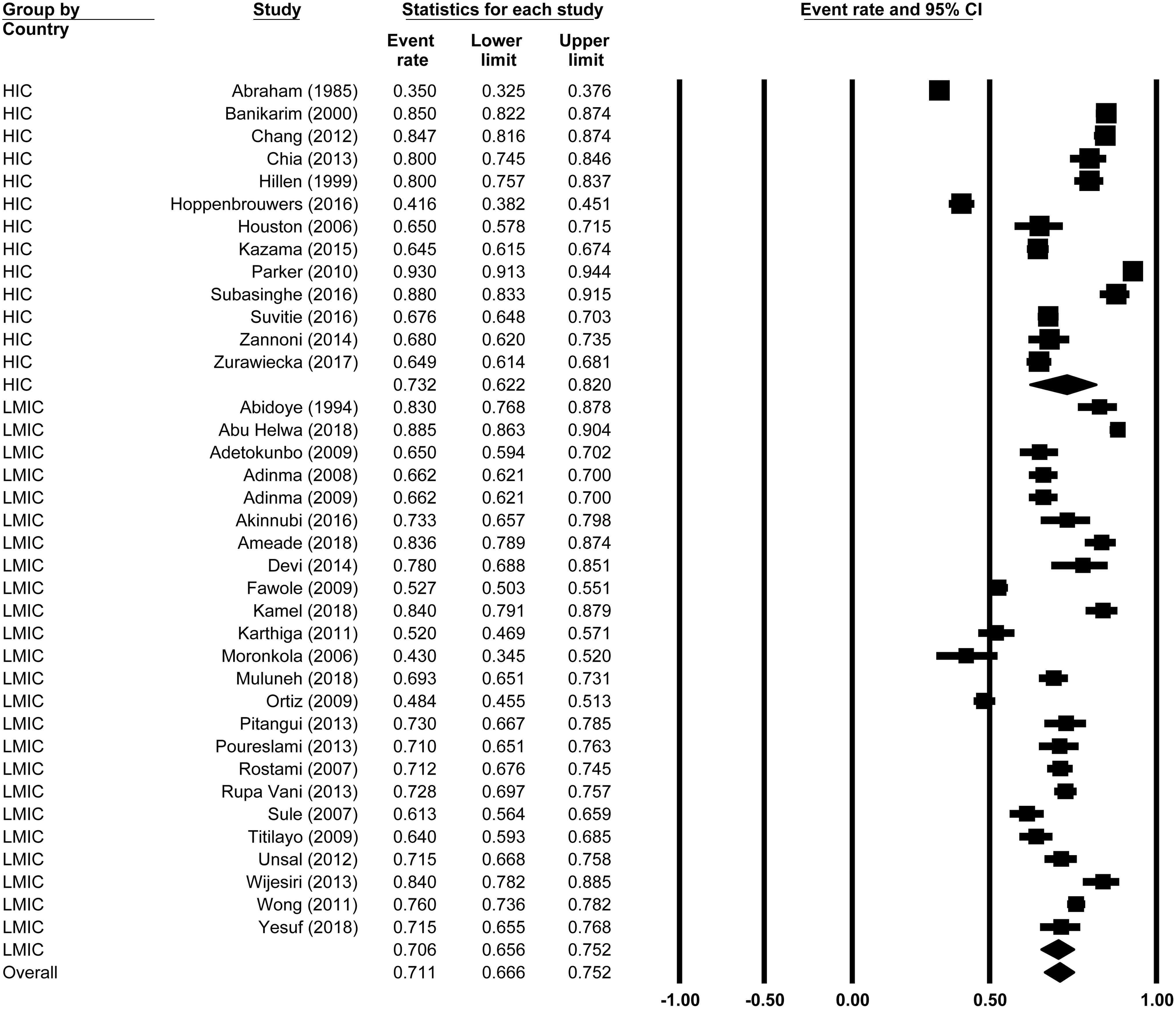
Prevalence of dysmenorrhea.
Severity and symptoms of dysmenorrhea
Complete data on dysmenorrhea severity measured via an NRS or VAS were only reported in three studies and were, therefore, not included in the analysis. Secondary symptoms of dysmenorrhea were very common, with 48.3% of women reporting one or more of emotional changes, breast tenderness, bloating, or fatigue (N = 33, n = 16,178, 95% CI 39.4–57.3, Q = 3112, I 2 = 98.97, p < 0.001). Bloating was the most commonly reported symptom, with 56.3% of women reporting this symptom (N = 6, n = 3381, 95% CI 42.5–69.1, Q = 251, I 2 = 98.0, p < 0.001), 56.0% reported breast tenderness (N = 6, n = 2038, 95% CI 25.2–82.8, Q = 616, I 2 = 99.2, p < 0.001), 44.0% reported fatigue (N = 12, n = 6671, 95% CI 42.5–69.1, Q = 1245, I 2 = 98.0, p < 0.001), and 34.6% reported emotional changes (N = 8, n = 3381, 95% CI 18.7–54.9, Q = 932, I 2 = 99.1, p < 0.001). Figure 3 shows the forest plot for all secondary dysmenorrhea symptoms.

Prevalence of secondary symptoms of dysmenorrheal; bloating, breast tenderness, emotional changes, and fatigue.
Educational impact
Across 19 studies with a total of 11,226 women, 20.1% were absent from school or university due to dysmenorrhea (N = 19, n = 11,226, 95% CI 14.9–26.7, Q = 987, I 2 = 98.2, p < 0.001). Subgroup analysis showed there was a trend (p = 0.061) toward a greater percentage (26%) of young women taking time off school in LMIC (N = 10, 95% CI 16.8–32.1, Q = 403, I 2 = 97.7, p < 0.001) compared with HIC at only 12.1% (N = 9, 95% CI 6.2–22.2, Q = 574, I 2 = 98.6, p < 0.001). There was no difference (p = 0.432) in absenteeism between young women at school (N = 10, 18.2%, 95% CI 11.6–27.5) and at university (N = 5, 23.5%, 95% CI 14.4–35.9).
Overall 40.9% of young women reported classroom performance or concentration being negatively affected (N = 10, n = 5126, 95% CI 28.3–54.9, Q = 743, I 2 = 98.8, p < 0.001, 10 studies, 5126 women). There was no difference (p = 0.789) between classroom performance being affected in LMIC (37.6%, 95% CI 24.0–53.4) and HIC (52.4%, 95% CI 25.6–77.9) or between (p = 0.878) young women at school (N = 4, 44.8%, 95% CI 22.8–69.0) and at university (N = 6, 42.4%, 95% CI 25.3–61.5). Reduction in other school activities was reported by 29.6% of young women (95% CI 15.6–48.8, Q = 561, I 2 = 98.9, p < 0.001, 7 studies, 3524 women). There were not enough studies reporting this outcome to perform either subgroup analysis.
Other impact
Reduction in “other activities” such as social or sporting activities was reported by 37% of young women (95% CI 24.2–50.7, Q = 2533, I 2 = 99.4, p < 0.001, 15 studies, 13,306 women). There was no difference (p = 0.593) in reduction in other activities between LMIC (40.5%, 95% CI 24.1–59.3) and HIC (34%, 95% CI 20.1–51.1).
Discussion
Prevalence of dysmenorrhea, regardless of the economic status of the country, was high, with more than two-thirds (70.8%) of young women reporting the presence of dysmenorrhea, regardless of geographical location. The LMIC subgroup included countries such as Sri Lanka, Nigeria, and India, where menstrual taboos are more prevalent 58 –60 and, therefore, reporting rates on menstruation and related issues is expected to be lower due to stigma, shame, or misinformation. However, despite these expected differences in reporting, there was no difference in overall prevalence rates between HIC and LMIC. This suggests that strategies to assist young women in managing dysmenorrhea are as important in HIC as in LMIC.
Most studies did not provide the definition they used for dysmenorrhea, and this is likely to, at least in part, explain the varying rates of dysmenorrhea between surveys. 14,61 A common theme regardless of geographic areas or cultures 16,62 is that most young women think period pain is a normal part of becoming a woman. 63 Additionally many young women were unable to identify the symptoms of dysmenorrhea. 28 Therefore, given the normalization of pain by young women, surveys that did not provide a definition of what constitutes dysmenorrhea (e.g., pain in the lower abdomen just before or during menstrual bleeding) may have resulted in an underestimate of the prevalence of dysmenorrhea in this meta-analysis. This is due to potential misunderstandings of how much pain is “normal” and, therefore, not worth reporting.
The severity of menstrual pain was not consistently reported, with only three articles reporting dysmenorrhea scores via a VAS or NRS, with the remainder using “mild, moderate, severe” or some variation thereof. This classification system is not unusual as clinicians tend to use a scale of mild, moderate, or severe depending on how daily living is impacted, 64 and there are prespecified scales using this criterion. 65 However, the definition of pain scores that were classified into these three groups was not consistently applied and this prevented meaningful comparisons between studies. Reporting of secondary symptoms was more consistent, and very common, with almost half (48.3%) of young women reporting secondary symptoms. Future studies should endeavor to use a standard self-report scale such as a VAS or NRS for pain to allow comparison between populations.
The impact of menstrual symptoms on education was significant, with around one in five young women (20%) being absent and 40% reporting that classroom performance (such as concentration levels or test-taking abilities) had been negatively affected. This illustrates that girls and young women may be significantly disadvantaged in their studies by the impact of dysmenorrhea. Hillen et al. succinctly sum up the possible impact of these academic restrictions on young women, stating that “School attendance and ability to concentrate on studies in Grades 11 and 12 are vital, as achievement in these high school years has significant long-term consequences for an individual.” 17 Our subgroup analysis suggests that this negative impact starts at school and continues relatively unchanged when young women progress to university/tertiary education. Previous systematic reviews on dysmenorrhea have suggested that as women age, the prevalence of dysmenorrhea decreases, 15,66 Latthe et al. found dysmenorrhea prevalence decreased with age, but in their review the subgroup analysis was age >30 years compared with age <30 years. 15 Our findings do not support any significant reduction in prevalence with increasing age in this younger population, where the majority of women were <25 years. It is also important to note that the severity of dysmenorrhea does not appear to reduce significantly over time, even after age 25 years, 67 and a significant proportion of women with severe dysmenorrhea may go on to develop more persistent pelvic pain symptoms. 68
These findings also have implications for teachers, curriculum, and pedagogy. Teachers, particularly health educators, need to have knowledge about dysmenorrhea to be able to educate young women about the condition and provide appropriate suggestions for material and emotional support. Although apparent in the syllabus, teachers may or may not address the topic adequately or, in some instances, at all. As Duffy et al. found, teachers, particularly in primary school education, demonstrate little confidence in teaching about “sensitive” topics, including menstruation. 69 Dysmenorrhea is, therefore, likely to be omitted from classrooms, disadvantaging the young women who experience the condition and reinforcing its invisibility in learning contexts. Thus, awareness needs to be raised in teacher education courses and professional learning provided for current teachers. Greater explicitness is required within school curriculum documentation to increase awareness and ensure the topic is adequately addressed. In addition, enhancing teacher awareness generally may have implications for pedagogy; that is, teachers need to provide young women who have missed lessons or who have poorly absorbed information due to the symptoms of dysmenorrhea, opportunities for additional pedagogical support. Even simple accommodations such as allowing more time during tests or extensions on the submission dates of tasks may be useful and contribute to a more equitable learning environment.
Other activities either directly school-related (such as sports) or social activities were also commonly affected in around a third of young women. Although there was no significant difference between absenteeism in LMIC and HIC, the trend toward greater absenteeism in LMIC found in the data may reflect the possibility that women in LMIC could be missing school not necessarily due to pain alone, but rather due to lack of sanitary products needed for menstrual management. 10 Once again, schools could provide support through on-going and targeted programs to provide sanitary products and information on effective pain management options such as ibuprofen or other nonsteroidal anti-inflammatory drugs (NSAIDs), 9,70 and, where appropriate, NSAIDs could be dispensed in line with school policy and parental consent. This is especially important for disadvantaged young people to ensure that they have the means to manage their period, and in doing so, continue to attend school and avoid absenteeism on this basis.
There are a number of strengths in this systematic review and meta-analysis. We searched for articles across a range of databases and used dual data extraction via a prespecified data extraction form to ensure rigorous data collection. Decisions on how to determine a country's status used the four tier World Bank system 23 rather than the more simplified “developing” or “developed” bipartite classification. There are a number of limitations that must be acknowledged. First, we did not search in languages other than English, so there may be a number of non-English language articles that were not included. Second, studies often did not provide the definition of dysmenorrhea that they used in the study, so there may be variations between studies in what is classified as dysmenorrhea. Third, the majority of studies did not report the recall period of the survey, if questions were related to experiencing dysmenorrhea at any time since menarche or if this was during a defined time period (e.g., in the past 6 months). Therefore, although we can be confident in the overall prevalence, we cannot be certain how frequently young women experience those dysmenorrhea symptoms, and this may over or underestimate the impact depending on how long the time period was. Fourth, the educational impact may be underestimated as women with severe pain may have dropped out of school or tertiary education and not been included in surveys undertaken in those locations, so although there were a number of community-based surveys that did ask about academic impact, it is possible that the overall academic impact may be more severe than reported. Fifth, secondary symptoms for dysmenorrhea are wide ranging and only a selection of the more common symptoms was included in this meta-analysis. This may not represent all the comorbid symptoms experienced by these girls—for example, menstrual headache, the stabbing pains consistent with pelvic muscle dysfunction, or bowel symptoms. Further studies could include assessment of a wider range of symptoms to ensure even better relevance to girls' needs. Finally, the quality of the studies tended to be low, with a lack of clear inclusion criteria and measures that were susceptible to self-report bias.
Conclusions
The prevalence of dysmenorrhea among young women is consistently high and unrelated to the economic status of their country. The consequences are that a significant number of young women regularly miss school or university or, if present, have their academic performance impaired. Considering the timing of this impact, it is crucial that the negative influence of dysmenorrhea is reduced as much as possible. Future research should focus on strategies to improve pain and symptom management with the aim of reducing the impact of dysmenorrhea so that young women can optimize their educational opportunities and future life chances.
Footnotes
Acknowledgments
Thummini Jayasinghe (T.J.) and Zelalem Mengesha are thanked for helping with the search strategies.
Author Disclosure Statement
M.A., K.P., and C.A.S.: As a medical research institute, NICM Health Research Institute receives research grants and donations from foundations, universities, government agencies and industry. Sponsors and donors provide untied and tied funding for work to advance the vision and mission of the institute. This study was not specifically supported by donor or sponsor funding to NICM. All other authors have no competing financial interests exist.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.