
Abstract
Background:
To investigate the hypothesis that increased uptake of long-acting reversible contraception (LARC) by women played a role in the declining abortion rates observed in New Zealand between 2008 and 2014.
Materials and Methods:
This quantitative ecological study analyzed routinely collected national data pertaining to abortion numbers, contraceptive prescriptions, and census population estimates for the period 2004–2014. Annual prescription and prevalence rates (per 1000 women) were calculated for short- and long-acting methods to investigate changes over time. Poisson's regression was used to (1) test whether the abortion rate changed by year; (2) whether 2010 (when the contraceptive implant became subsidized) was a significant point of change; and (3) test the relationship between declining abortions and patterns of contraceptive use.
Results:
Estimated LARC prevalence increased from 2009 to 2014, with a corresponding decrease observed in prescription of short-acting methods. The declining abortion rate accelerated each year from 2008 to 2014 (with a faster decline from 2010 to 2014), but 2010 was not a significant point of change. Three factors had statistically significant associations with declining abortion rates (p < 0.01): year (acting as a surrogate for all social changes), women's use of the levonorgestrel (LNG)-implant, and the combined model: use of the LNG-implant and copper intrauterine device (CuIUD) had the best fit (using Akaike's Information Criterion), indicating that this variable explained more of the year-to-year variability in abortion rates.
Conclusions:
The shift toward women's increased use of the two publically funded LARC methods (LNG-implants and CuIUD) was significantly associated with the declining abortion rates in New Zealand.
Introduction
New Zealand experienced a historically unprecedented decline in the abortion rate between 2008 and 2014. In 2007, the abortion rate peaked at 20.1 per 1000 reproductive-aged women, but by 2014 it declined to 14.4 per 1000. 1 The decline in abortion rates between 2007 and 2014 has been particularly marked in the youngest age groups; abortion rates almost halved for 15- to 19-year olds, and reduced from 37.6 to 25.2 for 20- to 24-year olds. 2
Declining rates of abortion have also been reported in the United States and the United Kingdom over this period of time. 3,4 Internationally, the increased use of long-acting reversible contraceptive (LARC) methods has been recognized as having played a role in declining abortion rates. 5 Women can more easily avoid or space their pregnancies by using long-acting contraception, in turn reducing their likelihood of unintended pregnancies that may end in an abortion. The benefits of LARC methods are well recognized and include high effectiveness, reversibility, no need for daily adherence (“fit-and-forget”), ability to space pregnancies, choice of hormone or nonhormone containing methods as well as high user continuation and satisfaction rates. 6 –9
There is now a wealth of clinical evidence indicating immediate postabortion insertion of a LARC method significantly reduces the chances of a subsequent abortion. 10 –14 Several studies have also replicated these findings at a population level—the Contraceptive CHOICE project in the United States provided clear evidence that promoting widespread access to and women's choice of LARC methods in an area reduces the abortion and teenage pregnancy rates in that area. 15 Research in the United Kingdom involving analysis of teenage conception rates and age-specific abortion rates found that use of LARC by women <20 years was associated with declining abortion rates, but no association was observed for other age groups. 16 A recent time-series analysis in Finland for the period 2000–2015 found that subsidization of long-acting contraceptive methods in 2013 significantly increased women's use of LARC, in turn coinciding with reduction in abortion rates, especially among those aged 15–19 years. 17
In New Zealand, there are two LARC methods subsidized by the government that are available to women at no or low cost: the copper intrauterine device (CuIUD) and the two-rod levonorgestrel-releasing subdermal implant (LNG-implant). While the CuIUD has been available as a subsidized (publically funded) contraceptive in New Zealand since 1994, the LNG-implant only became subsidized in 2010 (2 years after the abortion rate began to decline). Once subsidized, the implant became more widely available and was immediately a popular contraceptive choice for women. 18
The levonorgestrel intrauterine system (LNG-IUS) is subsidized only for women meeting specific criteria with very heavy menstrual bleeding but not for contraceptive use (so costs upward of NZ$340). 19 Depot medroxyprogesterone acetate (DMPA) is available at low cost but is not considered a LARC in this study due to its lower continuation rates and higher pregnancy rates when compared with intrauterine methods and implants. 6 Shorter acting methods including the combined oral contraceptive pill (OCP) and male condoms are also government subsidized in New Zealand, so available at low or no cost. 19
No research has investigated determinants of the decreasing abortion rate in New Zealand, although there has been speculation that increased use of LARC methods has played a role. 1,20,21 Abortion is accessible to most women up to 20 weeks gestation in New Zealand. However, women must be referred to an abortion service by a general practitioner or family planning clinic, and two doctors must certify the grounds for the abortion (most often that continuing the pregnancy would result in a serious risk to the physical or mental health of the woman), as specified in the Crimes Act 1961. 22
This study had three main objectives: (1) to estimate the changing prevalence of contraceptive methods used between 2008 and 2014 (long- and short-acting methods); (2) to explore the timing of changes in the abortion rate to determine whether the rate of decline of abortion was greater from 2010 to 2014 (after the subsidization of the LNG-implant) than it was from 2008 to 2010; and (3) to investigate whether changing patterns of LARC use were associated with the decreasing abortion rate.
Materials and Methods
Study design and population
This research used a quantitative ecological design utilizing routinely collected national data on contraceptive prescriptions and abortion rates for women in New Zealand for the period 2004–2014.
Data collection
Data for numbers of contraceptive units prescribed to women annually were obtained from the national database held by the New Zealand Ministry of Health that included prescriptions for the LNG-IUS and CuIUD for the years 2000–2014; the oral emergency contraceptive pill (ECP); OCP (progesterone only and combined); and DMPA for the years 2004–2014. Data for the LNG-implant were included only for the years 2010–2014 (it was not widely available before 2010).
Population estimates were obtained for women aged 15–44 for the years 2004–2015 from the Statistics New Zealand website. 23 Deidentified data collected for all abortions performed in New Zealand are national statistics provided in annual reports prepared by Statistics New Zealand. 1 Data on the annual number of abortions were obtained for the period 2004–2014 from the Statistics New Zealand website. 2 Male condom data were not used because although condoms are available through prescription, they are also widely available through retail stores, and therefore the prescription data are not representative of condom use.
Age data were available only for the LNG-implant and LNG-IUS but not for the other contraceptive methods studied, so age could not be included as a factor in our analyses.
Ethical approval was granted by the Human Ethics Committee at the University of Otago, New Zealand, to obtain and analyze routinely collected deidentified abortion, prescribing, and demographic data.
Data preparation
The three LARC methods available in New Zealand during the study period—the LNG-implant (Jadelle® Made in Finland for Bayer NZ Limited, Auckland, New Zealand), CuIUD (Multiload Cu375; Merck, Sharpe & Dohme, Auckland, New Zealand), and LNG-IUS (Mirena®; Made in Finland for Bayer NZ Limited) were each approved for a 5-year duration of action. Estimated duration of use (prevalence) was therefore calculated for each LARC method between 2004 and 2014, using removal rates obtained from the available literature (Supplementary Table S1).
The Multiload Cu375 and Jadelle LNG-implant are not widely used internationally, so only four clinical trials were found for the Multiload and three trials for Jadelle. These trials had limited follow-up periods, so clinical trials reporting removal rates for the Nova-T Copper IUD and Norplant LNG-implant were used to create removal rates for the fourth and fifth year. 25 From this, an estimated prevalence of usage was obtained for each method.
Prevalence estimates for the two funded methods (the LNG-implant and CuIUD) were also combined to create a single combined estimate “LNG-implant and CuIUD.” The LNG-IUS was not included in a “total LARC” measure due to its high cost (except when prescribed for the management of heavy menstrual bleeding) and use predominantly by older women (40–44 years), for whom the abortion rate did not change significantly for the period studied.
Statistical analyses
Patterns of contraceptive use in New Zealand (2004–2014)
Estimated prevalence rates were created for LARC methods by dividing the estimated prevalence of each LARC method by the population of women aged 15–44 years. The estimated prevalence rates for the CuIUD, LNG-IUS, and LNG-implant and prescription incidence rates for the OCP, ECP, and DMPA were graphed for the years 2004–2014.
Changes in the abortion rates (2008–2014 and 2010–2014)
To determine whether the abortion rate changed after the subsidization of the LNG-implant in 2010, two Poisson's regression models of abortion rates by year were fit: the first described the association from 2008 to 2014, and was compared with the association from 2010 to 2014. A regression with a Poisson distribution was designed to test association between a dependent variable and independent variables for count data. Analyses were performed using SPSS (version 23, IBM Corp., 2013). 26
Quadratic and linear relationship between “year” and abortion (2004–2014)
A quadratic model in time (year) was used to test whether the abortion rate accelerated over time. If the linear effect of time alone is significant, it indicates that the rate of decrease is the same across the years; however, if the quadratic term (the term in year 2 ) is significant, the rate of decrease is increasing over time. To compare how well the linear and quadratic models fit the observed data, the predicted number of abortions for each year was calculated from each model. Pearson's correlation was calculated to test whether the quadratic model or the linear model gave predicted numbers of abortions that were more closely correlated with observed numbers of abortions.
Association between contraceptive incidence, prevalence, and abortion rates
To investigate the relationship between patterns of contraceptive methods prescribed to women and abortion rates, separate Poisson's regression models were used to identify any associations between incidence or prevalence of each contraceptive method and the declining abortion rate.
First, “year” was used as a surrogate measure for the total change in all social, economic, and/or cultural changes that may have driven changes in abortion rates over a given period of time. “Year” was tested as a predictor of the abortion rate for the periods 2004–2014 and 2010–2014, with comparisons made for each contraceptive method to determine whether incidence or prevalence of the method was able to explain the abortion rate better than “year.” A separate model for each contraceptive method was fit to predict the number of abortions by year. Data for the CuIUD, “LNG-implant and CuIUD,” LNG-IUS, ECP, DMPA, and the OCP were fit for 2004–2014. The LNG-implant was fit for the years 2010–2014.
Akaike's Information Criterion (AIC) 24 is a comparative measure, which assesses the fit of a model. AICs for year were used as a comparison for each contraceptive measure; a smaller AIC value indicates a better fit. Due to large populations (denominators) and comparatively small numbers of contraceptive prescriptions and abortions (numerators), the coefficients, which usually signal the strength of a relationship, were very small. In this study, focus was placed on the direction of the coefficients, indicating a positive or negative association between the contraceptive method and abortion rates. p-Values were also examined to determine the statistical significance of the relationship. p-Values of <0.01, indicating a <1% likelihood that the result is due to chance, were considered as significant in this study.
Results
Patterns of contraceptive use in New Zealand (2004–2014)
Figure 1 presents the estimated national prevalence rates for long-acting methods and prescription rates for short-acting methods for the period 2004–2014. The figure shows that the estimated prevalence of the LNG-implant increased steadily from 3.77 per 1000 women in 2010 to 17.25 per 1000 women in 2014. The estimated prevalence of LNG-IUS also increased from 2.48 per 1000 women in 2004 to 43.71 per 1000 women in 2014. By contrast, the estimated prevalence of the CuIUD fluctuated over time. Prescriptions for the OCP decreased from 225.7 per 1000 women in 2004 to 200.13 per 1000 women in 2014. ECP also decreased over this time period from 176.29 per 1000 women to 48.48 per 1000 women from 2004 to 2014. Prescriptions of DMPA decreased from 174.2 per 1000 women in 2004 to 160.63 in 2014, with fluctuation in intervening years.
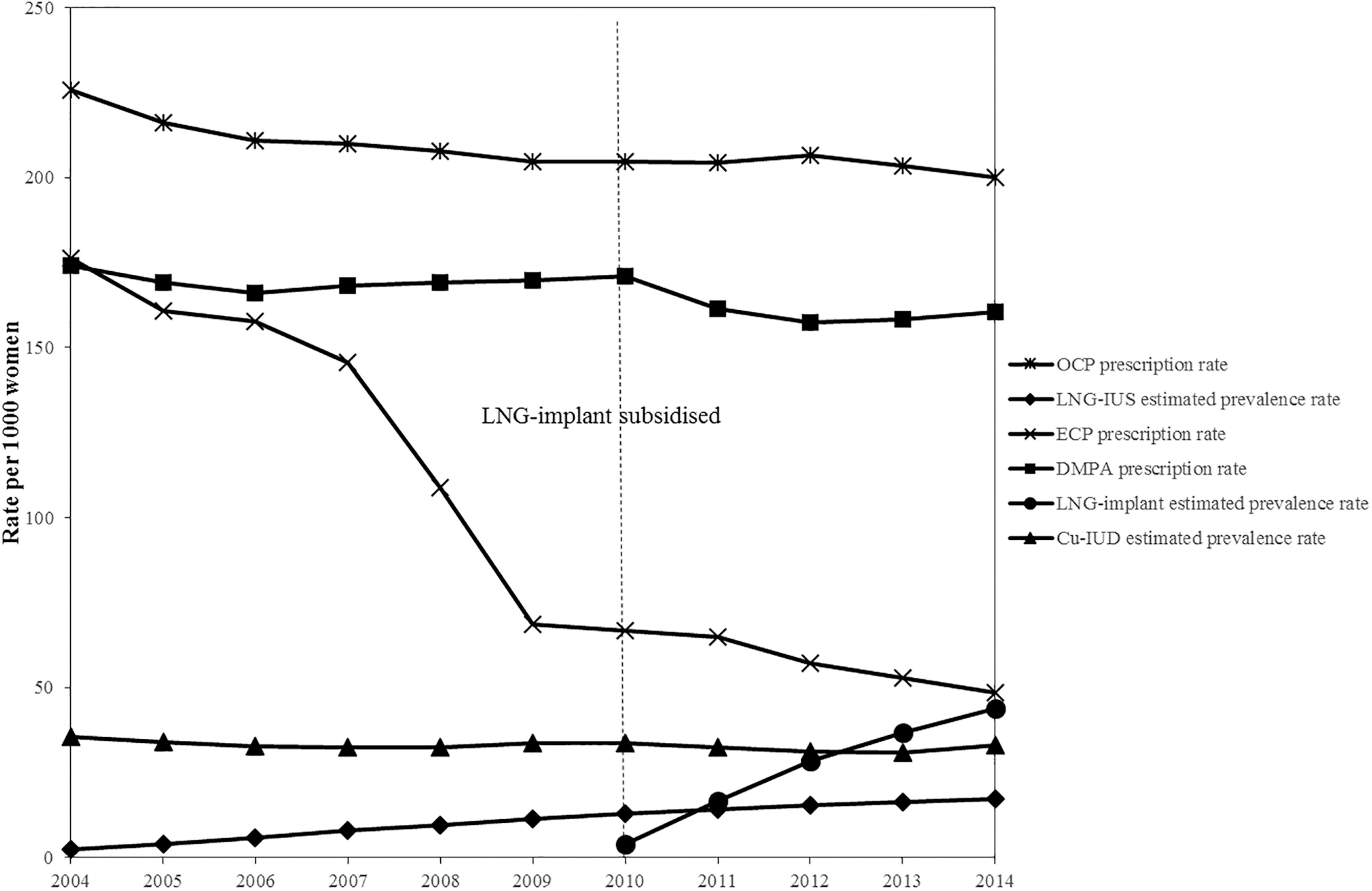
Estimated prevalence rates (per 1000 women) of long-acting reversible contraceptive methods and prescription rates (per 1000 women) for short-acting contraceptive methods in New Zealand from 2004 to 2014.
A review of data for the LNG-implant and LNG-IUS revealed a clear age gradient for both methods—LNG-implant use was highest among 15–19 and 20–24 year olds with declining prescription numbers observed in older age groups. Conversely, LNG-IUS use was highest among 40- to 44-year olds with lower levels of use in younger age groups.
Changes in the abortion rate (2008–2014 and 2010–2014)
A Poisson regression using year to predict abortion rates before and after 2008 was compared with a Poisson regression using year to predict abortion rates before and after 2010. Results showed that the decrease in the abortion rate from 2008 to 2014 (B = −0.0528, 95% confidence interval [CI] = −0.056 to −0.0498, p < 0.01) was slightly weaker than the yearly decrease from 2010 to 2014 (B = −0.0587, 95% CI = −0.0638 to −0.0537, p < 0.01). This implies that the rate of decrease in abortions was higher from 2010 to 2014.
Quadratic and linear relationship between “year” and abortion (2004–2014)
Table 1 presents the results of the Poisson regression analysis conducted to determine whether the decreasing abortion rate was linear or quadratic using both year and year 2 to predict abortion over the full time period. The decrease in the abortion rate was best described by a quadratic rather than a linear model, as it had a better fit (lower AIC). Pearson's correlation was used to compare the predicted abortion numbers from each model with observed abortion numbers. The predictions from the quadratic model had a higher correlation (r = 0.99, p < 0.01) than the linear model (r = 0.90, p < 0.01).
Poisson's Regression for Quadratic and Linear Relationship Between “Year” and Abortion
Denotes statistical significance.
95% CI, 95% confidence interval; AIC, Akaike's Information Criterion (a smaller AIC indicates a better fit); B, beta coefficient; SE, standard error.
Association between contraceptive prevalence and abortion rates
Table 2 presents the results of the Poisson regression analyses used to test for associations between contraception prevalence and abortion rates. The models for each contraceptive method were compared with that for year alone. The association of the abortion rate and “year” for 2010–2014 had an AIC of 63.73, and the association of the abortion rate and “year” for 2004–2014 had an AIC of 542.25. Based on data from 2010, as the estimated prevalence of LNG-implant use increased, abortion rates decreased (p < 0.005); however, the fit of the model was poor with an AIC of 78.46 (higher than the AIC of 63.73 for year 2010–2014). Similarly, as the estimated prevalence of the LNG-IUS increased, abortion rates decreased (p < 0.01), but with a poorly fitting model with an AIC of 700.60. Estimated prevalence of the LNG-implant and CuIUD as a combined variable was negatively associated with abortion (p < 0.01)—as use of both these methods increased, abortion rates declined. This model was a better fit with an AIC of 209.79, suggesting that together, changing prevalence in both of these methods explained more of the year-to-year differences in abortions than the measure year (acting as a surrogate for societal and other changes over time).
Results of Separate Poisson's Regression Models Testing for Associations Between Year, Patterns of Contraceptive Use, and Abortion Rates
Denotes statistical significance.
CuIUD, copper intrauterine device; DMPA, depot medroxyprogesterone acetate; ECP, emergency contraceptive pill; LNG, levonorgestrel; LNG-IUS, levonorgestrel intrauterine system.
Positive associations were found between abortion and DMPA prescription rates (p < 0.005), the OCP prescription rate (p < 0.01), and the ECP prescription rate (p < 0.01). As prescription rates for these methods decreased, so too did abortion rates.
Discussion
The estimated prevalence of LARC methods used by women increased from 2009 to 2014, and a corresponding decrease was observed in the prescription of short-acting contraceptive methods during this period. The decline in New Zealand's abortion rate accelerated each year from 2008 to 2014, but the year 2010 was not a significant point of change.
When considered as a separate factor, LNG-implant prevalence was significantly associated with declining abortion rates; however, it did not explain as much of the year-to-year variability in abortion rates as did year by itself (acting as a surrogate for societal and other changes over time). When considered as a combined variable, the prevalence of the LNG-implant and CuIUD was significantly associated with declining abortion rates and explained more of the year-to-year variability in abortion rates than year alone did. This suggests that together, prevalence of the two funded LARC methods was better at explaining the decline in the abortion rate than the LNG-implant alone, suggesting that these may have been competing methods.
This research was the first attempt to examine potential explanatory factors behind New Zealand's declining abortion rates. A key strength of our study was the inclusion of all data on contraception prescribed nationally, together with annual abortion numbers that are routinely collected at a national level for all elective abortions in New Zealand. This study is also the first to report on national patterns of contraceptive use over time in New Zealand—data have not previously been reported at a national level.
A limitation of our research was the nature of the contraceptive data available for analysis—patient-level data were not available for short-acting methods prescribed, nor for intrauterine methods. Health practitioners often use “Practitioner Supply Orders” to bulk order CuIUD and LNG-IUS, so prescriptions are not linked to recipient's hospital number. It was not therefore possible to investigate the relationship between LARC and age or other important demographic characteristics that may be important when considering abortion rates. Age group data were available for the LNG-implant and LNG-IUS, but due to a lack of comparable data for other methods we could not include age as a factor in our analyses. The use of prescription data has limitations because we do not know what proportion of prescriptions were filled. The typical cost for a 6-month OCP prescription is NZ$5—a cost that is prohibitive for some women.
We examined the potential impact of contraception as a central contributing factor to abortion rates in this analysis, as it is the most easily measured, and arguably the most likely candidate due to increased accessibility of effective LARC methods. While numerous other factors are likely to have contributed to the observed decline (societal, attitudinal, educational, and behavioral), they are far more challenging to assess. Due to a lack of local data on LARC prevalence and removal rates, we estimated prevalence from limited international clinical trial data. Estimates used in this study might therefore differ from actual prevalence for the population studied.
Our study findings align with research conducted elsewhere. For example, a British study investigating the association between LARC and abortion also found significant negative relationships between declining abortion rates and LARC, but only in younger age groups. 16
The Contraceptive CHOICE Project conducted in St. Louis, Missouri provided women with standardized information about and access to LARC methods free of charge in an effort to reduce unintended pregnancy. 15 Seventy-five percent of participants chose a LARC. 15 Twelve-month continuation rates were good among women of all ages (75%), including teenaged participants (81% of 14- to 19-year olds continuing at 1-year follow-up). 27 At 3-year follow-up, 67% of all LARC users but only 31% of non-LARC users were continuing their chosen method (53% and 23% for 14- to 19-year olds), which suggests higher satisfaction with long-acting methods. 28 Abortion rates among participants in the CHOICE study ranged from 4.4 to 7.5 per 1000 (adjusting for age and race) between 2008 and 2010. These rates were significantly lower than the national rate of 19.6 per 1000. 15
Funded LARC options in New Zealand are limited to the CuIUD or the LNG-implant, and the uptake of these methods was found to be closely linked in this study. As use of the LNG-implant increased in 2011, the numbers of women choosing the CuIUD decreased. Similarly, the decrease in the number of LNG-implants prescribed in 2014 corresponded with increased prescription of the CuIUD; therefore, the combination of these two methods was significantly better at predicting change in abortion rates than each method individually.
The abortion rate began to decline in New Zealand in 2008, 2 years before the LNG-implant was subsidized (Figure 2), and in the absence of a significant increase in the use of the CuIUD. It is likely that a shift toward use of these methods by younger women (the group with the most marked decline in abortion rates in New Zealand) partially explains the association between use of these methods and the declining abortion rates. Young women are more likely than older women to experience contraceptive failure when using short-acting contraception. 29 A shift toward the choice of “fit and forget” methods by younger women would conceivably therefore have a greater impact on unintended pregnancy rates for this group.
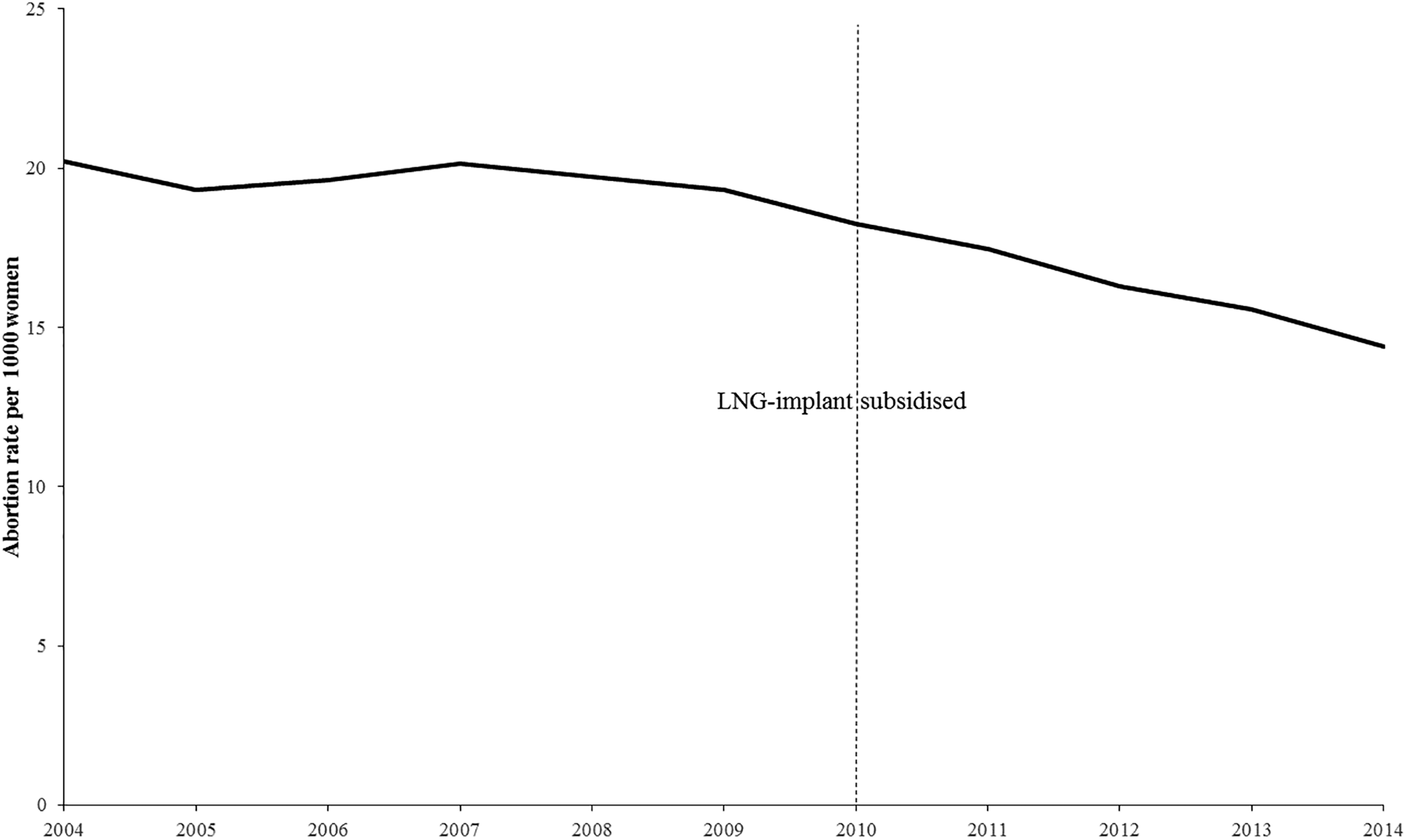
Abortion rates (per 1000 women) in New Zealand from 2004 to 2014.
There has been a growing acceptance of the CuIUD as a safe and effective contraceptive method for young and nulliparous women. 30 This shift in thinking about who can appropriately choose an IUD is well demonstrated in a New Zealand study of postabortion contraceptive uptake. Overall, postabortion LARC uptake increased over the 7-year period studied, but the greatest change was observed for nulliparous adolescents, with LARC use increasing from 5.5% in 2007 to 39.9% in 2013—representing a sevenfold increase by a group not previously considered appropriate candidates for this method. 31
Not only have abortion rates declined in New Zealand, but fertility rates have also declined during the period studied. 32 Declining abortion rates do not therefore simply reflect a shift toward women choosing to continue their pregnancies. Aside from the inclusion of the LNG-implant in the group of contraceptive methods that are government subsidized, and the associated increase in access to this method, there have been no policy changes or national strategies designed to reduce unintended pregnancy in New Zealand. This contrasts with the United Kingdom where government-led strategies have been specifically implemented, and appear to have had a positive impact on teenage pregnancy rates and abortion rates for younger women. 16
The Youth 2000 survey, a large well-being and health survey of New Zealand youth undertaken in 2001, 2007, and 2012, found young people's reports of having sexual intercourse decreased from around one-third in 2001 and 2006 to 24% in 2012. 33 However, changes in survey questions may explain some of this decrease. Delayed first intercourse may account for some of the decline of abortion rates in 15- to 19-year olds. The Youth 2000 survey also suggested declining rates of risk-taking behaviors among youth—for example, in smoking and alcohol use. 33 Reductions in risk-taking behavior may be reflective of overall changes in risky behavioral patterns by youth that could also account in part for observed reductions in the need for abortion. Further research into the impact of behavioral, educational, and attitudinal factors that may be related to unintended pregnancy risk would help further clarify the role of noncontraceptive factors on the declining abortion rate.
Conclusions
Our research highlights the positive impact access to a range of no or low-cost contraceptive methods can have on fertility control. Barrier-free access to all methods of contraception including choice of the most effective long-acting methods should be a sexual reproductive health right afforded to all women, together with access to safe and timely abortion.
Footnotes
Acknowledgments
We thank the New Zealand Ministry of Health and Statistics New Zealand for provision of data pertaining to the prescription of contraceptives and abortion rates. This article reports key results from a thesis undertaken in fulfillment of a Master of Public Health degree undertaken by the lead author (C.E.W.). C.E.W. was awarded a Postgraduate Publishing Bursary from University of Otago, New Zealand. Parts of this work were presented at an oral presentation at the New Zealand Family Planning.
Authors' Contributions
All authors were involved in the conception and design of the study. C.E.W. was responsible for acquisition and analysis of data; drafting and revision of the article. S.B.R. contributed to interpretation of results, drafting and revising the article. D.S. contributed to data analysis and interpretation, and article revision. H.C. assisted with data acquisition, contributed to interpretation of results and article revision. All authors reviewed and approved the final article.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
CEW was awarded a Postgraduate Publishing Bursary from University of Otago, New Zealand
Supplementary Material
Supplementary Data
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.