
Abstract
What is the impact of noncavity-distorting intramural fibroids on live birth rates in in vitro fertilization (IVF) cycles? We searched Embase, MEDLINE, Google Scholar, Cochrane Library, and PUBMED from inception to May 2018. We included studies with women undergoing IVF treatment who had at least one noncavity-distorting intramural fibroid. The studies had to report one or more of the following outcomes: live birth rate as our primary outcome, and implantation rate, clinical pregnancy rate, or miscarriage rate as our secondary outcomes. We excluded studies where women also had submucosal fibroids or had undergone myomectomy. Two authors independently selected studies and extracted data. Methodological quality was assessed using Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines. We included 15 studies with 5029 patients. Patients with noncavity-distorting intramural fibroids had 44% lower odds of live birth (estimated average odds ratio [OR] = 0.56, 95% confidence interval [CI] = 0.46–0.69) and 32% lower odds of clinical pregnancy (estimated average OR = 0.68, 95% CI = 0.56–0.83). Subgroup analysis of women with purely intramural fibroids showed significantly lower odds of live birth rates and clinic pregnancy rates. Analysis of prospective and retrospective studies shows that noncavity-distorting intramural fibroids have a significant adverse effect on live birth rates in women undergoing IVF. Further, well-designed prospective studies are needed to investigate whether removal of these fibroids improves IVF outcomes in this population.
Introduction
Uterine leiomyomas, or fibroids, are the most common benign gynecologic neoplasms among reproductive-age women. 1 Associated symptoms vary greatly depending on the number, size, and location of the pelvic masses, but may include abnormal uterine bleeding, dyspareunia, and noncyclic pelvic pain. 2 Furthermore, the effect of fibroids on infertility has been a topic of ongoing debate. Pritts et al. 3 found that women with submucosal or intramural fibroids experienced significantly lower clinical pregnancy, implantation, ongoing pregnancy, and live birth rates. Conversely, no difference in fertility outcomes was observed among women with subserosal fibroids. This suggests that fibroid location plays a significant role in how fibroids may affect fertility. 3
However, Pritts et al.'s article was marred by several methodological problems with study selection and confounding factors. Thus, its conclusions about the effect of intramural fibroids on fertility outcomes are not necessarily valid. 4
Studies that specifically evaluate the effect of fibroids on in vitro fertilization (IVF) outcomes benefit from exclusion of various confounding factors related to sperm function, anovulation, and tubal function. 5 Donnez and Jadoul 6 found that the presence of fibroids in women undergoing IVF treatment resulted in lower pregnancy rates compared with controls. Interestingly, the meta-analysis also found that uterine cavity distortion by fibroids played a role in the extent to which fibroids decreased fertility. For instance, the pregnancy rates in women with cavity-distorting fibroids, noncavity-distorting fibroids, and no fibroids were 9%, 33.5%, and 40%, respectively. 6
The importance of cavity distortion comes up more frequently in the case of intramural fibroids. Submucosal fibroids distort the uterine cavity, whereas subserosal fibroids do not. On the contrary, intramural fibroids can be either cavity distorting or noncavity distorting. While most agree that intramural fibroids that distort the uterine cavity negatively impact IVF outcomes, the evidence regarding the impact of noncavity-distorting intramural fibroids is controversial. 7 A previous meta-analysis concluded that noncavity-distorting intramural fibroids reduced the live birth rate and clinical pregnancy rate in IVF patients. 7
However, clinical heterogeneity among included studies was a significant limitation. 7 Since then, there have been several studies investigating this issue further. Hence, we conducted an updated systematic review and meta-analysis of current evidence to evaluate the impact of noncavity-distorting intramural fibroids on IVF outcomes.
Materials and Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines 6. 8
Identification of the literature
We performed an exhaustive literature search using MEDLINE (Ovid), Embase (Ovid), Evidence-Based Medicine (EBM) Reviews (OvidB), CINAHL (EBSCO), and the World Health Organization (WHO) Global Health Library from inception to May 2018. We used two subsets of citations. The first included studies of intramural fibroids and used the terms “intramural fibro*,” “intramural leiomyoma*,” or “intramural myoma.*” The second included studies of IVF with the search terms “IVF” or “in vitro fertilization.” The subsets were combined using “AND” to generate relevant citations.
We also searched Biomed Central, ClinicalTrials.gov, WHO International Clinical Trials Registry Platform, and Thomson CenterWatch for unpublished works and ongoing clinical trials. We completed citations chaining using reference lists on all primary studies that remained after our final selection process and on relevant review articles.
Study selection and data extraction
We implemented a two-stage selection process on the works obtained using the above search strategy. First, titles and abstracts were screened using the inclusion/exclusion criteria outlined below. If the abstract was unavailable, the full article was reviewed instead. Second, the full texts of studies that passed the first stage screening were evaluated, and final inclusion or exclusion decisions were made.
Inclusion and exclusion criteria
All studies had to include women in the exposure group undergoing IVF ± intracytoplasmic sperm injection (ICSI) treatment who had at least one or more noncavity-distorting intramural fibroids. We included studies that reported one or more of the following outcomes: live birth rate as our primary outcome, and implantation rate, clinical pregnancy rate, or miscarriage rate as our secondary outcomes. Studies that were written in languages besides English were translated and included if they met the inclusion/exclusion criteria.
We excluded studies where women in the exposure group also had submucosal fibroids in situ and studies where women in the control group had undergone myomectomy for previous fibroids.
Data extraction and quality assessment
Data extraction was performed in a systematic manner, using a preformatted Excel spreadsheet. We collected data on the study objectives, design, population, intervention, control, outcomes, and study quality.
We used the Newcastle–Ottawa Quality Assessment Scale 9 to rate the quality of our evidence. Studies were rated on a scale out of 9 for the following criteria: selection of cohorts and controls, comparability of cohorts on the basis of the design or analysis, and outcomes. Studies that scored ≥7 were regarded as being of good quality.
Statistical analysis
All analyses were carried out in R version 3.4.3 (November 30, 2017) (R Core Team 2017). We used random-effects meta-analysis as implemented in the R package “metafor” to calculate the estimated average odds ratios (ORs). 10 ORs were weighted by the inverse variance, which gives greater weight to larger studies. The I 2 metric was calculated to assess study heterogeneity. We assessed publication bias by visual inspection of funnel plots and using Egger's test. 11 We also conducted subgroup analyses for type of fibroid included (intramural only vs. intramural ± subserosal), type of study performed (retrospective vs. prospective), assisted reproductive technology (ART) method (ICSI only vs. IVF only vs. IVF ± ICSI), and number of IVF cycles (1 vs. >1).
Results
Our search strategy yielded 139 articles (Fig. 1). After removal of duplicate works, we were left with 91 articles. These underwent a title and abstract screening process, after which 59 articles were excluded as they did not fulfill our selection criteria. We conducted a full-text review of the remaining 32 articles and excluded 3 articles as the same data were used in other included studies. 12 –14 This left us with 29 potentially relevant articles.

Preferred Reporting Items for Systematic Reviews and Meta-analysis diagram for study selection. EBM, Evidence-Based Medicine; WHO, World Health Organization.
From there, 14 were excluded from our final selection list for the following reasons: one study did not specify if the fibroids in the exposure group were intramural or subserosal, 15 one study did not have a control group that consisted of women without fibroids undergoing IVF, 16 three studies included women with all fibroids types, including submucous fibroids, in their exposure group 17 –19 and finally, nine studies were excluded because women in the exposure group did not all have at least one intramural fibroid. 20 –28 This left us with 15 studies, with a total of 5029 patients, included in the review. All the studies were full articles, and they were all in English.
All 15 studies were observational studies, in which the exposure group (women with ∼1 noncavity-distorting intramural fibroid undergoing IVF) and the control group (women without fibroids undergoing IVF) were followed up to the outcomes. Ten studies were retrospective in nature, 29 –38 whereas five studies were prospective in nature. 39 –43 Supplementary Table S1 reflects the main characteristics of each study, and Table 1 reflects the Newcastle–Ottawa Quality Assessment. Two studies scored 7, nine studies scored 8, and three studies scored the maximum of 9.
Quality Assessment Using Newcastle–Ottawa Scale
indicates 1 point.
X indicates 0 points.
Live birth rate
Eight of 15 studies reported the live birth rate. 29,32,33,35,37,40,41,43 The random-effects model showed that women with noncavity-distorting intramural fibroids had significantly lower odds of live birth than women without fibroids (estimated average OR = 0.56, 95% CI = 0.46–0.69) (Fig. 2). There was no significant heterogeneity among studies (I 2 = 0%, Q test p = 0.32). There was no obvious evidence of systematic bias in the funnel plot, and Egger's test was not significant (p = 0.88). Given the small sample size, these results should be treated with caution, but it does not appear that a strong publication bias was present.
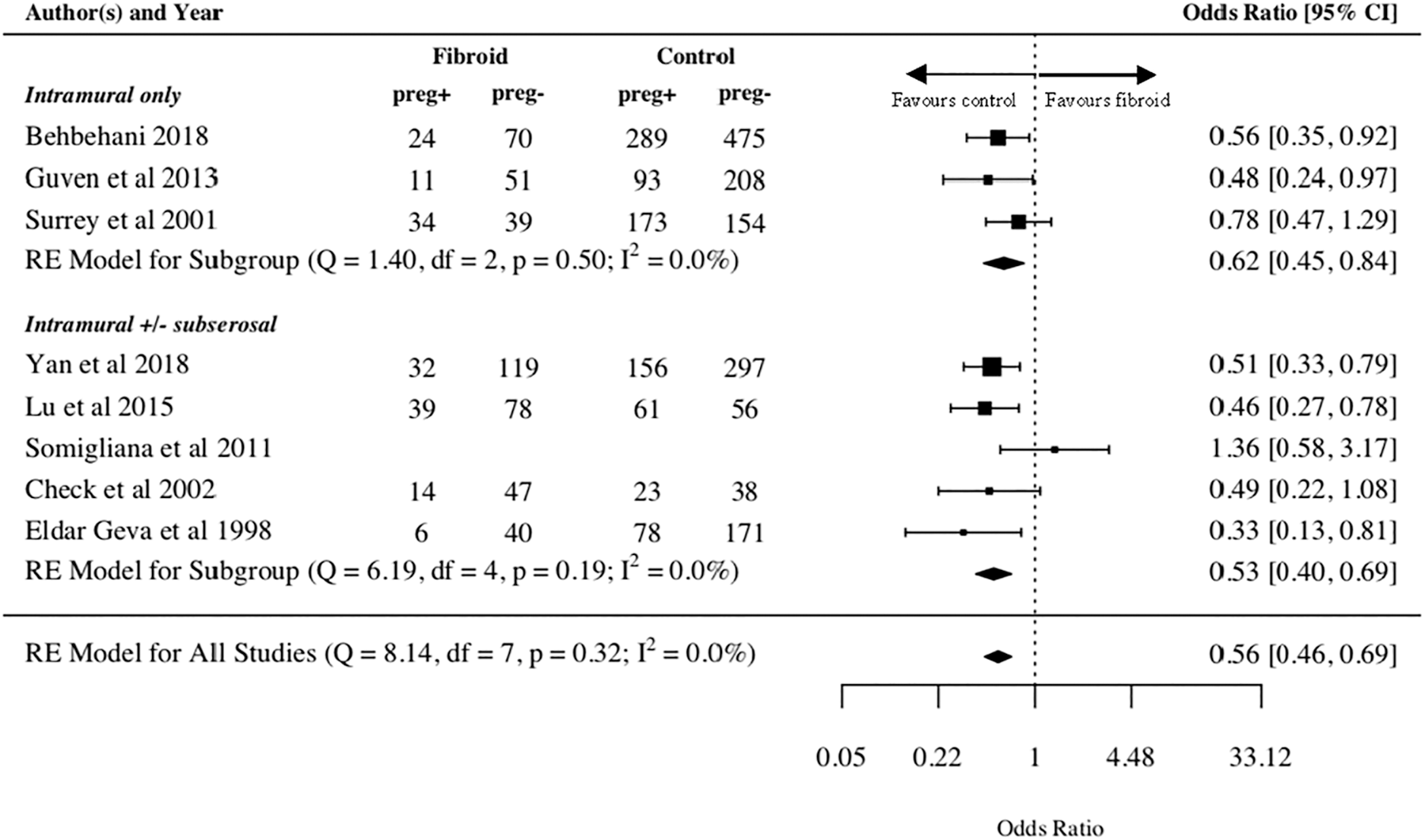
Live birth rate by fibroid type. CI, confidence interval; RE, Random Effects.
On subgroup analysis of studies that included intramural fibroids only, women with these fibroids had significantly lower odds of live birth (estimated average OR = 0.62, 95% CI = 0.45–0.84) (Fig. 2). This was similar for studies that included women with intramural ± subserosal fibroids (estimated average OR = 0.53, 95% CI = 0.40–0.69) (Fig. 2). Women with fibroids had significantly lower odds of live birth on subgroup analysis of retrospective studies and prospective studies (estimated average OR = 0.62, 95% CI = 0.45–0.84 and estimated average OR = 0.56, 95% CI = 0.46–0.69, respectively) (Supplementary Figure S1). For studies that included patients who underwent either IVF ± ICSI or only ICSI, the live birth rate was significantly lower for women with fibroids (estimated average OR = 0.64, 95% CI = 0.46–0.90 and estimated average OR = 0.50, 95% CI = 0.35–0.73, respectively) (Supplementary Figure S1). For studies that included patients who underwent only 1 IVF cycle, the live birth rate was significantly lower for women with fibroids (estimated average OR = 0.52, 95% CI = 0.40–0.69), but this was not the case for patients who underwent >1 IVF cycle (estimated average OR = 0.63, 95% CI = 0.37–1.07) (Supplementary Figure S1).
Clinical pregnancy rate
All 15 studies reported clinical pregnancy rate. The random-effects model showed significantly lower odds of clinical pregnancy in the fibroid group (estimated average OR = 0.68, 95% CI = 0.56–0.83) (Fig. 3). There was no significant heterogeneity among studies (I 2 = 35.6%, Q test p = 0.08). There was no obvious evidence of systematic bias in the funnel plot, and Egger's test was not significant (p = 0.52), suggesting no strong publication bias.
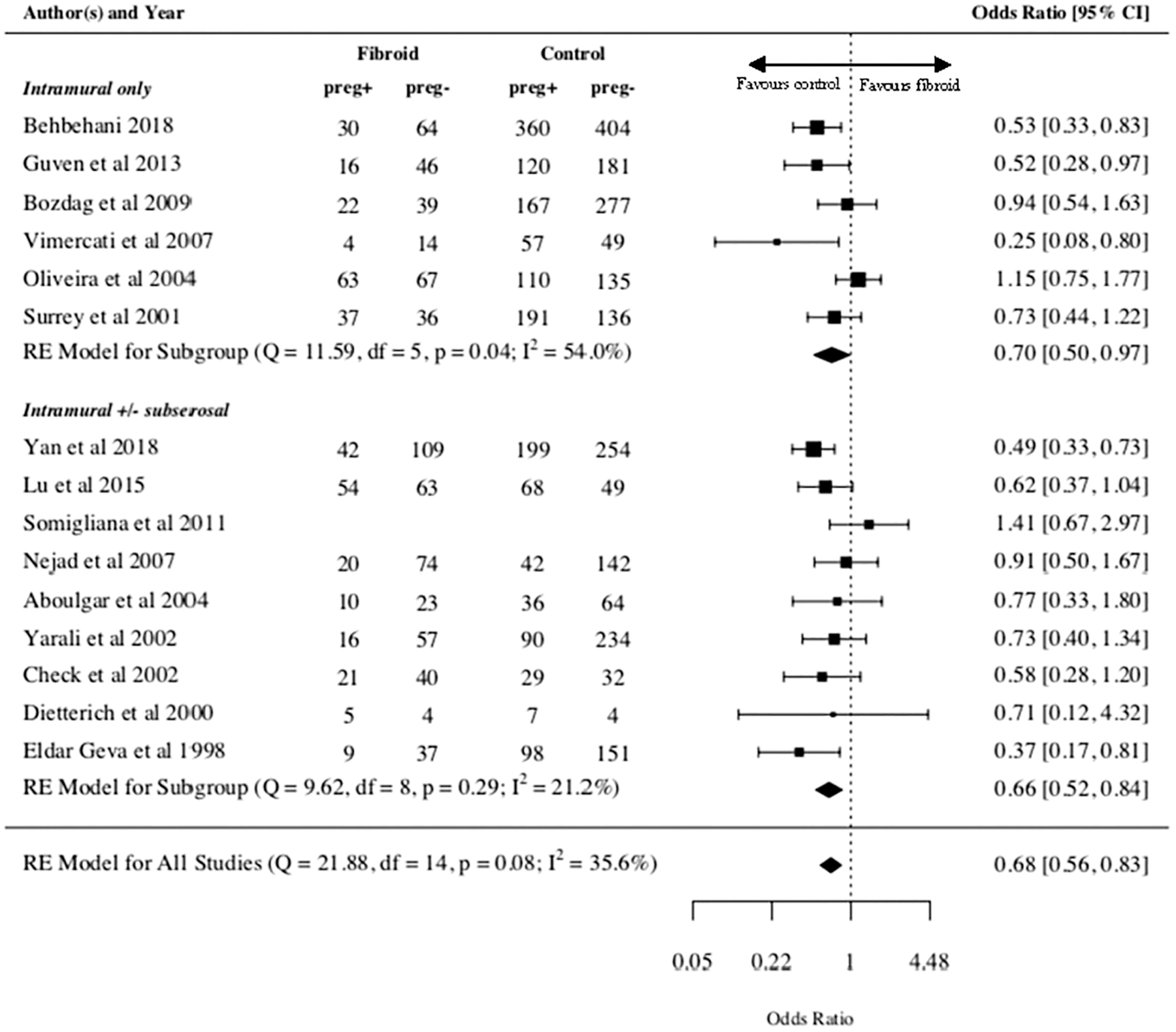
Clinical pregnancy rate by fibroid type.
On subgroup analysis of studies that included intramural fibroids only, women with these fibroids had significantly lower odds of clinical pregnancy (estimated average OR = 0.70, 95% CI = 0.50–0.97) (Fig. 3). This was similar for studies that included women with intramural ± subserosal fibroids (estimated average OR = 0.66, 95% CI = 0.52–0.84) (Fig. 3). On analysis of retrospective studies, women with fibroids had significantly lower odds of clinical pregnancy (estimated average OR = 0.64, 95% CI = 0.49–0.82), but this difference was not significant when analyzing prospective studies only (estimated average OR = 0.78, 95% CI = 0.58–1.06) (Supplementary Figure S2).
Women with fibroids who underwent IVF ± ISCI had significantly lower odds of clinical pregnancy than women without fibroids (estimated average OR = 0.64, 95% CI = 0.46–0.89). However, there was no significant difference in the clinical pregnancy rates between the two groups for patients who underwent IVF only (estimated average OR = 0.66, 95% CI = 0.43–1.01) and ICSI only (estimated average OR = 0.73, 95% CI = 0.51–1.04) (Supplementary Figure S2). For studies that included patients who underwent only 1 IVF cycle, the clinical pregnancy rate was significantly lower for women with fibroids (estimated average OR = 0.70, 95% CI = 0.53–0.92), and this was similar for patients who underwent >1 IVF cycle (estimated average OR = 0.67, 95% CI = 0.51–0.88) (Supplementary Figure S2).
Implantation rate
Eight of 15 studies reported implantation rates. 30,31,35 –38,41,43 In the random-effects model, the association between implantation rate and presence of noncavity-distorting intramural fibroids did not reach statistical significance (estimated average OR = 0.76, 95% CI = 0.58–1.01) (Fig. 4). There was some heterogeneity among studies (I 2 = 61.2, Q test p = 0.02), but no significant evidence of systematic bias was appreciated by the funnel plot, nor evidence of significant publication bias as demonstrated by Egger's test (p = 0.47).
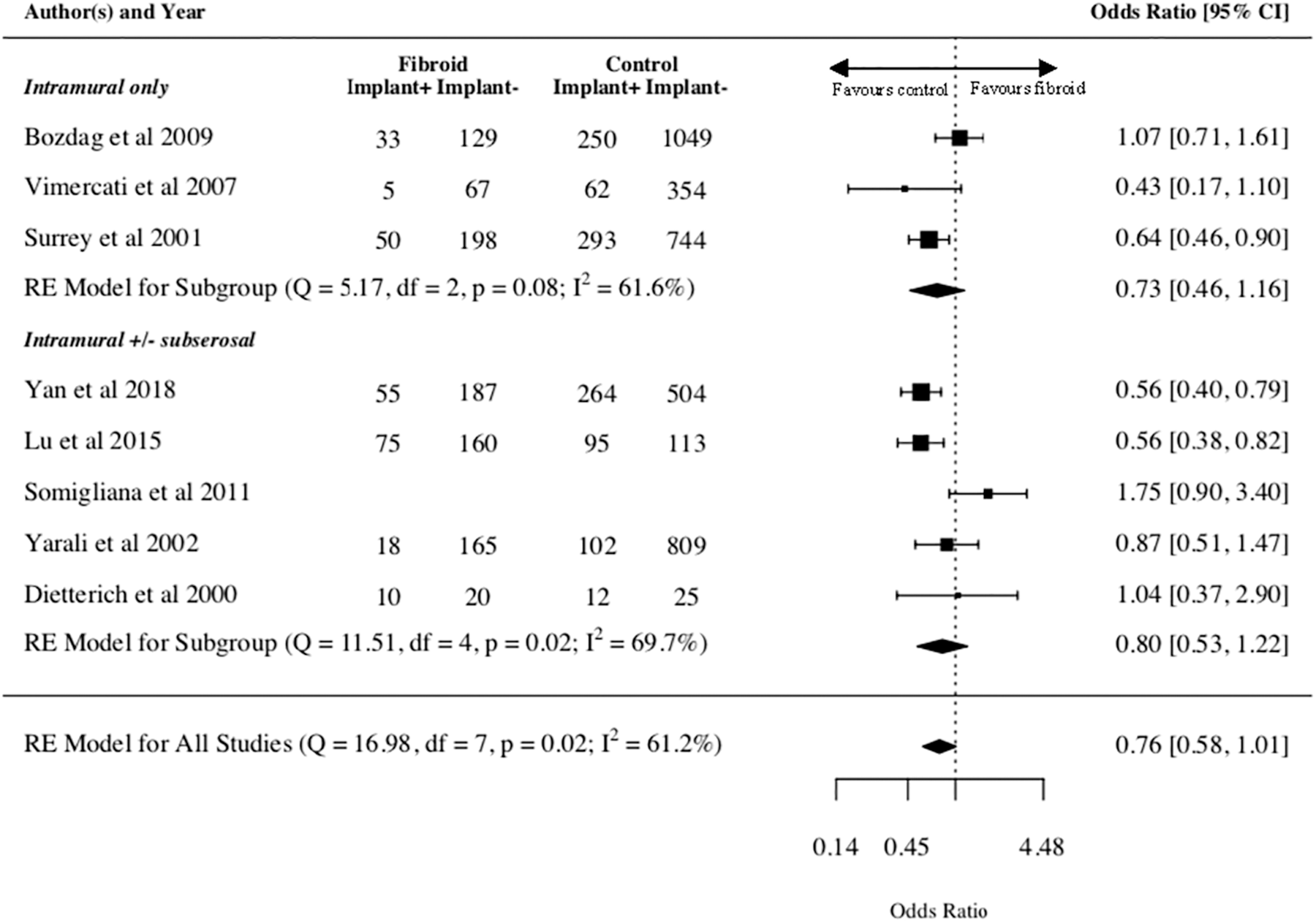
Implantation rate by fibroid type.
On subgroup analysis of studies that included intramural fibroids only, women with these fibroids tended to have lower odds of implantation but this did not reach clinical significance (estimated average OR = 0.73, 95% CI = 0.46–1.16) (Fig. 4). This was similar for studies that included women with intramural ± subserosal fibroids (estimated average OR = 0.80, 95% CI = 0.53–1.22) (Fig. 4). On analysis of retrospective studies, women with fibroids had significantly lower odds of implantation (estimated average OR = 0.73, 95% CI = 0.56–0.95), but this difference was not significant when analyzing prospective studies only (estimated average OR = 0.96, 95% CI = 0.31–2.93) (Supplementary Figure S3). Subgroup analysis was also performed for ART method (IVF ± ICSI vs. IVF only vs. ICSI only) and number of IVF cycles (1 IVF cycle vs. >1 IVF cycle). All subgroups showed lower implantation rates in the exposure group, but none reached significance (Supplementary Figure S3).
Miscarriage rate
Ten of 15 studies reported the miscarriage rate. 29,30,32,33,34,36 –38,40,41 In the random-effects model, the association between miscarriage rate and presence of noncavity-distorting intramural fibroids did not reach statistical significance (estimated average OR = 1.38, 95% CI = 0.98–1.95) (Fig. 5). There was no significant heterogeneity among studies (I 2 = 0%, Q test p = 0.881). There was no obvious evidence of systematic bias in the funnel plot, and Egger's test was not significant (p = 0.26). Although the small sample size suggests that these results should be treated with caution, it does not appear that there was very strong publication bias.
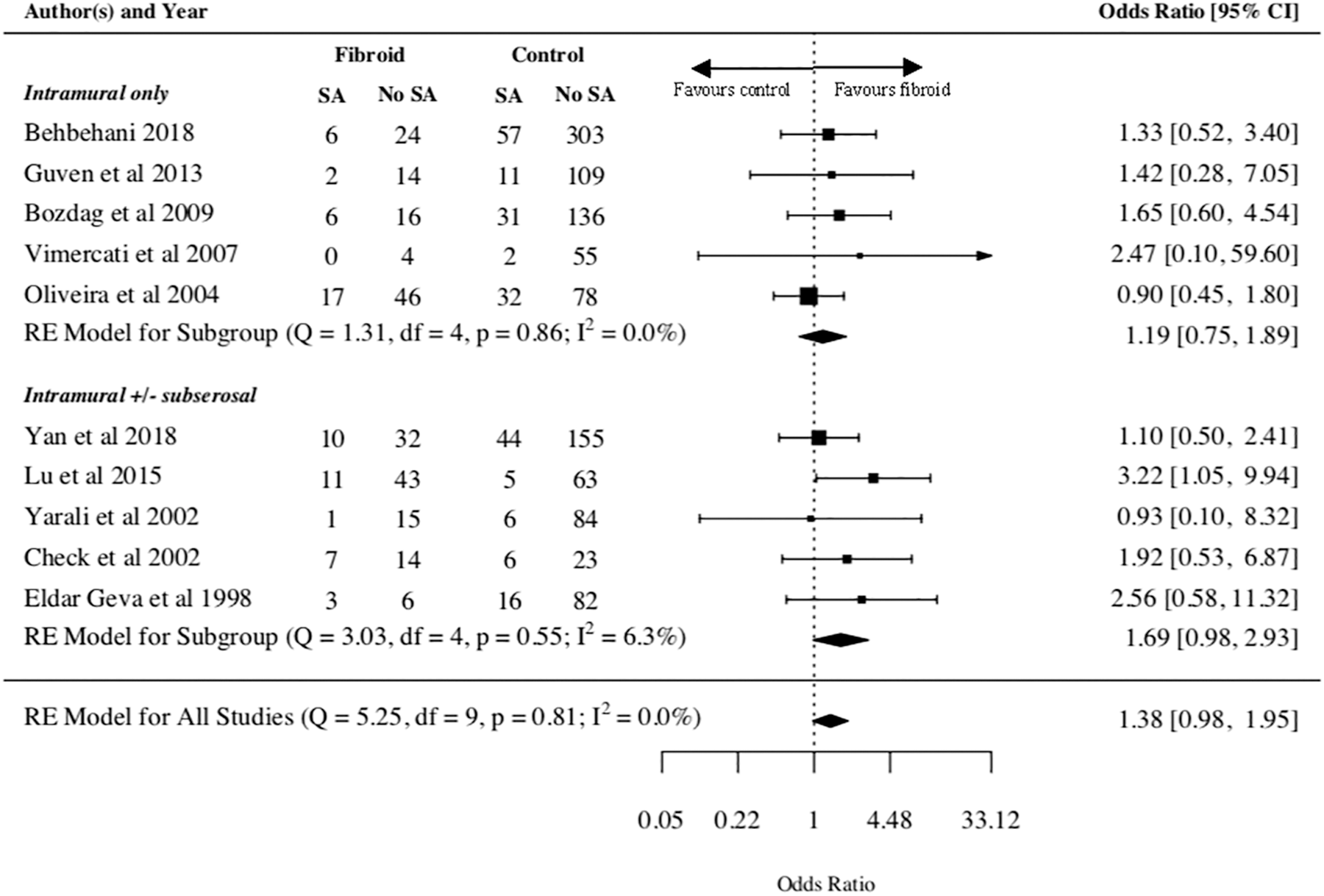
Miscarriage rate by fibroid type.
On subgroup analysis of studies that included intramural fibroids only, women with these fibroids tended to have higher odds of miscarriage but this did not reach clinical significance (estimated average OR = 1.19, 95% CI = 0.75–1.89) (Fig. 5). This was similar for studies that included women with intramural ± subserosal fibroids (estimated average OR = 1.69, 95% CI = 0.98–2.93) (Fig. 5). On analysis of retrospective studies, women with fibroids had higher odds of miscarriage but this did not reach significance (estimated average OR = 1.22, 95% CI = 0.83–1.78) (Supplementary Figure S4). For prospective studies, the miscarriage rate was significantly higher for women with fibroids (estimated average OR = 2.57, 95% CI = 1.10–5.97) (Supplementary Figure S4).
Subgroup analysis was also performed for ART method (IVF ± ICSI vs. ICSI only) and while both subgroups showed a tendency toward higher miscarriage rate in the exposure group, neither reached significance (Supplementary Figure S4). On analysis of studies in which women underwent 1 IVF cycle, women with fibroids had higher odds of miscarriage, but this did not reach significance (estimated average OR = 1.21, 95% CI = 0.82–1.77) (Supplementary Figure S4). For women who underwent >1 IVF cycle, the miscarriage rate was significantly higher for women with fibroids (estimated average OR = 2.51, 95% CI = 1.12–5.60) (Supplementary Figure S4).
Discussion
Main findings
Our systematic review found that patients with noncavity-distorting intramural fibroids undergoing IVF had 44% lower odds of live birth and 32% lower odds of clinical pregnancy than patients without fibroids. There was also a trend toward lower implantation rates and higher miscarriage rates in patients with these fibroids, although these did not reach statistical significance. Since live birth rate is the gold standard by which we measure IVF success, our analysis indicates that noncavity-distorting intramural fibroids may have an adverse impact on IVF success.
Among studies that included patients with only intramural fibroids, there were significantly lower odds of live birth and clinical pregnancy in the exposure group when compared with the control group. This is relevant because it removes the potentially confounding effect of subserosal fibroids, and it allows us to look at the effect of intramural fibroids in isolation.
Furthermore, subgroup analysis of prospective studies showed that the odds of live birth were significantly reduced in women with these fibroids. These studies help us make more robust conclusions on the topic without the inherent selection bias present in retrospective studies.
Interpretation
Several authors have attempted to identify the mechanisms by which noncavity-distorting intramural fibroids may affect IVF outcomes. One prevalent theory is that these fibroids alter uterine peristalsis during the implantation stage. A 2010 study used MRI technology to detect uterine peristalsis in 51 women with noncavity-distorting intramural fibroids. The authors discovered that intramural fibroids led to abnormal uterine peristalsis, which resulted in decreased implantation and pregnancy rate. 44 Although this study was carried out on a non-IVF population, it can still give us some insight as to the mechanism by which fibroids affect fertility.
Another leading hypothesis is that intramural fibroids increase blood flow to the endometrium. Kamel et al. 45 used 3D power Doppler ultrasound to assess the endometrial vascularity in patients with noncavity-distorting intramural fibroids before IVF initiation. They demonstrated that intramural fibroids >4 cm significantly increased endometrial vascularity, which led to dysregulation of endometrial function. 45 There is currently no consensus on the topic, and further research is required to discover the mechanisms by which noncavity-distorting intramural fibroids affect IVF outcomes.
Alternatively, it is possible that fibroid-associated confounding variables may be partially responsible for the observed relationship between noncavity-distorting intramural fibroids and IVF outcomes. For example, although most studies matched or controlled for age (Supplementary Table S1), they generally did not match for other potential confounders associated with fibroids such as body mass index or ethnicity.
Strengths and limitations
Sunkara et al. 7 carried out the only systematic review thus far to investigate the effects of noncavity-distorting intramural fibroids on IVF outcomes and demonstrated results consistent with those of this meta-analysis. Their systematic review found a 21% reduction in live birth rate and 15% reduction in clinical pregnancy rate in women with noncavity-distorting intramural fibroids. The authors hypothesized that these fibroids had an adverse effect on the course of the pregnancy, thus leading to a relatively low chance of achieving a live birth compared with a clinical pregnancy. 8
Although we had similar results to the meta-analysis by Sunkara et al., 7 our review had some notable differences in its methodology. For instance, we were much more specific about the types of fibroids we wanted women in our study groups to have. We only selected studies where all the women in the exposure group had at least one noncavity-distorting intramural fibroid, whether they had additional subserosal fibroids or not. However, Sunkara et al. 7 included studies where only a majority, but not all, women in the exposure group had one noncavity-distorting intramural fibroid. By inference, there were women in these exposure groups who had only noncavity-distorting subserosal fibroids in situ. Since our goal was to specifically investigate the effect of intramural fibroids, we can better extrapolate our results to women in this population.
Sunkara et al. 7 noted that the main weakness in their review was the clinical heterogeneity among the included studies. To address this issue, the authors performed analyses on the following subgroups: women with mean age <37 years old, women having their first IVF treatment cycle, and prospective studies. Results were similar in all subgroups; noncavity-distorting intramural fibroids had a negative impact on IVF outcomes. 8 Our review included even more subgroup analyses to better address clinical heterogeneity. We included the following subgroups: intramural fibroids only versus intramural fibroids ± subserosal fibroids, retrospective studies versus prospective studies, IVF ± ICSI versus IVF only versus ICSI only, and 1 IVF cycle versus >1 IVF cycle.
Perhaps the most important difference between our review and Sunkara et al.'s 7 is our subgroup analysis of studies with women who had purely intramural fibroids and no other fibroids, including subserosal, in situ. We identified six studies that fit this criterion: Behbehani et al., 29 Bozdag et al., 30 Oliveira et al., 34 Guven et al., 33 Surrey et al., 35 and Vimercati et al. 36 By doing so, we were able to very precisely answer our research question by eliminating the potential confounding effect of subserosal fibroids. We have thus shown that noncavity-distorting intramural fibroids negatively impact IVF outcomes independently of the presence of other fibroids, and our results further our understanding of the sequelae of such fibroids.
Furthermore, our meta-analysis is novel in its subgroup analysis of prospective studies only. This analysis showed significantly lower odds of live birth and significantly higher odds of miscarriage in women with noncavity-distorting intramural fibroids. Conversely, while prospective studies showed a trend toward lower odds of clinical pregnancy and implantation in the exposure group, these results did not reach statistical significance. However, given that live birth was our primary outcome and the gold standard by which IVF success is measured, the analysis of prospective studies supports our overall conclusion.
Similar to Sunkara et al., 7 the heterogeneity between the studies we included was the primary limitation of this review. Studies differed in their matching criteria between the study group and control group, the ART method used (IVF vs. IVF ± ICSI vs. ICSI only), the number of IVF cycles performed, the number of embryos transferred, and the types of fibroids investigated (intramural fibroids only vs. intramural fibroids ± subserosal fibroids). To address this heterogeneity, we performed multiple subgroup analyses—all of which consistently demonstrated the negative impact of noncavity-distorting intramural fibroids on IVF outcomes.
Moreover, studies used different tools to distinguish whether fibroids were subserosal, intramural, or submucosal. Six studies used transvaginal ultrasound and hysteroscopy, 29,30,33,35 –37 one study used transvaginal ultrasound and sonohysterogram, 39 while one study used transvaginal ultrasound and either hysterosalpingography and/or hysteroscopy. 38 Three studies used transvaginal ultrasound and hysterosalpingogram. 34,40,43 Four studies used only transvaginal ultrasound. 31,32,41,42 Each modality has a certain error rate associated with it and thus, it is difficult to determine if the fibroids in the included studies were at the location they were said to be.
Another notable limitation was that we were unable to assess the size and location of the fibroids within the uterus (anterior/posterior/fundal) due to inconsistent reporting in the included studies. For instance, Bozdag et al. 30 reported the mean size of all intramural fibroids, while Behbehani et al. 29 only reported the mean size of the largest intramural myoma in women with multiple fibroids. Furthermore, while Dietterich et al. 31 reported the number of fibroids that were anterior, posterior, and fundal in nature, Aboulghar et al. 39 did not make note of these characteristics in their study. These important characteristics likely impact IVF outcomes, but we were unable to determine their significance.
Finally, most of the studies included (10 of 15) were retrospective in nature. Thus, there is a higher chance of inherent selection bias in these works. There are currently no randomized controlled trials (RCTs) on this topic. Further RCTs and prospective studies are needed to better delineate the relationship between intramural fibroids and IVF outcomes.
Conclusions
This meta-analysis demonstrates that women with noncavity-distorting intramural fibroids had significantly lower odds of live birth when undergoing IVF. Our work is the most extensive review to date and can help clinicians performing IVF treatment better understand the role intramural fibroids play in their patients' outcomes. However, due to clinical heterogeneity between the included studies, further RCTs and prospective studies that standardize their patient selection criteria and IVF methods are needed to better address this question. Furthermore, although an association between the presence of noncavity-distorting intramural fibroids and impaired IVF outcomes was observed, the benefit of surgically removing these fibroids cannot be inferred. Hence, additional well-designed RCTs are needed to demonstrate whether there is a benefit in removing noncavity-distorting intramural fibroids in the IVF population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.