
Abstract
Background:
Recommendations for using menopausal hormone therapy (MHT) and bisphosphonates for postmenopausal osteoporosis management have changed over time. After the release of the Women's Health Initiative (WHI) trial results in 2002, new evidence on risks and benefits of MHT became available, and newer guidelines generally specify that MHT should not be prescribed for prevention of chronic disease, including osteoporosis. This raises the question of whether bisphosphonate prescribing changed over time to compensate for the decrease in MHT use.
Materials and Methods:
We examined trends in dispensed prescriptions in Australia (national) and Canada (province of Manitoba) in relation to prescribing recommendations. Administrative data were used to describe dispensing patterns and changes for persons of all ages from 1996 to 2008, and for women aged 50 to ≥80 years from 2003 to 2008 in Australia and 1996 to 2008 in Canada.
Results:
In both geographic settings, MHT dispensing increased 1996–2001, peaked in 2001, and declined substantially thereafter (67% reduction in MHT prescriptions for Australia; 64% reduction for Manitoba, Canada to 2008). From 2003 to 2008, the number of MHT prescriptions declined among all age groups in both settings, with the highest declines among women in their 50s. Concurrently, bisphosphonate dispensing increased until 2005 (2001–2005: 260% increase in the number of prescriptions in Australia; 125% increase in Manitoba) and stabilized thereafter, in both settings. Annual bisphosphonate dispensing rates increased 4.1–10.9% for women in their 70s and 80s in Australia and Manitoba during the period studied.
Conclusions:
Based on dispensed prescriptions data, more recent guidelines for MHT and bisphosphonates use for postmenopausal osteoporosis, which were updated during the study period (and are still consistent with the current guidelines), appear to have been broadly adhered to in both settings.
Introduction
Osteoporosis is an important public health issue for aging populations, with the burden of disease likely to increase substantially over the coming decades. Australia and Canada are two developed countries with aging populations, where one in every five people are over the age of 60 years. 1 As more information on the risks and benefits of menopausal hormone therapy (MHT) and bisphosphonates for the management of postmenopausal osteoporosis has become available, regulatory guidance (i.e., from national regulatory agencies) regarding their use has changed by becoming more specific in that, for example, MHT is generally recommended for management of menopausal symptoms and not for prevention of chronic disease. 2 In the past, both preparations were used, in certain geographic settings, for the prevention of osteoporosis. Since the release of first results from the Women's Health Initiative (WHI) trials in 20023 and subsequent high-quality evidence, 4,5 individualized treatment with the lowest therapeutic dose of MHT and periodic re-evaluation, of use is recommended. MHT is now recommended primarily for the relief of menopausal symptoms, rather than for the prevention of chronic disease. 6,7 Following the WHI trial results, MHT prescribing has fallen substantially in many European countries, 8 –11 in Australia 12,13 and Canada. 14 Based on age-specific prescribing data, this fall appears to have occurred predominantly in younger postmenopausal women for whom MHT was previously frequently prescribed. 8,15,16
Concurrently, a substantial increase in the use of bisphosphonates in peri/postmenopausal women has been reported in Europe 11,17–18 and the United States. 19,20 Despite initial suggestions that this increase might in part reflect the replacement of MHT by bisphosphonates prescribed for osteoporosis prevention in younger postmenopausal women, 19 the increase appears to have occurred predominantly in women ≥65 years old. 11,18 Such a change is consistent with the increased availability of weekly or monthly oral bisphosphonate regimes around the same period and the emergence of less frequent (e.g., annual) intravenous delivery options. 21 Increased use among women aged ≥65 years is also consistent with population aging, since the incidence of osteoporotic fractures (e.g., hip and vertebrae) increases steeply with age. 22 As more evidence on the risks of bisphosphonate use became available, 23 prescribing has become more targeted toward prevention of fractures in osteoporotic women, rather than on osteoporosis prevention per se. 24
Bisphosphonates are among the most widely used medications for the prevention and treatment of osteoporosis 25 and before 2002, MHT formulations were commonly used for the relief of menopausal symptoms. 26,27 There is evidence to suggest a decrease in population-level incidence of breast cancer in several countries after the decrease in MHT use after 2002. 8,12,14 In parallel, bisphosphonate use is thought to have contributed to declining rates in hip fracture incidence in several countries. 28 –31 The use of MHT and bisphosphonates has also been characterized by a rapidly and substantively changing clinical and policy environment, in line with major shifts in the availability of evidence on their risks and benefits. Australia and Canada share similarities in health systems, and have quality records of dispensed MHT and bisphosphonates collected by routine administrative databases. They are thus suitable geographic settings for investigating the impact of changes in government reimbursement for certain MHT preparations and the consequent impact on the quality use of medicines and, ultimately, health outcomes.
The aim of this study was to assess whether postmenopausal women's patterns of use of MHT and bisphosphonates in Australia and Manitoba (Canada) changed over the study period; more specifically, (1) to quantify changes in dispensing of MHT and bisphosphonates, especially after 2002, in two settings for which direct comparative data for trends in their use have not previously been reported; (2) to assess whether these changes were of similar magnitude and occurred over a similar period; and (3) to confirm that the decreases in MHT use occurred predominantly in younger (<70 years) women and increases in bisphosphonate use occurred in older (≥70 years) postmenopausal women.
Materials and Methods
Data sources
For Australia and Manitoba, data on dispensed prescriptions at point of sale were used. For both settings, the total number of prescriptions dispensed annually were used to describe long-term trends; an annual prescribing period was chosen to minimize short-term rate fluctuations. For Australia (all states and territories), we used data from the Pharmaceutical Benefits Scheme and Repatriation Pharmaceutical Benefits Scheme databases (collectively referred to as the “PBS database”). The PBS database is a national database that records reimbursement claims for all physician-prescribed dispensed prescriptions subsidized under the PBS for Australian residents. Medicines in Australia are partially subsidized and therefore reimbursed, only if they are above a threshold price (the “co-payment threshold”). For the study period, the PBS database captured reimbursement claims, and therefore dispensed prescriptions across the whole population for bisphosphonates, as bisphosphonates were priced above the threshold. Almost all MHT preparations were priced below the copayment threshold. The PBS database only captured complete dispensing of MHT prescriptions for a subgroup eligible for concessions (e.g., due to disability or for old age pensioners) as well as for patients captured under a special safety net scheme designed to limit an individual's total expenditure on medicines. Our analysis of dispensed MHT prescriptions was restricted to this group, here collectively referred to as “concession card holders.” The issue of the generalizability of the prescribing data from this subgroup of women is addressed in Supplementary Data.
Although overall prescription numbers were available for persons of all ages for the period 1996–2008, age- and sex-specific data were recorded in the PBS database only from mid-2002. Therefore, age- and sex-specific analyses were limited to 2003 onward.
Analyses were confined to the period until 2008 because, in 2009, some highly prescribed MHT preparations were removed from the PBS (including Premarin™, Premia Continuous™, Kliovance™, Kliogest™, and Trisequens™), which meant that concession card holders would no longer receive reimbursement when purchasing these preparations. Also, findings from surveys and ecological studies suggest that the prevalence of MHT use in the population has been more stable since 2008. 32 –35 The introduction of newer generation antiosteoporotic medications (AOMs) other than bisphosphonates, such as teriparatide (Forteo™) and denosumab (Prolia™), into the PBS scheme means that from 2009 onward bisphosphonate dispensing alone does not represent all the pharmacological interventions used for osteoporosis management in Australia. Additional details on the recording of MHT dispensations in the PBS database and validation analysis to assess the representativeness of concessional dispensing are reported as Supplementary Data.
For Manitoba, data on drug utilization are available through the Drug Program Information Network (DPIN), which is linked to all pharmacies and captures dispensed prescriptions at point of sale. This database is maintained by Manitoba's Ministry of Health. We first conducted validation analyses of data from Manitoba 36 against Canadian data, and found that it broadly reflects dispensing in Canada, nationally (Supplementary Fig. S1 in Supplementary Data S1). Utilization trends in Manitoba were compared with Canadian national trends studied in prior analyses, 14,37 and relative changes in utilization from the Manitoban provincial data and Canadian national data were found to closely correspond. 38
Lists of candidate regulatory-approved and reimbursed medications were obtained from the PBS for Australia and the Canadian Drug Products Database (DPD). The lists were reviewed and classified in consultation with the study team members (K.C. for Australia and E.V.K., W.D.L. for Manitoba). For this analysis, MHT was defined as any oral or transdermal estrogen-only and combined estrogen–progestagen preparation indicated for the alleviation of menopausal symptoms. For Australia, only the preparations that were subsidized by the PBS at any point in time during the study period were included, and this list was confirmed by comparison with a list used in a previous analysis by some of the study team members. 12 Tibolone was not subsidized in either setting and therefore was not included.
Bisphosphonates were defined as preparations of alendronate, risedronate, etidronate, and zoledronic acid for both countries. Other AOMs constituted a low proportion of overall dispensing and were examined separately. This group included raloxifene, strontium ranelate, calcitonin and parathyroid hormone analogues. A list of MHT and bisphosphonates included in the current analysis is provided (Supplementary Data S2).
Dispensing patterns 1996–2008
Time trends in dispensing of MHT, bisphosphonates and AOMs for all persons were examined for Australia and Manitoba for 1996–2008. In addition, we also calculated and compared the percentage changes in the number of dispensed MHT and bisphosphonate prescriptions, for persons of all ages over three time periods: (1) 1997–2001 (before WHI trial results); (2) 2001–2005 (before WHI trial results and then after the impact of the findings on MHT prescribing generally stabilised; also, bisphosphonate weekly preparations were released late 2001) and (3) 2005–2008 (after changes in prescribing guidelines for MHT in Australia and bisphosphonates in Manitoba, due to changes in its formulation).
Age-specific dispensing trends and relative changes in MHT and bisphosphonate use, 2003–2008 (Australia) and 1998–2008 (Manitoba)
The age-specific analysis focused on women ≥50 years, from both Australia and Manitoba. The cutoff age of 50 years was based on the average age at menopause from a pooled analysis of worldwide data being 49.3 years. 39 We compared patterns of use based on the total number of dispensed prescriptions, and the percentage change in the number of dispensed prescriptions by 10-year age groups in women aged ≥50 years over the time periods 1998–2003 (Manitoba) and 2003–2008 (Manitoba and Australia).
Annual percentage change in bisphosphonate dispensing rates 2003–2008
The annual rate of bisphosphonate prescriptions dispensed per 1,000 women in each age group by calendar year, for both countries, was modeled using generalized linear models assuming a Poisson distribution and log-link function, taking into account the differences in population structure over time. The dependent variable in each model was the number of prescriptions dispensed for each combination of categories of the independent variables and with the corresponding mid-year populations included as an offset. Independent variables were age (50–59, 60–69, 70–79, and ≥80 years) and calendar year (2003–2008), both treated as continuous variables with linear and quadratic terms. Terms for the interaction between age and calendar year were included in the models. To account for possible overdispersion, Poisson's standard errors were inflated by a scale parameter equal to the Pearson chi-squared statistic divided by the residual degrees of freedom. 40 Both linear and quadratic models were tested, with the quadratic model giving a better fit. The rate ratio indicating per year increase in dispensing per 1,000 women was averaged over a 5-year period (2003–2008) for the quadratic model where the trend is nonlinear in the log scale. Data were analyzed with STATA version 11.
Ethics approvals
Approval for access to Canadian data and for the analysis was obtained from the data custodians, Manitoba Health, and the Research Ethics Board at the University of Manitoba. Approval for access to Australian data was obtained from Medicare Australia external research evaluation committee, and ethics approval for the data analysis was obtained from the Sydney University Human Research Ethics Committee.
Results
Dispensing patterns 1996–2008 for MHT and bisphosphonates
Overall dispensing patterns of MHT, bisphosphonates, and AOMs over time were similar for Australia and Manitoba (Fig. 1). Australian concession card holders received a higher absolute number of dispensed MHT and bisphosphonate prescriptions compared with the Manitoba population, due to the former being a larger population (Australia had a total population of 20 million in 2002 [the midpoint of the study period], compared with a population of 1.2 million in Manitoba). In Australia, bisphosphonate dispensing for men was 13%–19% of total bisphosphonate prescriptions dispensed each year, over 2003–2008. In Manitoba, it was 7.4%–8.9% of the total annual bisphosphonate prescriptions dispensed 1996–2008. Sex-specific dispensing data were not available for Australia for earlier years. Therefore, in both settings, the majority of prescriptions over the study period were for women. AOMs constituted a low proportion (5.4% in Australia; 3.8% in Manitoba) of total antiosteoporotic dispensing and were therefore not considered for further analysis.

Number of dispensed prescriptions for MHT, bisphosphonates, and other AOMs in Australia (top panel) and Manitoba (bottom panel) from 1996 to 2008. ○ MHT prescriptions; ▪ bisphosphonate prescriptions; Δ other AOM prescriptions (Calcitonin, Raloxifene, Parathyroid hormone); _ _ _ the point in time when the WHI trial findings became publicly available. Top panel: prescription numbers for MHT, bisphosphonates, and other AOMs in Australia concessional card holders only. Data source: The PBS database and includes preparations as listed in Supplementary Data S2. Bottom panel: Prescription numbers for MHT, bisphosphonates, and other AOMs in Manitoba, Canada-all persons all ages. Data source: The DPIN database and includes preparations as listed in Supplementary Data S2. AOM, antiosteoporotic medications; DPIN, Drug Program Information Network; MHT, menopausal hormone therapy; WHI, Women's Health Initiative.
In both settings, MHT was more frequently dispensed compared with bisphosphonates in 1996 and, in both settings MHT use continued to increase, reaching a maximum in 2001, before the WHI findings were released in 2002. The number of MHT prescriptions dispensed each year declined substantially thereafter in both settings, as previously reported. 13,14 The relative increase in dispensed MHT prescriptions was similar in both settings 1997–2001 (by 36% in Australia; 40% in Manitoba) and declined in both settings 2001–2005 (by 55% in Australia; 53% in Manitoba) and 2005–2008 (by 28% in Australia; 23% in Manitoba). The “crossover” between MHT and bisphosphonate use (i.e., the year in which the number of bisphosphonate prescriptions dispensed exceeded those of MHT) occurred in 2003 in Australia and 2004 in Manitoba. With respect to bisphosphonates, in both settings, dispensing increased from 1996, and prescription numbers reached maximum levels in 2005 in Manitoba and 2007 in Australia. Bisphosphonate use then plateaued (or slightly declined) at least until 2008 in both settings. The relative increase in the number of dispensed bisphosphonate prescriptions was higher in Australia than in Manitoba 1997–2001 (714% in Australia; 360% in Manitoba) and 2000–2005 (260% in Australia; 125% in Manitoba). Bisphosphonate use was reasonably stable in both settings 2005–2008.
Age-specific MHT and bisphosphonate dispensing trends and changes, 2003–2008 (Australia) and 1998–2008 (Manitoba)
Broadly similar patterns of use over time in MHT and bisphosphonate prescription numbers were observed in different age groups for the two settings between 2003 and 2008, the period for which a comparison was possible (Fig. 2). In both settings, for women in their 50s, MHT dispensing was consistently higher than that of bisphosphonates over the entire period. For women in their 60s, initially, the total numbers of MHT prescriptions were higher than those for bisphosphonates in both settings. MHT dispensing dropped, and that of bisphosphonates increased until they “crossed over” in 2006 in Australia and 2004 in Manitoba. MHT prescription numbers, 2003 to 2008, were always lower than those for bisphosphonates for both Australian and Manitoban women in their 70s and 80s. Percentage changes in MHT and bisphosphonate prescription numbers 1998–2003 for Manitoba and 2003–2008 for both Australia and Manitoba (Table 1) were calculated based on the age-specific trends described in Figure 2.

Total number of dispensed MHT and bisphosphonate prescriptions by 10-year age groups in women aged ≥50 years in
Percentage Change in the Use of Menopausal Hormone Therapy and Bisphosphonates in Australia and Manitoba, by 10-Year Age Groups During 1998–2003 and 2003–2008
In concession cardholders only (see main text).
CI, confidence interval; MHT, menopausal hormone therapy.
Data sources: All Pharmaceutical Benefits Scheme databases for Australia; Drug Program Information Network for Manitoba, Canada.
In the 5-year period 2003–2008, MHT dispensing numbers declined among all age groups in both settings. With respect to bisphosphonate dispensing 1998–2003, Manitoban women in their 80s showed the largest increase in prescription numbers, followed by women in their 50s, 60s, and 70s, respectively, relative to a low baseline level. Between 2003 and 2008, in Australia and Manitoba, women in their 50s were the only group to show a drop in the number of dispensed bisphosphonate prescriptions. For all other age groups, bisphosphonate prescription numbers continued to increase in both settings 2003–2008 with women ≥80 years showing the largest increase. In the 10-year period 1998–2008 in Manitoba, women in their 50s were the only group in which a decline in bisphosphonate dispensing was observed 2003–2008 despite an increase in dispensing 1998–2003 (Table 1).
Annual percentage change in bisphosphonate dispensing rates 2003–2008
Between 2003 and 2008, on average there were 717 bisphosphonate prescriptions per year per 1,000 Australian women aged ≥50 years, compared with 496 in Manitoba (Fig. 3). Over this period, the average age-specific rates were 150, 576, 1,371, and 1,885 prescriptions per year for Australian women in their 50s, 60s, 70s, and 80s, respectively, compared with rates of 133, 396, 800, and 1,153 prescriptions for Manitoban women in the corresponding age groups. Although the absolute age-specific rates were higher for Australia in all age groups, changes in age-specific bisphosphonate dispensing rates over 2003–2008 were similar for the two countries (Fig. 3).
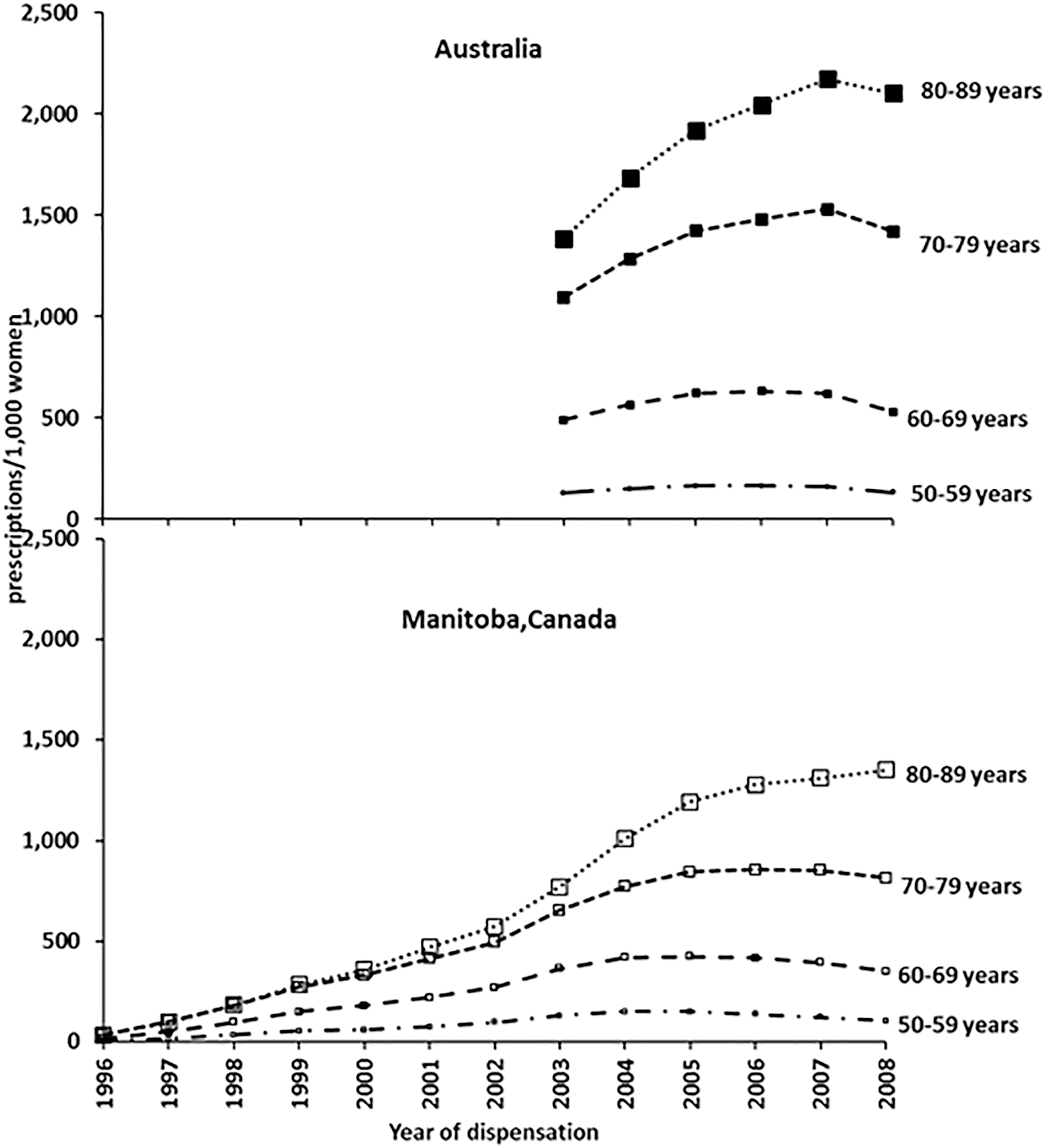
Age-specific bisphosphonate prescriptions/1,000 women by 10-year age groups in women aged ≥50 years in Australia and Manitoba, Canada. ▪ bisphosphonate prescriptions (Australia); □ bisphosphonate prescriptions (Manitoba). Data sources: The PBS database (for Australia) and the DPIN database (for Manitoba, Canada). All included preparations are listed in Supplementary Data S2.
For Australian women in their 50s, the dispensing rate in 2008 was comparable with the rate in 2003. Between 2003 and 2008, dispensing rates estimated by regression modeling increased annually by 2%, 5.5%, and 8.7% on average for Australian women in their 60s, 70s, and 80s, respectively (p < 0.001 for differences between age groups). In Manitoba, bisphosphonate dispensing rates in 2008 were 23.2% lower than those in 2003 for women in their 50s. On average, the model-predicted bisphosphonate dispensing rates fell annually by 5.1% for Manitoban women in their 50s, were unchanged for women in their 60s, and increased by 4.1% and 10.9% for women in their 70s and 80s, respectively, during this period (p < 0.001 for differences between age groups).
Discussion
Key findings
We compared dispensed MHT and bisphosphonate prescriptions in Australia and Manitoba, for women 50 to ≥80 years from 2003 to 2008 in Australia and 1996 to 2008 in Canada and found similar patterns in the overall and age-specific trends in use in both countries. In both settings, the number of dispensed MHT prescriptions increased from 1996 until 2001, reaching a maximum just before the initial findings from the WHI study in 2002. Thereafter, MHT prescription numbers declined substantially. Between 2003 and 2008, MHT prescription numbers declined among all age groups in both settings, with the highest percentage declines among women in their 50s. Our estimates of the decline in dispensed MHT prescriptions 2001–2008 (67% in Australia; 64% in Manitoba) are in agreement with other reports for Australia and Canada. 12 –14,41 Similar declines in MHT dispensing after 2002 have been reported in other developed countries. 8 –11
Where age-specific data were available (2003–2008 for Australia; 1996–2008 for Manitoba), in both settings, the bisphosphonate dispensing rate was lower for women in their 50s and generally increased with age. Changes in the annual rates of bisphosphonate dispensing also showed similar patterns by age, 2003–2008, for both settings, although the absolute rates were higher for Australia compared with Manitoba, for all the age groups examined. Between 1998 and 2003, there was a large increase in bisphosphonate use among women in their 50s in Manitoba, but after 2003 rates stabilized. Estimated bisphosphonate dispensing rates for women in their 50s in 2008 were similar to those in 2003 for Australia and were 23% lower in 2008 than in 2003 for Manitoba. These findings suggest that the decline in MHT use after 2001 and the substantial increase in bisphosphonate use over a broadly similar period occurred for the most part in women from different age groups. Our findings for age-specific dispensing of bisphosphonates are in line with lower cost-effectiveness for prevention of fractures among low-risk younger women.
Study findings in relation to guidelines for the use of MHT
Our results show that MHT dispensations were highest in younger postmenopausal women, likely to benefit most from its use. This finding is consistent with guidelines by key policy organizations/agencies that were updated more recently in view of new data becoming available from longer follow-up of the WHI trial and observational study. 42 The revised global consensus statement on MHT (2016) 7 recommends that MHT be used by women symptomatic for vasomotor symptoms before the age of 60 years, as benefits are more likely to outweigh risks, that MHT should be individualized and the benefit/risk profile reassessed annually. Similar guidelines were also recommended in the position statement by the North American Menopause Society (NAMS) on the use of MHT for management of menopausal symptoms and for the prevention of chronic conditions. 6 This position statement was endorsed by both the Australasian and Canadian Menopause Society. The US Preventative Services Task Force (USPSTF) in 2017 43 evaluated the evidence around the use of systemic MHT for prevention of chronic conditions rather than alleviation of menopausal symptoms. Their concluding statement was that neither combined MHT nor estrogen-only therapy held a net benefit for the primary prevention of chronic conditions (including osteoporosis and osteoporotic fractures). The observed decline in MHT prescriptions in older age groups is concurrent with the increase in bisphosphonate prescribing for women in their 70s and 80s, and appears to accord with recommendations that MHT should not be used for the primary prevention of chronic conditions. It should be noted that recommendations prevalent in both Australia and Canada, in relation to the use of MHT for the management of menopausal symptoms and for the prevention of osteoporosis, 24 were broadly similar to the updated guidelines mentioned above.
Guidelines for the management of osteoporosis in relation to MHT and bisphosphonates
Guidelines for use of MHT for the management of osteoporosis in postmenopausal women have also been revised by key policy organizations in both Australia and Canada. In 2004, the Therapeutic Goods Administration in Australia recommended against MHT for the long-term prevention or treatment of any disease, including osteoporosis. 2 In 2004, the Osteoporosis Australia guidelines recommended bisphosphonates as a treatment option for postmenopausal women with established osteoporosis and as a preventative measure in women with significant osteopenia; MHT as first-line therapy for osteoporosis was recommended only after balancing the risks and benefits. Guidelines (2010) from the Royal Australian College of General Practitioners also endorsed the use of bisphosphonates as first-line therapy but supported the use of estrogen-only MHT among postmenopausal women, after a rational consideration of the risks and benefits. 44 The Osteoporosis Society of Canada guidelines, as published in 2002 (based on the data from the pre-WHI era), recommended estrogen and combination hormone therapies as first-line therapy for the prevention, and second-line therapy for the treatment of postmenopausal osteoporosis. Bisphosphonates and raloxifene were also recommended as first-line therapies for its prevention and treatment. Osteoporosis Canada Guidelines (2010) support the use of pharmacological therapy based on an individual's absolute risk of osteoporosis-related fractures. Bisphosphonate use in fracture prevention is recommended for high-risk women, while MHT use is indicated for women with vasomotor symptoms who also require treatment for osteoporosis. 24
In Australia, bisphosphonates are reimbursed under the PBS for the treatment of established osteoporosis in women with a history of fractures due to minimal trauma, or if bone mineral density (measured as the T-score) is < −3.0 for women aged >70 years. The bone mineral density indication first came into effect in 2007 and subsequently changed in 2012 to include individuals aged >70 years with T-score ≤ −2.5. In Manitoba, under the Pharmacare formulary policy, bisphosphonates were indicated for both the prevention and treatment of postmenopausal osteoporosis until 2005. In late 2005, all bisphosphonates were recategorized, indicated for use only in people with established osteoporosis. It is likely that the changes in recommendations, for both Australia and Manitoba, could have influenced the changes in MHT and bisphosphonate use observed in the two settings. For example, the changed indications for bisphosphonate use in the Manitoba formulary in late 2005, restricting its use for established osteoporosis, appear to be reflected in the continuous rise in bisphosphonate use until 2005, followed by a fall in rates of dispensing among all age groups except those aged ≥80 years.
Impact of once-a-week bisphosphonates
Another major event that occurred over the study period is the release of once-a-week formulations of bisphosphonates in 2001 in Australia and 2002 in Canada. These considerably facilitated bisphosphonate uptake and compliance with therapy, since they were more convenient and associated with fewer side effects (e.g., damage to the gastroesophageal mucosa 45 ) compared with the daily formulations. Potentially in line with this development, we observed substantial population-level increases in bisphosphonate uptake after 2001. This trend continued until 2007 in Australia and 2005 in Canada when the changes in prescribing indications came into effect as discussed above.
The extent of prescribing AOMs in any population is also dependent on the prevalence of osteoporosis and osteoporotic fractures in the population. In 2007, in Australia, it was estimated that ∼25% of women and 7.7% of men aged ≥50 were affected by osteoporosis. In Canada, ∼21.3% of women and 5% of men aged ≥50 had osteoporosis based on the lowest bone mineral density scores. 46 Given these differential risks, with women three to four times more likely to be affected than men, AOMs are mainly prescribed to women. In line with this, we found that 83% of prescriptions in Australia and 92% of prescriptions in Canada were prescribed to women.
Limitations and strengths of the study
Our study has several limitations, mostly related to the use of routinely collected administrative data. First, as MHT dispensing is only completely captured in the PBS database for concessional card holders, we restricted our analyses to this population. Second, because age- and sex-specific prescription data have been recorded in Australia only since mid-2002, it was not possible to compare MHT and bisphosphonate prescriptions dispensed specifically to older (and more likely postmenopausal) women, before and after the WHI trial results. Also, prescription numbers may not accurately reflect the annual trends in use of MHT/bisphosphonates in the population since an individual may receive multiple prescriptions over a year. However, although information on the number of individuals using MHT and bisphosphonate was not available for Australia, we were able to obtain data on prescription numbers and user numbers for Manitoba, which showed a high level of correlation over the study period (see Supplementary Data S1).
Another limitation is that trends in bisphosphonate use are only reported up to the year 2008, before major changes in osteoporosis care. 47 Studies from Australia, the United States, and Europe reported a substantial decline in the use of bisphosphonates after 2008. 48 –50 Although the direct causes of this trend cannot be stated with certainty, announcements by the US Federal Drug Administration regarding bisphosphonate side effects of osteonecrosis of the jaw (2005), atrial fibrillation (2007), and atypical femur fracture (2010) are thought to precede decreased use of bisphosphonates. 51 Our analyses could not, however, go beyond 2008 because of issues related to data availability for bisphosphonates (and MHT, which is the comparator) in Australia, as explained in the methods. It should also be noted that we have not accounted in detail for frequency of use. However, our period of analysis was confined to 1996–2008, before long duration formulations for bisphosphonates (e.g., 6 months) became available. Finally, we have interpreted our findings against the prevailing and changing recommendations within the study period and have not extrapolated to current prevalence of MHT.
The strengths of this study include the use of dispensing data (rather than prescription data, which may less directly reflect use) to describe and compare MHT and bisphosphonate utilization across both Australia and Manitoba and the assessment of bisphosphonate utilization in both the absolute numbers of dispensed prescriptions and as a rate. It should, however, be noted that although dispensing data are more reflective of use, they are still a proxy for medication that has actually been taken. Furthermore, we conducted validation analyses showing the national representativeness of provincial data from Manitoba (Supplementary Fig. S1 in Supplementary Data). Where validation was possible, relative changes in utilization from the Manitoban provincial data and Canadian national data were found to closely correspond. Using the Manitoba data, we found relative changes in utilization based on dispensed prescription numbers to be similar to those based on numbers of women using the preparations (Supplementary Fig. S2 in Supplementary Data S1), and dispensing rates in Manitoba per 1,000 resident adults per quarter to be consistent with a previous analysis (Supplementary Fig. S3 in Supplementary Data).
Conclusions
In this study, the patterns of dispensed MHT and bisphosphonate prescriptions 1998–2008 were found to be broadly similar for Australia and Canada. Both countries experienced a substantial decline in MHT use after the WHI findings in 2002. Both countries experienced an increase in bisphosphonate use in the early 2000s, however, compared with Canada, the proportional increase in bisphosphonate dispensing in Australia was higher. In both jurisdictions, the decline in MHT use and the substantial increase in bisphosphonate use occurred mostly in women in different age groups. The increases in bisphosphonate dispensing 2003–2008 were greater in elderly women, whereas the decreases in MHT dispensing during the same period were highest in women within a decade of menopause. Results from this study suggest that prescribing recommendations for bisphosphonates, in relation to the recommended age for use, have been adhered to, with scripts being written mainly for elderly women who are likely to benefit the most from their use.
Footnotes
Acknowledgments
We thank Ms. Grace Musto (CancerCare Manitoba) for extracting data from data files provided by Manitoba Health. We note that the results and conclusions are those of the authors, and no official endorsement by the Manitoba Health, Seniors and Active Living or other data providers is intended or should be inferred.
Author Disclosure Statement
EK has had consultancies with Merck Frosst Canada and GlaxoSmithKline. He has also received funds for travel, accommodation and meeting expenses from Merck Frosst Canada. KC is co-principal investigator of an investigator-initiated trial of cervical screening in Australia (Compass; ACTRN12613001207707 and NCT02328872), which is conducted and funded by the VCS Foundation (VCS), a government-funded health promotion charity. She is also an investigator of Compass New Zealand (ACTRN12614000714684), which was conducted and funded by Diagnostic Medlab (DML), now Auckland District Health Board. The VCS Foundation received equipment and a funding contribution from Roche Molecular Systems and Ventana USA and DML received equipment and a funding contribution for Compass from Roche Molecular Systems. However, neither KC nor her institution on her behalf (Cancer Council NSW) receives direct funding from industry for this trial or any other project. The remaining authors have no competing financial interests.
Funding Information
The first author, U.S., carried out this work as part of her PhD program. She was funded by Tour De Cure, an Australian cancer charity. Additional infrastructure and in-kind support for U.S. and her coauthors was provided by the host institution Cancer Council NSW and the collaborating institution CancerCare Manitoba.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.