
Abstract
Introduction:
Endometriosis is a burdensome chronic condition for which conservative management is often recommended when indicated. Nonetheless, some women seek care for endometriosis in the emergency department (ED). We evaluated trends in ED visits for endometriosis from 2006 to 2015.
Materials and Methods:
Nationally representative estimates of ED visits for endometriosis by women aged 18–49 were extracted from the Health Care Utilization Project Nationwide Emergency Department Sample into three cohorts by calendar years 2006–2007, 2010–2011, and 2014–Q3 2015. Visits with a principal diagnosis code of endometriosis (International Classification of Disease, 9th Edition, Clinical Modification, code 617.x) were included. Patient and hospital characteristics were compared across cohorts using analysis of variance. Trends in the proportion of ED visits ending in inpatient admission and in mean charges (2015 USD) were assessed using generalized linear models controlling for patient and hospital characteristics.
Results:
The annual number of ED visits nationally was stable at ∼15,000 visits per year during 2006–2015. From 2006–2007 to 2014–2015, the composition of ED visits shifted away from private pay (42.0% vs. 35.3%) and uninsured (23.6% vs. 16.6%) to Medicaid (26.7% vs. 40.1%) and became more concentrated in metro-teaching hospitals (33.9% vs. 51.9%) (p < 0.001 for all). Inpatient admission rates declined from 20.1% to 9.2% (p < 0.001). Mean ED charges increased from $2458 to $4953 (p < 0.001).
Conclusion:
During 2006–2015, the number of ED visits for endometriosis remained stable, the inpatient admission/transfer rate declined by half, and mean charges per visit doubled.
Introduction
Endometriosis is a chronic inflammatory condition characterized by the presence of hormonally responsive endometrial-like tissue outside of the uterus. 1 It is common, affecting an estimated 6%–10% of reproductive-aged women, and can substantially reduce quality of life largely due to pain. 2 –6 Women with endometriosis may experience severe abdominal pain, especially with menstruation, and subfertility. 1 First-line therapies for endometriosis typically involve medical management, especially oral hormonal therapies. 7 In some cases, depending on patient preferences and disease severity, surgery may be necessary. 8 Management goals for endometriosis are to control pain effectively and facilitate family planning ambitions. 8
In addition to a high symptom burden, endometriosis comes with a considerable economic burden. Research in the United States shows that women with endometriosis have higher health care utilization, direct medical costs, and indirect productivity costs than women without endometriosis both before and after their diagnosis, 9,10 whereas a European study suggests that the direct health care costs associated with endometriosis are as large as those for other serious chronic conditions, including diabetes and Crohn's disease. 11 The cost burden is driven in large part by the chronic nature of the disease and the role of surgery in both diagnosis and treatment. 12 Surgery is also not completely curative. Studies suggest that women who receive surgical treatment with endometriosis often require a repeat procedure and experience surgical complications, further compounding costs. 13,14
Emergency department (ED) visits are another component of the economic burden of endometriosis. Despite recommendations for conservative management, 8,15 ED visits for endometriosis occur and are a costly contributor to the overall economic picture of the disease. 9 However, there are no recent estimates of the number or frequency of endometriosis-related ED visits in the United States, and no evidence of whether this number has responded to changing management guidelines. 8 Insights into the population of women who receive endometriosis care in the ED could help identify and establish interventions to direct preventable ED visits to other care settings and reduce the total economic burden of endometriosis.
We analyzed a nationally representative database to evaluate trends in ED visits with a primary diagnosis of endometriosis between 2006 through the third quarter of 2015. Our objectives were to assess the number of ED visits for endometriosis over this time and to evaluate changes in hospital charges and patient characteristics.
Materials and Methods
Data
We used data from the National Emergency Department Sample (NEDS), which is developed by the Healthcare Cost and Utilization Project (HCUP). It collects data from two databases: the State Emergency Department Databases, which capture discharge information on all ED visits that do not result in an admission to the same hospital, and the State Inpatient Databases, which capture information on patients initially seen in the emergency room and then admitted to that hospital. The NEDS is the largest all-payer ED database in the United States; in 2016, there were ∼144 million ED visits nationwide represented in the NEDS after weighting. 16 The NEDS contains information about patient demographics, hospital characteristics, International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes, and ED charge amounts. For those patients admitted to the hospital after an ED visit, the NEDS also contains procedure codes and hospital charges associated with the inpatient stay. NEDS data are publicly available and completely de-identified. Thus, their use does not constitute human subjects research under the United States Federal Policy for the Protection of Human Subjects (the Common Rule) 45 CFR part 46, and consideration of this study by an institutional review board is not required.
Sample
We evaluated all ED visits recorded in the NEDS from the beginning of 2006 through the third quarter of 2015. We truncated the sample at the end of the third quarter of 2015 due to the change in the United States from ICD-9-CM to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes on October 1, 2015, which presented an opportunity for misclassification across coding systems. 17 All visits with a primary diagnosis of endometriosis (ICD-9-CM code 617.x) were included initially. Visits were excluded if the patient was <18 years, >49 years, or had a diagnosis code for malignant neoplasms of female genital organs (ICD-9-CM codes 179 and 180.0–184.9). We grouped the sample into three time-based cohorts for analysis: 2006–2007, 2010–2011, and 2014–2015 (third quarter).
Variables
Patient characteristics of interest included age, payer type for the ED visit, national quartile of ZIP code-level median household income, and the Charlson–Quan comorbidity count (calculated using diagnosis codes present on the ED visit portion of the record). 18 Payer type was organized into the following categories: private, Medicaid, uninsured, and Medicare/other/missing. In the United States, Medicaid insurance is available to low-income individuals and families, with expanded eligibility for low-income women who are pregnant and people with disabilities. Medicare is available to Americans who are at least 65 years of age and those with serious disabilities. Hospital characteristics included census region and location/teaching category (i.e., urban teaching, urban nonteaching, and rural). Outcomes of interest were total counts of ED visits across time-defined cohorts, being admitted as an inpatient to the same hospital after the ED visit, receipt of endometriosis-related surgery among those admitted (defined as hysterectomy, bladder intervention, laparoscopy, laparotomy, oophorectomy, other excision/ablation, and salpingectomy; see Supplementary Table S1 for details), and total charges for ED visits and inpatient admissions. Charge variables were inflated to 2015 USD using the hospital care component of the Personal Health Care price index. 19
Analyses
Descriptive statistics of patient and hospital characteristics for each time-period-defined cohort were calculated as counts and percentages for categorical variables and means for continuous variables and were compared across cohorts using analysis of variance. To account for changes in the U.S. population over the study period, we also calculated a rate of endometriosis-related ED admissions per 100,000 people. Regression modeling was used to compare unadjusted and adjusted outcomes across cohorts. Logistic regression models were used to analyze the likelihood of hospital admission and surgery after admission, whereas log-gamma generalized linear models were used to evaluate ED and inpatient charges. Adjusted models controlled for age category (18–29, 30–39, and 40–49 years), payer type (private, Medicaid, uninsured, or Medicare/other/missing), Charlson–Quan comorbidity count (0 or ≥1), quartile of ZIP code-level median household income, hospital census region (Northeast, Midwest, South, or West), and a combined categorical measure of hospital location and teaching status (rural, urban nonteaching, or urban teaching). The NEDS does not report a more granular measure of hospital urbanicity and teaching status. Predictive margins and average marginal effects were computed from the regression model results to estimate the unadjusted and adjusted outcome means and their differences across cohorts. All analyses accounted for the complex survey design of the NEDS using the provided sampling weights. Statistical analyses were conducted using Stata version 15.1 software (College Station, TX). Statistical significance was determined based on a two-sided alpha of 0.05.
Results
Figure 1 displays the sample selection and number of visits for each time-defined cohort. The numbers reflect national estimates based on NEDS sampling weights.

Cohort selection criteria. Sample sizes are based on weighted national estimates; numbers may not add due to rounding. ED, emergency department.
Figure 2 shows the national rate of endometriosis ED visits and the total number of ED visits for each year in the study. Although the annual number of all-cause ED visits nationally increased slightly from 2006 to 2014, the annual rate of ED visits for endometriosis remained steady at around 5.0 per 100,000 people. 20
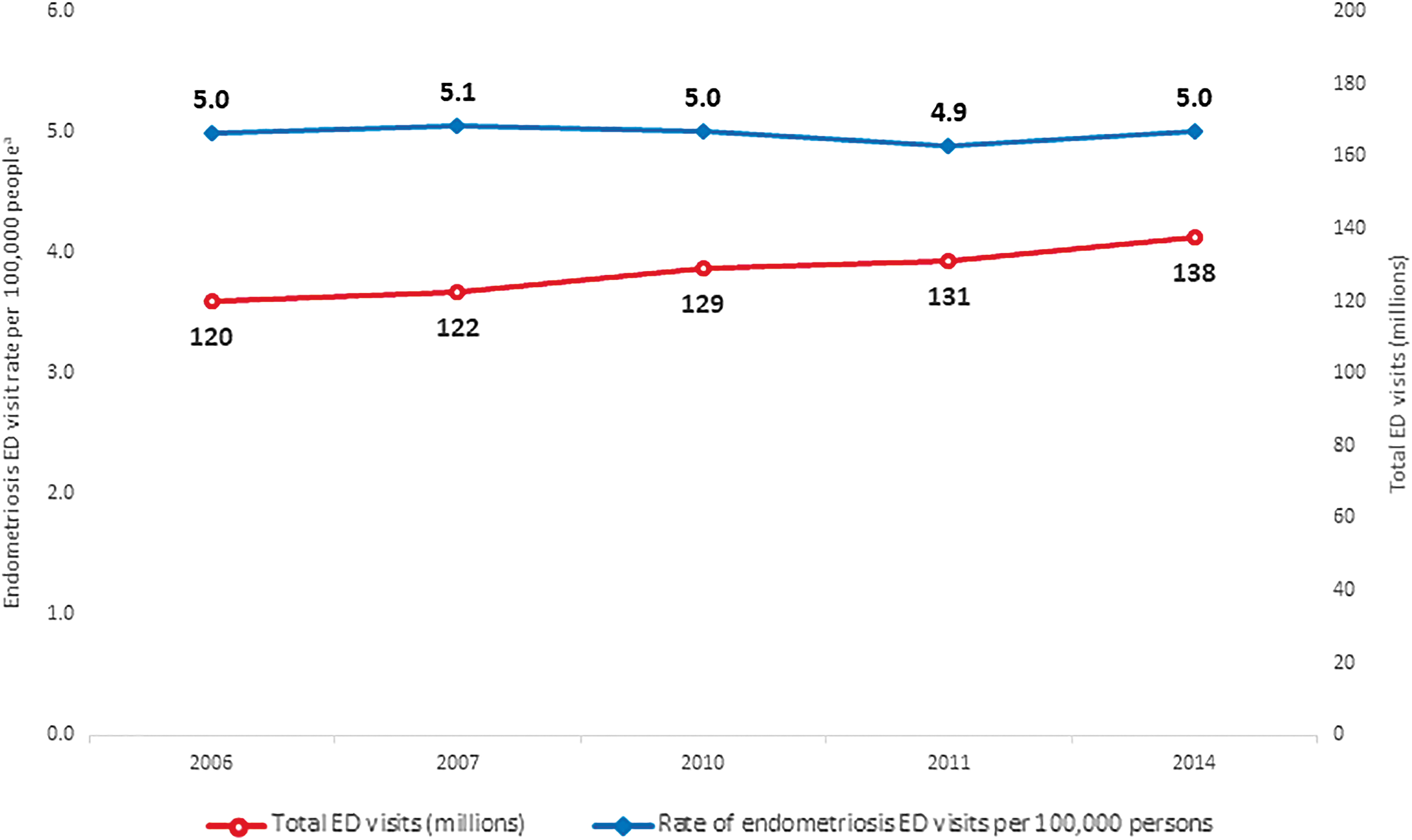
ED visits overall and endometriosis ED visit rate. aVisit rate is calculated using the national population of the United States as the denominator. Note: 2015 excluded because 2015 data were not available on the HCUPNet portal. Source: Agency for Healthcare Research. HCUPnet, Healthcare Cost and Utilization Project. 20
Patient and hospital characteristics for ED visits with a primary diagnosis of endometriosis are displayed across time-defined cohorts in Table 1. Overall, there were ∼15,000 ED visits for endometriosis per year (30,000 per 2-year cohort) over the study period. Although the number of visits remained consistent, some patient and hospital characteristics changed over time. The proportion of women aged 30–39 years old increased over time, whereas the proportion of patients aged 18–29 years decreased slightly from 56.8% to 46.5%. The share of endometriosis ED visits by patients with at least one Charlson–Quan comorbidity increased slightly over time. The mix of insurance coverage also changed, with the share of patients covered by Medicaid increasing and the shares of patients with private coverage and no coverage decreasing. Finally, the share of ED visits taking place at urban-teaching hospitals increased. Unadjusted and adjusted total ED charges increased over time (Fig. 3). In the adjusted model, the mean cost of an ED visit increased from $2,454 to $4,929 from 2006–2007 to 2014–2015 Q3.
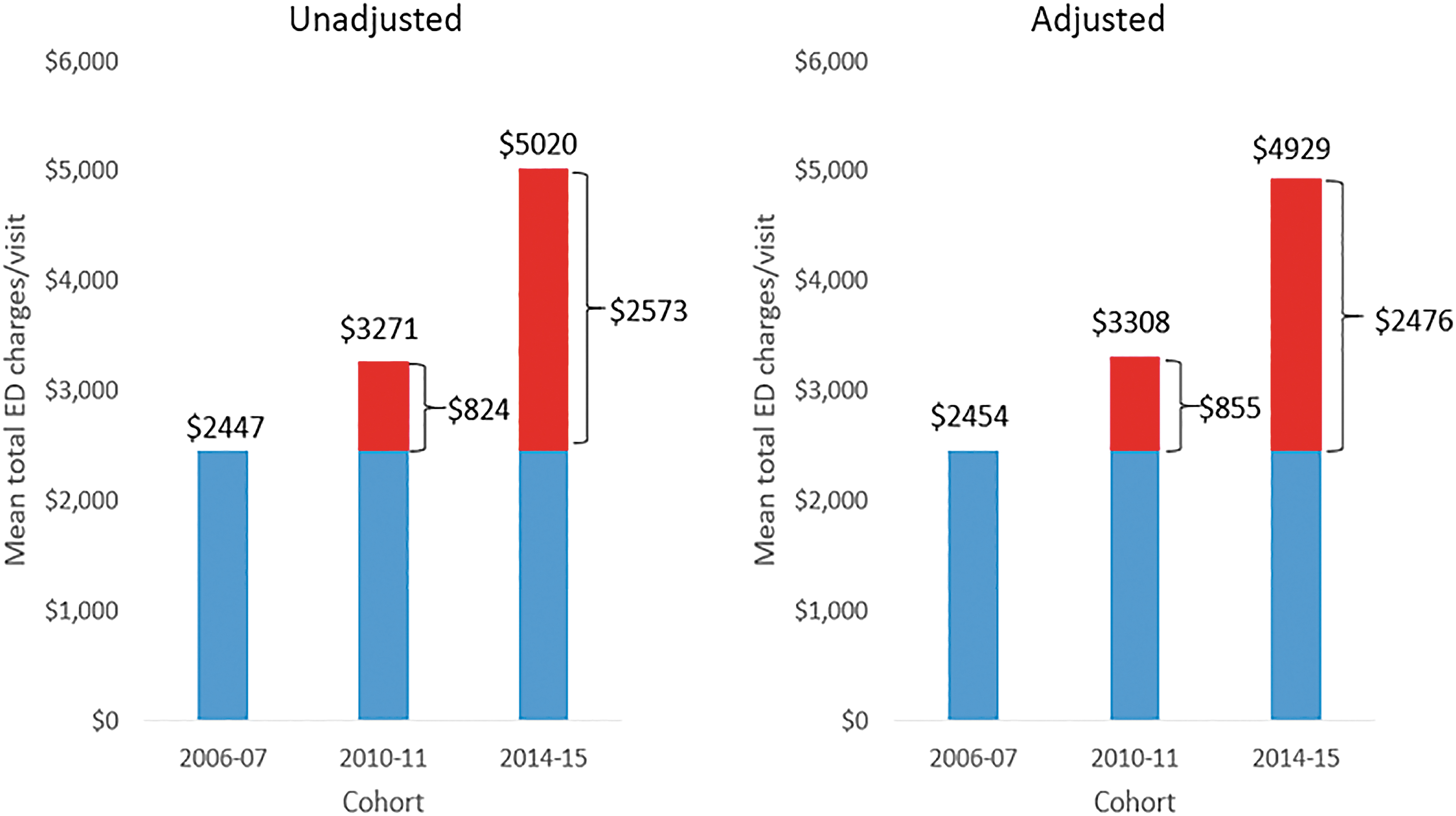
Mean total ED charges per visit. Data for 2015 cover Q1–Q3 only; values may not sum due to rounding. ED charges were inflated to 2015 USD and modeled using a log-gamma generalized linear model that accounted for survey weighting. Adjusted models controlled for age, payer type, Charlson–Quan comorbidity count, median household income quartile, hospital census region, and hospital location/teaching category. Differences relative to 2006–2007 are all statistically significantly different from zero at p < 0.05.
Patient and Hospital Characteristics of Women with an Emergency Department Visit for Endometriosis by Year of Emergency Department Visit
Proportions may not sum to 100% due to rounding.
Data for 2015 cover Q1–Q3 only.
p-values are from Pearson chi-squared tests that account for survey design.
Weighted counts are nationally representative.
The first quartile corresponds to the lowest median income, the fourth the highest.
ED, emergency department.
Over the study period, the proportion of ED visits that resulted in inpatient admissions to the same hospital fell from 20% to 9% in the adjusted model (Table 2). Among those admitted to the hospital, the proportion of patients receiving surgery decreased slightly even as adjusted estimates of mean total inpatient charges increased from $30,395 to $45,008 between 2006–2007 and 2014–2015 Q3.
Trends in Inpatient Admission and Any Surgery and Total Inpatient Charges Per Year Conditional on Inpatient Admission
Data for 2015 cover Q1–Q3 only; values may not sum due to rounding.
Weighted counts are nationally representative.
Any inpatient surgery modeled using logistic regression that accounted for survey weighting.
Adjusted models controlled for age, payer type, Charlson–Quan comorbidity count, median household income quartile, hospital census region, and hospital location/teaching category.
Any inpatient surgery includes hysterectomy, bladder intervention, laparoscopy, laparotomy, oophorectomy, other excision/ablation, and salpingectomy.
Mean total inpatient charges modeled using a log-gamma generalized linear model that accounted for survey weighting.
CI, confidence interval.
Discussion
From 2006 to 2015, the national frequency of ED visits for endometriosis remained stable even as the total number of all-cause ED visits increased slightly. The proportion of ED visits resulting in an inpatient admission decreased, as did the proportion of those admitted who received surgery. Simultaneously, the mean total ED and inpatient charges increased steadily even after adjustment for confounders. The characteristics of women with endometriosis visiting the ED also changed over the study period. Over time, women became slightly older, more likely to have at least one comorbidity, and more likely to have Medicaid insurance coverage with corresponding decreases in private coverage and no coverage, as expected given the implementation of the coverage provisions of the Affordable Care Act in January, 2014. 21 There was also a progressive increase in the proportion of ED visits for endometriosis occurring at urban-teaching hospitals.
Recent clinical guidance has promoted minimally invasive outpatient procedures for endometriosis management. 8,15,22,23 A recent position statement also recommends certain procedures that should be phased out of endometriosis care, as they increase patient burden for little gain. 24 Although this guidance may have contributed to observed reductions in inpatient admissions and surgeries from the ED, it did not reduce the quantity of ED visits for endometriosis over the study period.
There are multiple possible explanations for the stable trend in ED visits that are not mutually exclusive. In general, pain is a primary driver of ED visits, 25 so ED visits could represent especially severe patients for whom conservative management is inaccessible or ineffective. It is also possible that changing patterns of insurance coverage have kept the rate of ED visits stable. A nationally representative study of all-cause ED visits from 2006 to 2014 showed that the proportion of visits covered by Medicaid increased as the proportion covered by private insurance decreased. 26 Our results show a similar trend in insurance coverage of the visits in our sample. A study of privately insured patients suggested that between 2008 and 2015 visits to non-ED urgent care settings (e.g., urgent care clinics) for low-acuity conditions increased, whereas ED use decreased. 27 It may be that patients with endometriosis, particularly those with Medicaid coverage, are not aware that alternative urgent care settings are an option, or that they do not receive adequate treatment or insurance coverage in those settings. We also do not know how many of the patients in our sample were receiving their first endometriosis diagnosis in the ED. Diagnosing endometriosis can be a challenge due to symptom overlap with other conditions, nonspecific symptoms, and limited efficacy of noninvasive diagnostic options in some cases; thus, diagnostic delays are not uncommon. 28,29 It is, therefore, possible that some patients had not previously sought care for their symptoms, or were misdiagnosed, in other care settings. Finally, it remains possible that the number of ED visits for endometriosis is decreasing, but that diagnosis or awareness has improved and so the number of visits identified as endometriosis-related has increased.
In terms of where visits were occurring, we noted a shift in the type of hospital at which most endometriosis-related ED visits took place. Over the study period, there was an increase in the proportion of visits occurring at urban-teaching hospitals and corresponding decreases in the proportions of visits to rural hospitals and to urban-nonteaching hospitals. It is likely that the concomitant ACA-related expansion in Medicaid and the acceleration in the closure of rural hospitals played roles in influencing patient flow to EDs broadly. 30,31 Although our data do not allow for accurate investigation of the reasons for this shift, further research in this area may help guide future health care policy.
It is important not to overinterpret the increases in mean inpatient charges found in this analysis. Actual payments to providers are typically much less than billed charges, and there is substantial interhospital variation in charges billed for the same inpatient stay. 32 The process by which hospitals set their charges is largely opaque, but higher charges are associated with more hospital revenues. 33 It is thus not surprising that there have been steady increases over time in both billed charges and paid amounts for inpatient admissions. 32,34
Although our analysis adds to the little that is known about the characteristics of endometriosis patients who receive care at the ED, there is still a lack of understanding about women in this population and their motivations. Future research in endometriosis should consider women who receive care in the ED, and particularly should aim to gather more details than that are available in the NEDS database, including whether the endometriosis was previously diagnosed, whether chronic management strategies had been attempted, and the patient's level of knowledge about the disease and treatment options. Qualitative research could yield important insights into why women seek endometriosis care in the ED and could provide important foundational knowledge for future research studies.
There are important strengths and limitations inherent to using the NEDS database. A key strength is that our study results are generalizable to the United States. In contrast, information contained in the NEDS is necessarily limited. The NEDS records admissions only to the same hospital, so patients who were transferred to another hospital are unobserved. The NEDS also does not track individual women over time and has no information about women with undiagnosed endometriosis or those with endometriosis-related visits coded under a different diagnosis code. The only payment information in the NEDS is hospital charges, which may not perfectly reflect reimbursed amounts or costs faced by hospitals. Our study only included visits through the third quarter of 2015 due to misclassification concerns, 17 and practice patterns may have changed since then. Finally, we have no information about why women decided to receive care in the ED as opposed to other care settings.
Conclusions
Despite evolving guidelines for endometriosis management, our findings indicate that the rate of endometriosis-related ED visits has not declined and that their associated charges increased. We posit that the frequency of endometriosis-related ED visits could be an important indicator of the quality of endometriosis care in the health system more broadly. If women are not receiving effective chronic care, we would expect a greater frequency of ED visits for endometriosis. Careful monitoring of trends in the use of the ED for endometriosis could provide important insights into the quality of endometriosis care more broadly. Finally, more research into endometriosis care in the ED setting and the women who receive it is critical to reduce the burden of endometriosis for both society and patients.
Footnotes
Acknowledgments
We thank Matthew Davis, MA, of Medicus Economics who provided medical writing and editing services in the development of this publication.
Author Disclosure Statement
The design and financial support for the study was provided by AbbVie Inc. AbbVie participated in data analysis, interpretation of data, review, and approval of the research article. S.K.A. is a research consultant for AbbVie, Inc. A.M.S. is an employee of AbbVie, Inc., and may own AbbVie stocks or stock options. A.J.E and J.C.B. are employees of Medicus Economics.
Funding Information
Received funding from AbbVie, Inc., to conduct this study.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.