
Abstract
Background:
Individuals with depression have increased nonpsychiatric health care utilization. Associations between depression and utilization have not been studied in perinatal women, despite their heightened depression risk. We examined patterns of nonpsychiatric health care utilization by symptoms of perinatal depression, expecting more frequent use of acute services while being less likely to have routine medical care.
Materials and Methods:
We identified 1,103 perinatal participants from the 2005 to 2016 National Health and Nutrition Examination Surveys. The Patient Health Questionnaire was used to identify depression (score ≥10). We evaluated associations between perinatal depressive symptoms and health care utilization using logistic models and relative excess risk due to interaction (RERI) using adjusted models with appropriate weighting to provide national estimates.
Results:
Among perinatal U.S. women, 7.3% had depressive symptoms. Relative to those without these symptoms, women experiencing depressive symptoms were younger, more impoverished, and uninsured (p < 0.05). Women with depressive symptoms, compared with those without them, had twice the odds of being without routine medical care (21.6% vs. 12.5%, adjusted odds ratio [aOR]: 2.1, 95% confidence interval [CI]: 1.1 to 4.1) and of using urgent care more frequently (26.5% vs. 15.1%, aOR: 1.9, 95% CI: 1.0 to 3.9). Depressive symptoms combined with lack of insurance generally increased the odds of not having routine care (RERI: 8.4, 95% CI: −0.5 to 17.3) and more frequent use of urgent care (RERI: 7.1, 95% CI: −2.7 to 17.0).
Conclusions:
Perinatal depression is a prevalent, high-risk illness that requires more nonpsychiatric services and increased psychiatric care. Approaches that facilitate establishing a place for routine care and decreasing acute care use are necessary.
Introduction
Depression is a common and debilitating mental illness in the United States and the leading cause of disability worldwide. 1 –3 Women are twice as likely to develop depression as men 1,3,4 and are at increased risk of new onset or relapse of depression in the perinatal period. 5,6 Depression in pregnancy, particularly when untreated, is associated with preterm delivery, abnormal birth weight babies, and neurodevelopmental delays. 7,8
In the general population, depression is associated with increased risk for medical comorbidities, including cardiovascular disease, 9 diabetes, 10 asthma, 11 and chronic pain. 12 It is unclear whether depression precedes and/or leads to medical comorbidities, 13 whether medical comorbid conditions contribute to depression, 14 or some combination of the two. 15 However, we do know that patients with depression use health care services more frequently than those without it. 11 This increased utilization includes nonmental health services such as visits to acute care medical facilities; however, people with depression are also less likely to use preventative or routine services, which have been shown to reduce overall health care utilization, improve patient outcomes, and chronic disease illness burden, while also decreasing associated costs. 9,16 –18
Even without depression, perinatal women are at risk for these medical comorbidities. 19 Troublingly, the rates of mental health treatment are lower among women with perinatal depression than adults in the general population, 20 –23 so that women with perinatal depression may have a compounded risk for medical comorbidities. This likely affects their use of health care, but the extent to which it has an impact remains largely unknown. If trends follow, perinatal women with depression may use fewer preventative services and more acute care services, which may contribute to poor patient outcomes and rising health care costs. 24,25 Therefore, it is important to understand the association of depression and health care utilization, including the types of use, in pregnancy and postpartum.
This study compared use of health care, specifically use of routine and acute services, and associated factors between women with and without symptoms of depression in pregnancy and postpartum by using a nationally representative sample. We hypothesized that perinatal women with depressive symptoms would be less likely to have a place to go for routine care and use urgent services more frequently than perinatal women without depressive symptoms.
Materials and Methods
Data source and participants
We conducted cross-sectional analyses by using publicly available data from the 2005 to 2016 National Health and Nutrition Examination Survey (NHANES). 26,27 This is an annual survey that collects interview, examination, laboratory, and physiological measures on participants across the country conducted by the National Center for Health Statistics and CDC. The survey included ∼5,000 civilians chosen from 15 randomly selected locations and response rates were 60% or more. The University of Massachusetts Medical School Institutional Review Board considered this study exempt from review, as the data are publicly available for use.
We included women aged 20–44 years determined to be pregnant or within 1-year postpartum, as perinatal depression is defined by the American College of Obstetricians and Gynecologists (ACOG) as a major or minor episode of depression at any point during pregnancy or in the first 12 months postpartum. 28 Pregnancy was determined by self-report or urine screen. Women were considered postpartum if they reported 12 months or fewer to the question, “How many months ago did you have a baby?” We identified 1,258 women who met our inclusion criteria. The final sample included those who also completed the Patient Health Questionnaire (PHQ-9) and was 1,103 (87.7%) women.
Measure of perinatal depression
We used the PHQ-9 to categorize depressive symptoms. 29 The PHQ-9 is a nine-item, self-report screening tool that assesses depressive symptoms over the preceding 2 weeks. It assesses depressed mood, anhedonia, sleep, appetite, guilt or hopelessness, concentration, lethargy or restlessness, and suicidal thoughts or behaviors. Participants rated each item on a scale of 0–3, with 0 meaning “Not at all” and 3 “Nearly every day.” Scores range from 0 to 27 and we considered scores ≥10 as positive for depression symptoms. This cutoff has been well validated with a high sensitivity and specificity 29,30 and has good concordance with other commonly used tools to screen for perinatal depression (e.g., Edinburgh Postnatal Depression Scale [EPDS]) 31 that were unavailable in the NHANES. In pregnant women, the EPDS (score ≥13) has a 79% rate of correct identification of depression versus the PHQ-9 (score ≥10) with a rate of 74%; in postpartum women, both the EPDS and PHQ-9 have 84% rates of correct identification of depression. 31 The PHQ-9 has been used to identify individuals with depression in numerous other studies using the NHANES data. 3,23
Measures of outcome
The outcome measures were those of health care utilization. The NHANES contains the Hospital Utilization and Access to Care questionnaire (HUQ), with participant-reported data on health status and health care accessibility and utilization. Specifically, we were interested in nonmental health-based care and thus chose two questions from the HUQ that we thought best approximated nonmental health care utilization: (1) whether the participant had a place to go for routine care; and (2) the type of care (acute vs. routine) used most often. We chose these because: (1) generally, “routine” care refers to use of a primary care or related services, provided in a nonmental health setting even if the patient is seeking mental health services; and (2) urgent or emergency care facilities, which, although they serve patients with a variety of illnesses, are generally nonmental health care locations, despite the fact that many visits are behavioral health related. These questions did not explicitly ask participants to exclude mental health care visits or locations in their responses, but mental health care was asked about as a separate and distinct question in the same questionnaire, likely indicating to participants to think about it separately. Therefore, we felt that these two HUQ questions were adequate approximations of nonmental health care use.
For the question regarding routine care, participants were asked, “Is there a place that you usually go when you are sick or you need advice about your health?” We categorized responses (yes, there is no place, there is more than one place) as the presence (yes and there is more than one place) or absence (there is no place) of a place for routine care. Regarding acute care use, participants were asked, “What kind of place do you go to most often—a clinic, doctor's office, emergency room, or some other place?” We dichotomized responses (clinic or health center, doctor's office or health maintenance organization, hospital emergency room, hospital outpatient department) into tendency to use urgent/emergent care more (hospital emergency room) or not (all other options).
Covariates
Several other demographic and clinical variables were examined, including: age in years (20–25, 26–34, 35–44), race/ethnicity (Mexican American/other Hispanic, non-Hispanic white, non-Hispanic black, other race/multi-racial), primary language (English, Spanish, other), education (less than high school, high school graduate/general education diploma, some college or associates degree, college graduate or above), marital status (married/living with partner or widowed/divorced/separated/never married), and poverty-to-income ratio (<1.00/below the poverty line, 1.00–1.99, 2.00 or more). We examined health insurance status (currently uninsured, current coverage but any time without coverage in the past 12 months, continuous insurance coverage for the past 12 months), the effects of multiparity by using women's reports of prior pregnancies (1, 2, 3, or ≥4 pregnancies), gestational age, and number of months postpartum. We used additional questions within the HUQ about health status, asking participants to rank themselves on a 1–5 scale of their general health (1 being poor, 5 excellent) and about use of mental health care in the past year (yes/no). Other clinical factors such as chronic diseases common to these populations (e.g., asthma, elevated blood pressure, diabetes, obesity, arthritis, cancer), prescription medication use (antidepressants, antianxiety, opioids), and substance abuse (cigarette use, alcohol, other drugs) were also evaluated.
Based on prior research 4,23 and using causal diagrams, 32 we identified potential known confounding covariates to examine in our study. We also identified insurance status and mental health care use as potential modifiers of how depression affects health care utilization.
Statistical analyses
Analyses were completed by using weights, strata, and sampling units to account for the complex survey design 33 and, thus, results are nationally representative. Demographic and clinical variables were compared between depressive and non-depressive perinatal groups, using Chi-square or t-tests where appropriate. Univariate relationships that can exhibit strong age effects were standardized for age. 34 Logistic regression models were used to estimate crude and adjusted odds ratios (aORs) and 95% confidence intervals (CIs) of primary care use and urgent/emergent care use for symptoms of perinatal depression versus no symptoms. All models were adjusted for age, education, poverty-to-income ratio, race/ethnicity, marital status, and substance use. We determined which covariates to include as confounders in the model by using a manual and iterative process, examining the effects of each potential confounder on the total effect estimate. We also included those covariates considered pertinent from the literature. 4,23
We examined the effects of interaction between depressive symptoms and two modifiers: insurance status and mental health care use. We used the properties of additive effect measure modification to estimate relative excess risk due to interaction (RERI) in estimating how total aORs may change based on a combination of exposure (depression) and each modifier (insurance or mental health care use). The RERI is the difference between what we would expect to see without excess risk due to interaction (simple sum of the independent aORs of each exposure) and the actual, observed joint effects aOR:
Taking lack of insurance as an example, aOR11 is the aOR of being exposed to depression and lacking insurance, aOR10 is being exposed only to depression, and aOR01 is only lacking insurance. The expected joint effects are the sum of the independent contributions of depression and lack of insurance, and equate to the total anticipated aOR, should no biological interaction be present. If this were the case, the RERI would equal 0.
Results
Study sample overview
Of the population of perinatal women in our U.S. sample, ∼7.3% were found to have symptoms of depression (Table 1). Compared with women without symptoms, women with perinatal depressive symptoms were more likely to be younger, not married or partnered, have received less education, and have a lower poverty-to-income ratio (all p < 0.05).
Demographic Characteristics of Perinatal Women With and Without Depression
Data presented in table are weighted percentages. Variables with missing values: language (n = 75), marital status (n = 1), poverty-to-income ratio (n = 71).
Depression was defined as a total PHQ-9 score of ≥10 points.
Total percentages may not sum to 100.0% because of rounding.
p-Value <0.05.
Standardized for age.
GED, general education diploma; PHQ-9, Patient Health Questionnaire.
Clinical characteristics
All women had similar distributions of perinatal status (pregnant vs. postpartum), gestational age, and months postpartum (Table 2). Compared with women without symptoms, women with depressive symptoms had higher rates of being uninsured, having fair or poor health status, and of utilizing mental health care services (all, p < 0.01). Almost one in five women reported being pregnant four or more times earlier, and this increased to almost one in three in those with symptoms of depression. Women with depressive symptoms tended to use all types of prescription medications more and suffered from all comorbid medical conditions more frequently than those without, though only elevated blood pressure was statistically greater in the depressive group (p < 0.05). One in four also reported using a substance or non-prescribed drug during the prior 30 days. Women with symptoms of depression reported higher rates of substance use, with almost half of the group reporting use of some substance relative to one-quarter of the women without depression (p < 0.001).
Clinical Characteristics of Perinatal Women With and Without Depression
Data presented in table are weighted percentages and means. Variables with missing values: gestational age (n = 320, data not collected for last 2 cycles), months postpartum (n = 146, data not collected for first cycle), health insurance (n = 2), number of prior pregnancies (n = 2), health status (n = 1), asthma (n = 8), elevated blood pressure (n = 2), cancer (n = 1), cigarettes (n = 1), alcohol (n = 79), other drugs (n = 22), medications (n = 140, data not collected in last cycle).
Depression was defined as a total PHQ-9 score of ≥10 points.
Total percentages may not sum to 100.0% because of rounding.
p-Value <0.05.
Does not include current pregnancy.
Standardized for age.
SE, standard error.
Health care utilization
Women with perinatal depression symptoms had different health care utilization patterns than those without depressive symptoms (Table 3). After adjusting for potentially confounding covariates, women in the depressive group had twice the odds of having no routine place to go for care (aOR: 2.1, 95% CI: 1.1 to 4.1) and of using urgent or emergent care more often than non-urgent care (aOR: 1.9, 95% CI: 1.0 to 3.9) than those without depression.
Association Between Depression and Health Care Utilization Variables Among Perinatal Women in the United States
Data presented in table were generated by using weighted data. ORs are estimated by using logistic regression, comparing perinatal women with and without depression. The time frame for both outcomes is use in the past year.
Depression was defined as a total PHQ-9 score of 10 points or more.
Adjusted for age, education level, poverty-to-income ratio, marital status, race/ethnicity, and substance use.
p-value <0.05.
aOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio.
Figure 1 shows the RERI of 8.4 (95% CI: −0.5 to 17.3), representing the relative excess risk of having no routine place for care due to the interaction between depression and lack of insurance. The RERI of using urgent/emergent care due the same interaction was found to be 7.1 (95% CI: −2.7 to 17.0). The interaction of mental health care use and depression symptoms showed similar trends and excess risk due to interaction, but with less precision (data not shown).
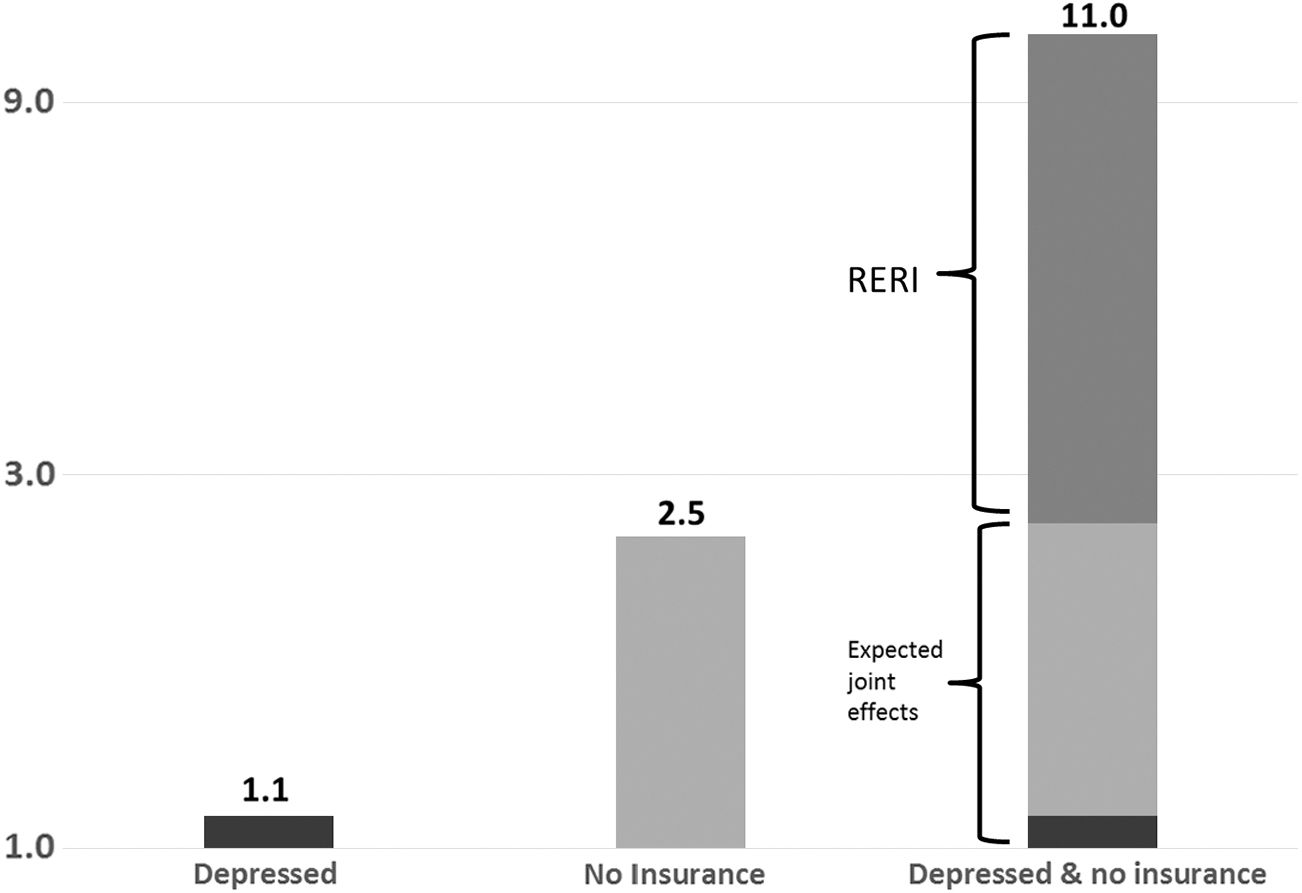
The interaction between depression and insurance status on perinatal women's having no place to go for routine care. Data presented in figure were generated by using weighted data. Scale is in adjusted odds ratios, adjusted for age, education level, poverty-to-income ratio, marital status, race/ethnicity, and substance use. aOR represents the likelihood that a woman will not have a place for routine care. Non-depressed and insured are used as the reference, with these women having a 1.0 aOR of not having a routine place for care. The black bar and light grey bars represent the main effects of depression and lack of insurance, respectively, on the aOR. Expected joint effects are the sum of the independent contributions of depression and lack of insurance, and equate to the total anticipated aOR, should no biological interaction be present. RERI is the additional effects to the total aOR due to the interaction between depression and lack of insurance. RERI = 8.4 (95% CI: −0.5 to 17.3). aOR, adjusted odds ratio; CI, confidence interval; RERI, relative excess risk due to interaction.
Discussion
Using the most recently available NHANES data, we found that perinatal women with symptoms of depression tended to have poorer overall health, based on their comorbidities and self-reported health status, versus those without perinatal depressive symptoms. Perinatal women with depressive symptoms were less likely to have a place for routine care and more likely to use acute care services over non-acute than women without symptoms, and not having insurance appeared to increase this association. Despite having higher mental health care utilization rates than those without depressive symptoms, rates of utilization were lower than what is estimated nationally for perinatal women with depression 4,20,23 and this was associated with increased odds of potentially inappropriate health care use, meaning greater use of urgent care and less use of routine care.
We found that 7.3% of perinatal women in our nationally representative U.S. sample suffer from symptoms of depression. This number is consistent, though on the lower end, with other estimates. 5,6,35 Antidepressant and mental health care use were generally low in the depression group. These findings suggest that, despite the increased medical and media attention around perinatal depression, it is possible that many women are still not being detected and/or treated. Although there is a dearth of data on the proportion of practices screening, ACOG and other organizations recommend screening for perinatal depression at least once in the perinatal period. 36 The American Academy of Pediatrics recommends screening mothers at the 1-, 2-, 4-, and 6-month well-child visits. 37 The latter is important, as pediatric practices have unique access to the family unit in the first year and can play a pivotal role in identifying postpartum depression. Although these recommendations are a major step forward, increases in screening for depression alone are not enough to improve outcomes without subsequent coordination of care. 36,38 Thus, efforts to make mental health care available to patients and for more training of obstetric and pediatric providers in how to appropriately respond to a positive depression screen are imperative. In obstetric settings, implementation of practice workflows that detail exactly how providers should manage perinatal depression, including detection, assessment, and treatment until symptom remission, is an effective approach. 38,39 Currently, screening rates for perinatal depression are highly variable and dependent on the available resources, 21 but there is no doubt that increasing awareness of screening and subsequent follow-up care recommendations from professional organizations would increase the detection of perinatal depression in all clinical settings.
Our findings support previous reports that perinatal women with depressive symptoms are a high-risk pregnancy population. Our data are consistent with prior studies demonstrating that women with greater health disparities, such as racial/ethnic minorities or socioeconomic disadvantages, are at increased risk for perinatal depression. 40,41 Other high-risk behaviors such as substance use were alarmingly high in our depression group, especially when compared with the entire sample, which mirrors previous findings. 42,43 Also consistent with the literature, 44 we found that women with more prior pregnancies were also at higher risk for perinatal depression symptoms than those with fewer. As expected, 13 –15 rates of physical comorbidities were higher in our perinatal depressive group across the board than those without symptoms of depression. These findings suggest that the link between physical and mental health is very important during the perinatal period, reaffirming the importance of integrated models of care.
Despite being both physically and psychiatrically high risk, many women with symptoms of perinatal depression do not appear to be getting the care they need, and nonmental health care utilization patterns reflect this. Depression impacts one's ability to function, including decreases in motivation and energy, which may impair the ability to plan for and adhere to care. In addition, it is often comorbid with anxiety symptoms, which affect functioning and could contribute to choices in care (e.g., choosing urgent/emergent treatment or avoiding treatment altogether when anxiety is high). Depression symptoms may create barriers or challenges to accessing care, thus making it even more important that women have a place to go for routine care established before pregnancy or symptom exacerbations. However, our data suggest that, compared with women without, women with perinatal depressive symptoms are less likely to have a place for primary care and use urgent care more frequently, which are shown to be associated with increased long-term chronic disease burden, patient costs, and stress. 45 Further, more than half of the study sample was postpartum; this is important because many women lose health insurance coverage at 6 weeks postpartum. Given that our findings also point to an intersection of perinatal depression and insurance status, studies evaluating the impact of continued insurance coverage to bridge the gap for women needing access routine or preventative health care services are warranted. Better facilitation of both routine prenatal and primary care for women with perinatal depression could, in turn, improve outcomes and decrease acute care visits. In addition, perinatal women with depression symptoms are much less likely to be insured, which appears to be associated with and potentially exacerbates inappropriate health care utilization patterns and, thus, increases costs of care. Ensuring that perinatal women are able to receive insurance will surely contribute to more primary care coverage as well. The influence of being uninsured on health care utilization patterns generally aligns with other studies that aimed at discerning moderators of depression and health care utilization, where untreated depression, level of social support, socioeconomic status, and race/ethnicity may affect the relationship between depression and rates of mental and nonmental health treatment. 9,18 Because our study spanned the role out of the Affordable Care Act (ACA), research in the post-ACA era is warranted.
There have been a few studies to date examining the interplay between perinatal depression and suboptimal utilization of nonmental health care. Therefore, our study is an important stepping stone for future work. Other strengths lie in its use of a rich and robust, nationally representative data set that allows for weighted estimates of population averages. Our study was limited to a small sample size and resulted in estimates with lowered precision. Estimates of women exhibiting symptoms of perinatal depression were likely low, as we were limited by the tools available in the data set: The PHQ-9 only measures symptoms experienced in the 2 weeks before interview. In addition, our parameterization of our nonmental health care utilization outcomes relies on many assumptions and may be limited since it did not explicitly exclude the use of mental health care as a participant's place for routine care or reason for urgent care use. However, even increased trends of use of said nonmental health care for psychiatric reasons (e.g., using the emergency department for emergent psychiatric care) are still noteworthy, as these settings may not be the most optimal place to get care. It would be helpful to be able to delineate the reason for use, or overuse, in future studies to effectively target solutions.
Our study emphasizes the fact that continuing to educate patients and providers on the importance of screening, assessment, and treatment of depression in the perinatal period is important. Given that the estimated prevalence of depression in pregnancy is on par with that of gestational diabetes and even greater postpartum, 46 our health care systems should be as equipped to identify and care for perinatal women with depression as we are for diabetes. Future work should be focused on identifying more of the variables involved in the relationship between perinatal depression and utilization of different facets of health care and determining whether decreasing acute care while increasing routine use may help to decrease health care costs. This might allow us to further understand the barriers to care and help us to provide more informed advice for women and providers. In addition, our data emphasize that insurance status plays a role in prenatal physical and mental health.
Conclusions
Perinatal depression is common and has many downstream consequences for the mother, baby, and their family. Approaches focused on helping perinatal women establish a place for routine care, with the goal of decreasing acute care use, are needed. Such approaches, including establishing and maintaining insurance coverage and aiding front-line providers in detecting, assessing, and managing perinatal depression, may help improve maternal and child health care and outcomes and decrease health care costs.
Footnotes
Author Disclosure Statement
Dr. Byatt is currently receiving grant funding from the National Institute of Health (R41 MH113381) for a project related to perinatal depression. Dr. Byatt received and/or receives salary and/or funding support from Massachusetts Department of Mental Health via the Massachusetts Child Psychiatry Access Program for Moms (MCPAP for Moms). Dr. Byatt is the founding and current statewide Medical Director of MCPAP for Moms. Dr. Byatt is also the Executive Director of Lifeline4Moms. Dr. Byatt is a member of the American College of Obstetricians and Gynecologists' Expert Work Group on Maternal Mental Health. She has served on the Perinatal Depression Advisory Board for the Janssen Disease Interception Accelerator Program, the Physician Advisory Board for Sage Therapeutics, and is a Council Member of the Gerson Lehrman Group. She has also received speaking honoraria from and serves as a consultant for Sage Therapeutics or their agents and Ovia Health. Dr. Byatt has also received honoraria from Medscape and Miller Medical Communications. The remaining authors have no conflicts to disclose.
Funding Information
This study was supported by the CDC (Grant No. U01DP006093), and an award from the UMass Medical School Center for Clinical and Translational Science TL1 Training Program (Grant No. TL1TR001454).