
Abstract
Background:
Maternal morbidity and mortality are key indicators of women's health status and quality of care. Maternal morbidity and mortality are high and rising in the United States. There has been no evaluation of severe maternal morbidity and mortality among veteran women, although population characteristics suggest that they may be at risk. This study aimed to evaluate a surveillance methodology at the U.S. Department of Veterans Affairs (VA) and describe the characteristics of women veterans who experienced severe maternal morbidity events.
Materials and Methods:
The study sample derived from a national sample of Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn veterans who were enrolled for care at the VA. The surveillance methodology followed a recommended process of case identification and chart review following a standardized guide. Centers for Disease Control and Prevention (CDC) International Classification of Diseases codes for maternal morbidity were applied to billing, inpatient, and outpatient data for 9,829 pregnancies among 91,061 veteran women between January 1, 2014 and December 31, 2016. Descriptive statistics is reported.
Results:
One hundred twenty-seven pregnancies with severe maternal morbidity events were identified, 66 of which were confirmed after chart review. The positive predictive value of CDC indicators to identify cases was 0.52. High rates of mental health problems, obesity, rurality, maternal conditions, and racial discrepancies were noted among veterans who experienced severe maternal morbidity events.
Conclusions:
Severe maternal morbidity affects a significant number of veteran women. Systematic reporting of pregnancy outcomes and a multidisciplinary review committee would improve surveillance and case management at the VA. The VA is uniquely positioned to develop innovative comanagement strategies, especially in the area of perinatal mental health.
Introduction
Maternal morbidity and mortality are key indicators of women's health status and quality of care. Maternal morbidity and mortality have been rising in the United States for the last three decades 1 rather than following the global trend downwards. 2 Currently maternal mortality is 2–6 times higher than in other high income countries, 2 despite more per capita health care spending. 3,4 For every woman that dies in the United States, around 100 more experience life-threatening pregnancy-related events. 5 Evaluation of these near miss events, termed severe maternal morbidity, expands the opportunity to address factors that contribute to maternal death and disability.
In a joint consensus statement, the American College of Obstetricians and Gynecologists and the Society of Maternal Fetal Medicine have recommended a case identification and chart review process for all severe maternal morbidity events. 6 This recommendation acknowledges that severe maternal morbidity merits review and that review can lead to improved outcomes. It further acknowledges that, unlike mortality, severe maternal morbidity can be difficult to identify given that some events arise from unavoidable maternal conditions. A systematic review of these maternal “near miss” events suggests that reducing preventable maternal morbidity depends on knowing the characteristics of specific populations within their local health care context. 7 Responding to this recommendation, this study aimed to implement a severe maternal morbidity case identification process among a cohort of women veterans and report descriptive statistics on confirmed cases following in-depth, individual chart review.
The maternal morbidity and mortality crisis in the United States has received increasing attention from governmental and nongovernmental initiatives, popular media, and research. Despite attention, however, the problem continues to worsen, especially among black women who are 3–4 times more likely to die or be seriously harmed in pregnancy-related events than their white counterparts. 8 While the number of pregnant women who are older or obese has increased in the United States, research has consistently shown that these and other trends in maternal health do not fully account for the rise in morbidity and mortality. Leonard et al. 9 conducted an analysis of over 3.5 million California women between 2007 and 2014 to investigate the relationship between maternal characteristics (advanced maternal age, obesity, prepregnancy comorbidities, and cesarean delivery) and severe maternal morbidity. While health conditions before pregnancy and cesarean section were risk factors, they did not fully explain the continued rise in severe maternal morbidity events. 9 Kuklina et al. reported that cesarean delivery alone, and not maternal factors like age and health conditions, was associated with severe maternal morbidity nationally between 1998 and 2005. 10 Currently, around one in three babies is delivered by cesarean section in the United States, 11 nearly twice the rate that would be expected if responding to medical need alone. 12
Quality of care and access have also been investigated in relation to maternal morbidity and mortality. 13 Howell et al. reported that differences in delivery location may account for almost half (47.7%) of racial disparities in severe maternal morbidity in New York City. 14 In this study, factors such as teaching status of the hospital, nursery acuity, patient volume, and public–private ownership were all related to racial disparities in maternal outcomes. 14 Lack of services has been identified as a possible contributor to increased risk among rural women. Over half of all rural counties in the United States are currently without obstetric services. 15
The most common direct causes of maternal mortality nationally include hemorrhage, cardiovascular/coronary conditions, cardiomyopathy, infection, embolism, mental health problems (associated with an increased risk of suicide, homicide, and accidental death), and preeclamspia/eclampsia. 16 However it is estimated that over 60% of maternal deaths are preventable. 17 Patient-, provider-, facility-, and system-level factors have all been identified in relation to preventability. Modifiable patient-level factors include lack of awareness of resources and warning signs, failure to adhere to medication regimens, and psychosocial issues like disruptive family relationships, lack of social support, and unstable housing. Preventable provider-/facility- and system-level factors include lack of assessment skills, misdiagnosis, delayed treatment, poor communication, and uncoordinated services. 16
To date there has been no evaluation of severe maternal morbidity and mortality among veteran women; however, many factors that have been previously associated with maternal morbidity and mortality are more common among veterans than among civilians. For example, a higher proportion of women veterans are African American (31%) and live in rural areas (22%) than in the general population. 18 Women veterans are more likely to suffer from hypertensive disorders of pregnancy, gestational diabetes, and obesity 19 compared to their civilian peers, all conditions that may increase the risk of delivery complications. 9 Although not fully understood, it is hypothesized that this increased burden of maternal disease may arise from higher rates of preexisting medical and mental health conditions among veterans, along with a more sedentary lifestyle imposed by musculoskeletal injuries incurred during active duty service. 19
Mental health problems are also common among women veterans. As reported by Mattocks et al., one-third (32%) of pregnant veterans had one or more mental health diagnoses during or within 5 years of pregnancy and were twice as likely as nonpregnant veterans to be diagnosed with depression, anxiety, posttraumatic stress disorder, bipolar disorder, or schizophrenia. 20
System-level factors may also contribute to risk among pregnant veterans. During pregnancy, women veterans who are enrolled for care at the U.S. Department of Veterans Affairs (VA) are referred to non-VA providers for maternity care, 21 a system that creates the potential for fragmented care as women go between the VA and the community. 20,22 The non-VA providers they see may also be largely unprepared to comprehensively care for them. A 2018 Rand corporation survey conducted among New York state licensed health care professionals (n = 746) found that slightly over 2% were prepared to effectively serve the veteran population. 23 Similarly, a survey among primary care providers (n = 102) reported that the majority never or rarely ask their patients about military service, have limited knowledge of military stressors, are unaware of veteran-specific resources, and can not identify health conditions that commonly affect veterans. 24
Women veterans are the fastest growing segment of the veteran population. 18 The number of women veterans in their childbearing years more than doubled between 2000 and 2015. 18 This is the first study to evaluate severe maternal morbidity among women veterans. As such it provides an analysis of the efficacy of a case surveillance methodology at the VA and a 3-year snapshot of severe maternal morbidity cases. It provides basic insights into the benefits and challenges of maternal outcome surveillance within the VA's referred care system and suggests implications for future practice and research.
Materials and Methods
The sample for this study derives from the VA electronic health record and administrative data of veterans who separated from service after September 12, 2002. It is composed of women who served in support of Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn (OEF/OIF/OND) and enrolled for VA care after their separation from active military service. OEF/OIF/OND veterans represent around 19% of the total female veteran population. 25 This study was approved by the Institutional Review Board at the VA Connecticut Health Care System.
Severe maternal morbidity cases were identified and reviewed in the following manner. First, all pregnancies were identified from billing, inpatient, and outpatient data for a 3-year period (January 1, 2014–December 31, 2016) using a comprehensive list of all International Classification of Diseases (ICD)-9/10 pregnancy-related codes. This included all pregnancies regardless of outcome, including full-term and premature deliveries, spontaneous abortion, missed abortion, pregnancies that ended with elective termination, and ectopic pregnancy. From this list of pregnancies, cases were extracted using the 18 severe maternal morbidity indicators published by the Centers for Disease Control and Prevention (CDC). 5 This previously tested selection criteria were used instead of a suggested alternative method of identifying transfusion and intensive care unit (ICU) admission only, 6 to provide the broadest, most detailed classification system possible and to highlight cases for possible review, as has been recommended for institution-specific screening. 6 Furthermore, the CDC criteria were selected in an attempt to overcome variability in ICU admission criteria 26 that might have existed between the diverse non-VA hospitals where veteran women gave birth. These hospitals vary by geographic location, acuity level, staffing, and resources and it was therefore anticipated that ICU admission criteria could vary substantially between facilities.
Finally, in-depth chart review was performed on all pregnancies with a severe maternal morbidity code identified during the 18 months following the first pregnancy diagnosis. Although maternal morbidity is usually evaluated through the first 42 days postpartum, 26 the observation period was extended in this study to capture any cases that might have occurred beyond the 6-week postpartum time frame. Chart review was performed following a standardized guide that was based on the Severe Maternal Morbidity Reporting Form published by the Council on Patient Safety in Women's Healthcare. 27 Patient medical records were accessed through the national VA electronic health record and included multispecialty patient encounters and scanned records from non-VA providers.
Pregnancies with a severe maternal morbidity event were sorted into four categories as follows: (1) confirmed negative (complete obstetric records available that confirmed the absence of a severe maternal morbidity event), (2) presumed negative (incomplete obstetric records available but subsequent VA records confirmed a normal perinatal course without a qualifying severe maternal morbidity event), (3) confirmed positive (complete obstetric records available that confirmed the presence of a severe maternal morbidity event), and (4) presumed positive (incomplete obstetric records available but subsequent VA records confirmed a severe maternal morbidity event).
The following variables were included in the analysis: Age was determined based on age at delivery. Age was then grouped into the following categories: 22–34 and ≥35 following the typical clinical designation of advanced maternal age for women 35 and older.
Race/ethnicity was extracted from chart review based on current VA classifications. These included: White, Black or African American, Hispanic, American Indian/Alaska Native, Asian, and Native Hawaiian/Other Pacific Islander.
Residence/Rurality was based on zip code at the time of delivery. Rurality was determined using Rural Health Research Center's Rural Urban Commuting Area (RUCA) zip code approximation of census tract codes. The RUCA three-level designation (urban, rural, highly rural) is consistent with previous VA methodology. 18
Parity was identified at the time of the index pregnancy and separated into (1) primiparous women and (2) multiparous women.
Delivery mode was classified as (1) normal spontaneous vaginal delivery; (2) instrumental vaginal delivery; and (3) cesarean section. Cesarean sections were further classified as (1) primary or (2) repeat.
Gestational age at delivery was categorized as (1) 37 through 40 completed weeks, (2) ≥41 weeks, and (3) <37 weeks.
Hypertension and diabetes status were extracted from chart review and contained the following designations: (1) preeclampsia, (2) preexisting hypertension, (3) preexisting hypertension with superimposed preeclampsia, and (4) diabetes mellitus before and/or during pregnancy.
Obesity status was based on the earliest body mass index (BMI) identified following pregnancy diagnosis. Proximal prepregnancy BMIs were not consistently available. BMIs were classified as: (1) ≥30 or (2) <30.
Mental health diagnosis was based on diagnoses identified from first pregnancy diagnosis through the year following pregnancy in the VA record, the obstetric record, or both. Diagnoses were identified from in-depth chart review and included any and all mental health diagnoses mentioned in the medical record.
Substance use was classified as smoking, consuming alcohol more than “socially” or “occasionally,” or using drugs recreationally while pregnant.
Timing of event in relation to pregnancy was divided into the following three categories: (1) antepartum, (2) intrapartum/immediate postpartum, and (3) postpartum following discharge from the birth hospitalization. The postpartum category was further divided into: (1) the first week following hospital discharge, (2) the second week through the sixth week following hospital discharge, and (3) seven or more weeks following discharge.
Severe maternal morbidity was defined as any diagnosis or procedure included in the CDC ICD-9/10 list of 18 indicators. 5 Transfusion was handled in the following way. Massive transfusion was classified as: (1) confirmed if inpatient records detailed the number of units of blood products as ≥4; (2) presumed positive if confirmatory documentation from the inpatient record was missing but if there was subsequent reference to hemorrhage with interventions such as return to the operating room, use of a bakri balloon, uterine artery embolization, or coagulopathy due to blood loss; (3) negative if the inpatient recorded fewer than 4 units of blood products; and (4) presumed negative if postpartum hemorrhage was documented but no transfusion or other intervention mentioned.
Descriptive statistics was performed on all confirmed/presumed positive cases.
Results
From January 1, 2014 through December 31, 2016, 9,829 pregnancies were identified among a cohort of 91,061 women veterans. From these pregnancies, 127 severe maternal morbidity cases were extracted after applying the 18-indicator CDC ICD-9/10 diagnosis and procedure codes. Comprehensive chart review was performed on all identified cases. Sixty cases were classified as confirmed or presumed negative due to (i) no pregnancy within 18 months before event (8) or (ii) no event meeting criteria for a severe morbidity event (52). One case was removed because the electronic health record could not be accessed. These 61 cases were removed from consideration. Sixty-six cases were identified as either confirmed positive (43) or presumed positive (23). No maternal deaths were identified. No woman experienced more than one pregnancy in the time period studied. The positive predictive value (PPV) of applied CDC severe maternal morbidity indicators was 0.52. See Table 1 for descriptive statistics of the 66 severe maternal morbidity cases following in-depth chart review.
Descriptive Statistics of Sixty-Six Veteran Pregnancies with a Severe Maternal Morbidity Event Based on Data Extracted from Individual Chart Review
Includes American Indian/Native Alaskan, Asian, Pacific Island/Native Hawaiian.
RUCA designation rural/highly rural.
BMI during pregnancy recorded nearest to first pregnancy diagnosis.
Includes adjustment disorder, borderline personality disorder, social anxiety disorder, attention deficit hyperactivity disorder, bipolar disorder
Includes marijuana, opioids, heroin, cocaine.
BMI, body mass index; RUCA, Rural Urban Commuting Area; AMA, Advanced maternal age; PTSD, posttraumatic stress disorder.
The majority of pregnancies affected by severe maternal morbidity events were among women who were younger than 35 (76%), experiencing a first pregnancy (61%), and delivered by cesarean section (59%). The primary, or first time, cesarean section rate was 69%. Mental health problems (59%), obesity (65%), hypertensive disorders (38%), gestational diabetes (17%), rurality (29%), and substance use (26%) were common (Table 1). Forty-four percent of severe maternal morbidity events occurred among Black women although Black women represented only 27% of all pregnancies during the time period studied (Table 2).
Demographics of Pregnancies with Severe Maternal Morbidity Events and All Pregnancies
Nearly half (48%) of all severe maternal morbidity events occurred in the postpartum period following discharge from the hospital. Of these, over half (53%) occurred in the first week postpartum (Table 3).The 66 cases of severe maternal morbidity events occurred in 64 different hospitals. Following discharge from the delivery hospitalization, some women sought care in other hospitals. A total of 14 additional hospitals were involved in postpartum care for these 66 maternal morbidity cases. Cases occurred in 27 different states with half (50%) in the 10 states designated as southern by the United States Census Bureau.
Timing of Severe Maternal Morbidity Events Among Sixty-Six Pregnancies
Among the 66 pregnancies reviewed, 92 severe maternal morbidity events were identified. Sepsis, eclampsia, embolism, massive transfusion, and congestive heart failure/pulmonary edema/cardiomyopathy accounted for the majority of events (Fig. 1).
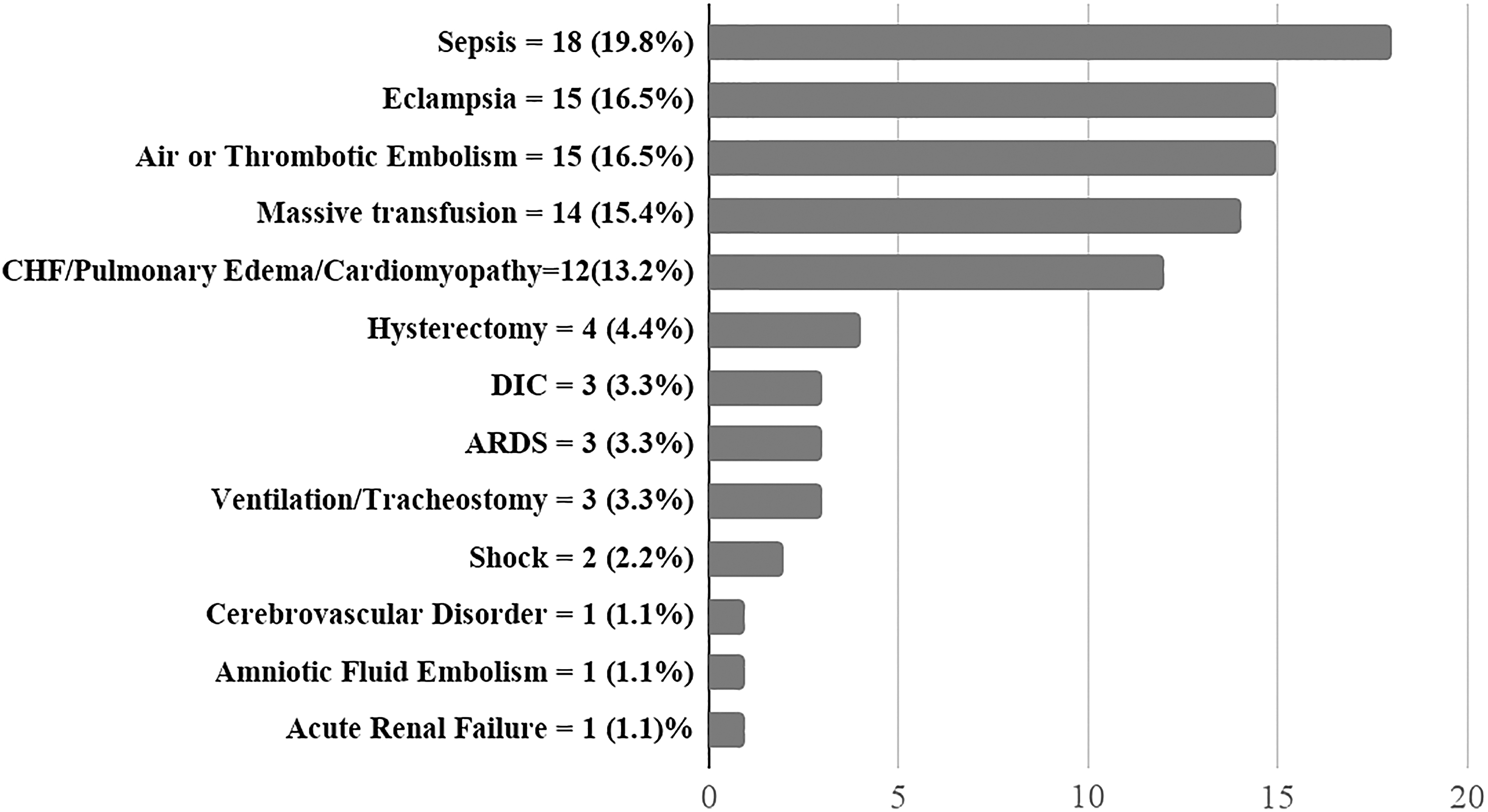
Severe maternal morbidity events among a cohort of 66 Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn women veterans enrolled for care at the Veterans Health Administration January 1, 2014–December 31, 2016 (n = 92 events).
Of note, 14 of the 66 cases involved hemorrhage and transfusion, 9 of which were confirmed positive for massive transfusion with ≥4 U blood products documented in the medical record. The remaining five lacked documentation in the medical record about the exact number of blood products transfused, but other procedures were referenced in subsequent progress notes, including returning to the operating room with use of a bakri balloon and/or uterine artery embolization or coagulopathy due to blood loss.
Discussion
This study investigated severe maternal morbidity events among a cohort of OEF/OIF/OND veterans who were enrolled for care at the VA and experienced a pregnancy between January 1, 2014 and December 31, 2016. Pregnancies were identified using an exhaustive list of pregnancy-related ICD-9/10 codes that included all pregnancy diagnoses regardless of outcome. Severe maternal morbidity events were identified by applying the ICD-9/10 codes used by the CDC to identify 18 severe maternal morbidity indicators. 5 Chart review was then performed for 127 pregnancies that were identified with a severe maternal morbidity code based on a structured guide. Following chart review, 66 cases were classified as confirmed or presumed positive for a severe maternal morbidity event. There were no repeat pregnancies for any individual during the study period and no maternal deaths occurred. The PPV of applied CDC severe maternal morbidity indicators was 0.52, roughly consistent with previous findings that reported a PPV = 0.44 using CDC indicators to identify severe maternal morbidity cases. 28
The VA does not directly provide comprehensive maternity care to women veterans. Instead women are referred to non-VA providers for care, which is paid for by the VA. Nonetheless, this investigation of severe maternal morbidity suggests several ways in which the VA can develop or strengthen services for pregnant and postpartum veterans. Particularly relevant to VA involvement in maternity care is the high rate of mental health problems among women veterans who experienced severe maternal morbidity events. The VA has previously demonstrated significant success in addressing the mental health needs of women veterans. 29
In the current study, 59% of women who experienced a severe maternal morbidity event during pregnancy had at least one mental health diagnosis, while 20% had three or more. The most common diagnoses were depression (39%), anxiety (30%), and posttraumatic stress disorder (29%); however, adjustment disorder, borderline personality, and bipolar disorder were also identified. The high rate of depression confirms the need for consistent evaluation of perinatal suicidality and depression screening, as has been previously recommended, 22 especially since mental health problems have been identified nationally as preventable contributors to severe maternal morbidity and mortality, and an important focus for maternity care improvement initiatives. 16,30,31 The VA is well positioned to develop innovative comanagement strategies that integrate veteran-specific mental health care with maternity care during the childbearing year.
Black women appeared to be differentially affected by severe maternal morbidity events in this cohort, although reasons for higher rates of adverse events among black women were not readily apparent. Forty-four percent of women experiencing severe maternal morbidity events were Black, while only 27% of all pregnancies were among Black women. This finding is consistent with national data. 1,5,8 Likewise, rural women may have been differentially affected. Nearly one-third (29%) of women experiencing severe maternal morbidity lived in rural areas by zip code at the time of event. While it was not possible to obtain individual-level zip code data from all pregnancies for comparison, 22% of all women veterans live in rural or highly rural settings. 18 Further evaluation of risk factors and barriers to care is warranted, especially among these high risk populations.
Other preventable patient level factors, such as lack of awareness of warning signs, medication compliance, and psychosocial factors, were difficult to assess in the current study. The VA maintains a system of Maternity Care Coordinators, usually nurses and social workers, who contact pregnant women through pregnancy and the postpartum period to identify problems, provide education, and connect women to appropriate resources. 32 The Maternity Care Coordination program could support further research into preventable patient-level factors associated with maternal morbidity and mortality. Current veteran uptake of the Maternity Care Coordination program is around 60%. 32 The feasibility and efficacy of expanding the role and reach of Maternity Care Coordinators should be considered, especially in regard to women veterans who experience severe complications during pregnancy.
Provider- and facility-level factors contributing to maternal morbidity were difficult to assess in this study given limitations of the data and the number of institutions involved. Collectively, women veterans receive maternity care at hundreds of non-VA clinics and hospitals across the nation that differ in terms of volume, level of acuity, public/private ownership, and teaching status. The 66 severe maternal morbidity cases evaluated in this study occurred at 64 different hospitals located in 27 different states, with additional care episodes for evaluation of related problems occurring in 14 other hospitals. Obstetric records were requested by each veteran's local VA facility, usually for billing purposes, and then scanned into the electronic health record. This produced a maternity care record that was inconsistently available, frequently lacked supporting information such as laboratory results and prenatal records, and was accessible only through review of archived documents. Practice characteristics, such as criteria for ICU admission, cesarean section rate, and staffing, could not be retrospectively evaluated. Ongoing maternal outcome surveillance among veteran women would be improved by consistent data collection related to facility and provider characteristics.
VA coverage of maternity care costs may reduce access barriers due to uninsurance among veteran women. However, research has shown that women veterans still experience barriers to receiving care at the VA and a relatively high percentage fail to enroll. Washington et al. reported a 44% VA market penetration rate among OEF/OIF/OND women veterans, higher than veteran women from other combat eras, but relatively low utilization overall. 33 Reporting on a survey of 519 women veterans, Mattocks et al. found that nearly one third reporting barriers to receiving prenatal care as early as they desired. 34 Tracking timeliness and comprehensiveness of care, including time from pregnancy diagnosis to first prenatal visit, gestational age at first prenatal visit, and total number of prenatal visits, would provide a more accurate view of potential access barriers. Prenatal records that would contribute to these data were seldom available in pregnancy documentation within the VA electronic health record.
The majority of severe maternal morbidity events occurred during the postpartum period following discharge from the hospital (49%). Among these cases, over half were during the first postpartum week (53%). This is consistent with national reports and confirms the importance of early and frequent postpartum care as needed, as opposed to a single appointment 6 weeks after birth. 35 In 14 cases postpartum evaluations and readmissions occurred at hospitals that were different from the facility where the birth occurred. While it was not possible to determine why these alternative facilities were chosen, geographic proximity, previous connection with a facility, or concern over lack of insurance at non-VA facilities once the pregnancy had ended may have contributed to the decision to seek care elsewhere. These findings highlight the importance of continuity of care during the critical period immediately following delivery and suggest an opportunity for increased outreach and support from the VA as women transition back to VA care following pregnancy.
Future research
Further qualitative research among women veterans who experience severe maternal morbidity would help build the evidence for best practice prevention and support, with special focus on populations at high risk, including African American veterans, those who experience mental health problems and other complications, and women living in rural areas. Coordination of pharmacotherapy between VA care and obstetric care should also be evaluated. Further research is needed to design and test perinatal care interventions that strengthen mental health and obstetric comanagement between the VA and non-VA providers, as well as the efficacy of providing education to women veterans about pregnancy complications and warning signs, such as those associated with hypertension, diabetes, and substance use. Race-based and rural/urban comparative analysis is needed in future investigations with a larger sample to identify predictors of severe maternal morbidity in these populations. Finally, as the population of reproductive-aged women veterans continues to grow, the efficacy of VA-based partial (antepartum and postpartum only) or complete (antepartum, intrapartum, and postpartum) obstetric services should be evaluated in high volume facilities. Continuity of care before, during, and after pregnancy has been associated with improved outcomes among mothers and babies. 4,36,37
Strengths and limitations
This research is limited by the frequent lack of comprehensive obstetric record and data reporting in the VA system. Access to records from non-VA providers varied substantially across facilities. This has several implications for the study. Twenty-three of the 66 cases of severe maternal morbidity identified were classified as presumed positive, rather than confirmed positive, and this may have led to inaccuracies in the data. Furthermore, this lack of consistent, comprehensive record prevented analysis of preventability or appropriateness of medical intervention, especially in terms of cesarean section. Prospective case review based on access to the complete obstetric record would correct this limitation, along with standardized pregnancy documentation in the VA electronic health record. This study was limited by lack of a multidisciplinary review as is typical for morbidity/mortality review committees. The small sample size limited the ability to draw conclusions about statistically significant predictors of severe maternal morbidity.
Conclusions
This study provides an analysis of a severe maternal morbidity surveillance methodology among women veterans whose pregnancy costs were covered by the VA and who received care from non-VA providers. High rates of mental health problems, obesity, rurality, hypertensive disorders, gestational diabetes, and racial discrepancies were noted among women who experienced severe maternal morbidity events. Surveillance at the VA would be improved by standardized reporting of maternal outcomes in the electronic health record. A multidisciplinary review committee within the VA would help refine surveillance systems, identify service coordination issues, and develop problem solving strategies aimed at improving maternity care for women veterans. As the national health care system best qualified to address the unique needs of veterans, the VA is well positioned to develop innovative care models that integrate mental health and obstetric care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Women Veterans Cohort Study (WVCS) is supported by the Department of Veterans Affairs, Veterans Health Administration, Health Services Research and Development Project [IIR 12-118].