
Abstract
Background:
Delay in diagnosis may be a contributing factor to the observed correlation between young age and advanced disease. We examined time to cancer diagnosis in young women presenting to surgeons with breast-related complaints.
Materials and Methods:
This population-based cohort study included all women aged 18–44 presenting to a surgeon with breast-related complaints between 2005 and 2015 in a large health care plan (n = 157,264). Data included demographics, diagnosis codes, and workup. Cancer diagnosis was ascertained from the national cancer registry. Time to breast imaging and biopsy was compared between the different age groups. Logistic regression analysis was used to determine the association between age and delay to biopsy while adjusting for possible confounders.
Results:
During the 1st year after the visit, 45,434 (29%) women had breast imaging; 5,766 (3.7%) women had a breast biopsy; and 676 (0.43%) were diagnosed with breast cancer. Overall, time to first breast imaging and biopsy did not differ significantly between the age groups. But nonspecific visit codes (other than breast mass) were associated with delays to imaging and biopsy. Among, women diagnosed with breast cancer, age under 40 years (odds ratio [OR]: 2.3, 95% confidence interval [CI]: 1.4–3.9), being postpartum (OR: 2.6, 95% CI: 1.1–5.9), and a nonspecific visit code (OR: 8.3, 95% CI: 4.9–14.2) were associated with delay.
Conclusions:
Symptomatic women with lower a-priori likelihood of malignancy (younger age, postpartum, or nonspecific visit code) are at significantly greater risk of delayed diagnosis of cancer. Physicians should be aware of the diagnostic challenge in young women presenting with nonspecific symptoms.
Introduction
Breast cancer in women younger than 40 years of age is not common although it is the leading cause of cancer-related death in young women. 1 Young women are more likely to be diagnosed with more advanced disease, 2 –5 which may be related to more aggressive disease characteristics, lack of screening, or diagnostic delay. Diagnostic delay may be a result of multiple factors, including patient and health care delays. 6 Referral and diagnostic delays can occur because symptoms are attributed to benign causes due to the low incidence of breast cancer and the high prevalence of benign breast lesions in this age group. The low suspicion may be accompanied by inconclusive or negative studies, leading to a slower workup of the patients' complaints.
As screening for breast cancer is not recommended for average risk women younger than the age of 40 years, 7 most women diagnosed with breast cancer younger than the age of 40 years present with breast symptoms, usually a self-discovered breast lump. 8 –10
Studies examining the association between age and delay in diagnosis report conflicting results and are limited by their design, surveying selected women diagnosed with breast cancer in retrospect, and therefore subject to selection and recall bias. 6,8,9 To clarify if there is an association between age and diagnostic delay and the factors that may contribute to such a delay, we examined the diagnostic workup of young women presenting to general surgeons. As screening mammography is recommended in Israel starting at 50, we focused on women younger than the age of 45 years within a large health care plan.
Materials and Methods
Data were obtained from the Maccabi Healthcare Services (MHS), a large sick fund in Israel, with over two million members. The Institute Review Board approved this population-based cohort study examining the time elapsed from the first breast-related visit to a general surgeon to breast imaging and biopsy in women younger than the age of 45 years. Informed consent was waived.
All first visits to a surgeon between 2005 and 2015 by women aged 18–44 years, with a breast-related visit code (Appendix Table A1) were included. We excluded older women to minimize the inclusion of visits of healthy women for screening clinical breast examination. This visit was defined as the index visit. Women were required to be members of the MHS for at least 1 year and with at least 1 year of follow-up.
To limit the visits to those of women presenting with breast symptoms, and exclude visits of women presenting with screening abnormalities, visits of women with a mammogram or ultrasound done within 1 year before the index visit were excluded. Visits with codes describing breast cancer, lymphadenopathy, or high-risk screening were excluded, as were women with known cancer (breast or other). As coding is frequently inaccurate, we included also nonspecific codes such as observation or health check-up.
Data collection
Data collection included: Demographics, including age, marital status, country of birth, district of residence, and socioeconomic level (categorized into quartiles according to the poverty index of the member's enumeration area as defined by the 1995 national census based on several parameters, including household income, educational qualifications, crowding, material conditions, and car ownership.)
11
Data related to the visit (date, diagnosis codes, date of closest delivery) and data on subsequent workup (breast imaging and breast biopsy within 12 months of index visit), and breast cancer diagnosis.
Cancer diagnoses and dates were ascertained through the Maccabi Cancer Registry, which is regularly updated with all cancer cases in MHS members reported to the Israel Cancer Registry (INCR). 12
Delay in diagnosis was defined when more than 90 days passed between the index visit and the diagnosis of breast cancer. We used a 90-day definition for delay based on published research supporting a possible clinical relevance for this time period. 13
For women who were pregnant and the delivery occurred up to half a year before the index visit, the visit was considered a postpartum associated visit. When delivery occurred within 9 months after the index visit, it was considered a pregnancy-associated visit.
Statistical methods
Time to workup was calculated according to age categories, socioeconomic level, district of residence, pregnancy, and postpartum status. Time to first imaging and biopsy was compared between the younger and older groups using the Mann–Whitney test. Categorical variables were compared using the chi-square test.
Multivariable ordinary logistic regression models were created to examine the correlation of age with delay to biopsy separately for women with benign diagnoses and those with cancer diagnoses, while adjusting for potential confounders to determine an odds ratio (OR) as an estimate of the relative risk and the 95% confidence interval (CI). The following covariates were included in the multivariable models as potential confounders: patient demographics (marital status, socioeconomic status, district of residence), index-visit code (mass in breast vs. all other), postpartum-related visit, and pregnancy-associated visit. For the multivariable models, two age groups were formed: young ( younger than the age of 40 years) and old (40–44 years).
Kaplan–Meier survival curves were fit to the data to assess the association between age groups, visit code, and time to diagnosis. All tests were two sided and a p-value of <0.05 was considered significant. All analyses were done using IBM SPSS Statistics for Windows, Version 25.0 (Armonk, NY).
Results
During the study period, a total of 157,264 eligible women were identified and divided into four age groups (younger than 30 years of age, 30–34, 35–39, and 40–44). At the time of the index visit, half of the women were married (78,245), 5,566 (3.5%) were pregnant, and 15,274 (9.7%) were postpartum. Table 1 summarizes the distribution of patients among various categories, the associated times to breast studies and rates of cancer diagnoses within 1 year of the index visit.
Breast Studies and Diagnosis of Cancer Within 1 Year from Index Visit
See text for details.
SE, standard error; US, ultrasound.
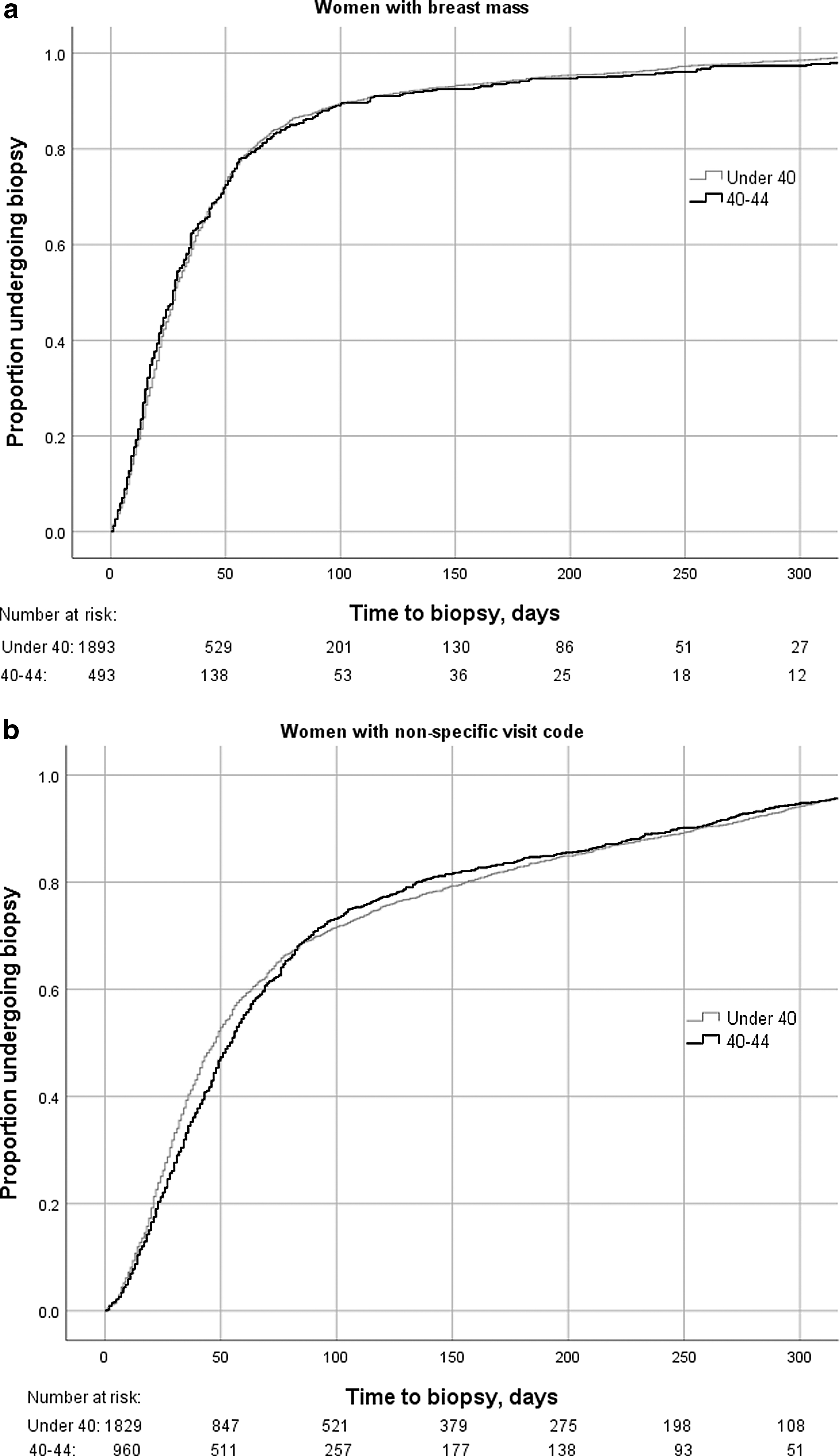
Within 1 year of the index visit, 45,434 (29%) women had at least one breast imaging done, 5,766 (3.7%) had a breast biopsy, and 676 (0.43%) women were diagnosed with breast cancer (invasive or in situ). The proportions of women undergoing breast imaging increased with age. In the group of women who had an imaging study, the proportion of women undergoing a biopsy decreased with age (18% in women younger than 30 years; 12% in women 30–34; 11% in women 35–39; and 10% in women 40–44 years old, p < 0.0001). Breast cancer diagnoses per visit increased from 0.1% in the youngest age group to 0.8% in the oldest age group (40–44). Time to first imaging and to first biopsy did not differ significantly between the different age groups. Figure 1 compares cumulative time to first biopsy between women younger than 40 years and the older group (40–44 years, log rank p = 0.051).

Cumulative time from index visit to biopsy (p = 0.051).
To identify predictors of diagnostic delay, the cohort was divided according to the visit diagnosis code into two groups, those with a diagnostic code describing a breast mass (n = 12,483; 7.9%) and those with all other visit codes (Table 1). Most (n = 10,145; 81%) of the women with a breast mass visit code underwent at least one breast imaging study within 1 year of the index visit (compared to 24% (n = 35,289) of the women with all other codes). Over a fifth (n = 2,763; 22%) of the women with a visit code describing a breast mass had a biopsy within a year of the visit, compared to 2% (n = 3,003) of the women with all other codes (p < 0.0001). Mean time to first imaging and biopsy differed significantly between the two diagnosis groups (Table 1); women with a nonspecific visit code had longer mean times to first imaging and biopsy regardless of their age (Table 2).
Mean Time to First Imaging and Biopsy Based on Age Group, Visit Diagnosis Code, and Biopsy Result
For the difference between the two age groups.
Chi square test.
Mann–Whitney test.
Most (n = 35,289; 78%) of the women undergoing a breast imaging study within 1 year of the index visit had a nonspecific visit code. In the group of women undergoing a biopsy within 1 year of the index visit, 3,003 (52%) had a nonspecific visit code.
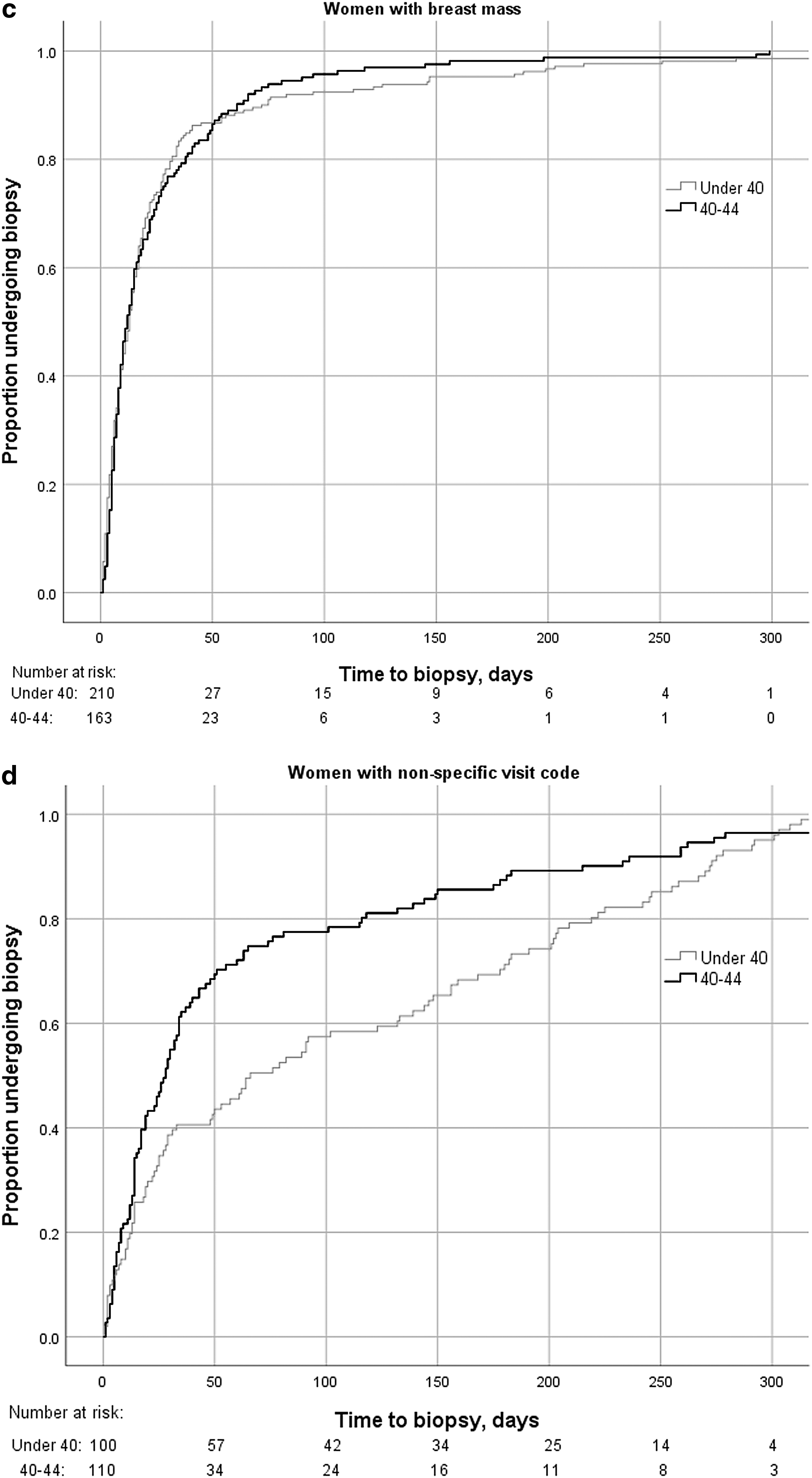
The cohort of women undergoing a biopsy within 1 year was further divided based on the results of the biopsy (benign vs. malignant). Of the 676 women diagnosed with cancer within 1 year of the index visit, 248 (37%) had a nonspecific visit code. Table 2 summarizes mean times to first imaging and biopsy based on visit diagnosis code, age group, and final biopsy result. Cumulative incidence curves of time to biopsy in the different diagnosis groups are shown in Figure 2a–d. Women younger than the age of 40 years with a nonspecific visit code had the longest times to biopsy, especially when the final diagnosis was cancer.
Two separate multivariable regression models were fit to assess predictors of delay to biopsy based on the final diagnosis. A nonspecific visit code was associated with delay to biopsy in all women. Age was not associated with delay to biopsy in women with a final benign diagnosis. In women ultimately diagnosed with cancer, age <40, a nonspecific visit code and being postpartum at the index visit were all predictors of delay to diagnosis (Table 3).
Multivariable Analysis of Risk Factors for Diagnostic Delay (Defined as More Than 90 Days Between Index Visit and Biopsy), by Outcome (Benign or Malignant)
CI, confidence interval; NA, not available; OR, odds ratio.
Discussion
The results of this population-based study of young adult females indicate that while time gaps from initial surgeon visit to breast imaging and biopsy are reasonable, clinically important delays were recorded among subgroups. These subgroups include women with a visit code other than breast mass, and in the group of women ultimately diagnosed with breast cancer, being postpartum or younger than the age of 40 years.
Our results are in line with previous studies on the association between age and delay in diagnosis of breast cancer. In a multicenter cohort study women aged 40 years and younger with breast cancer were interviewed regarding their presentation and diagnosis. 7 Delay was defined as 90 days between seeking medical care and receiving a diagnosis of cancer. Of 585 participants, 80% presented with self-detected abnormalities. Median time to seeking medical care in this study was 14 days. The median time between seeking medical attention and diagnosis was 16.5 days, with 12% recalling care delays. Pregnancy was not associated with delay. Although there was a group of women who suffered from self-delay and or care delay, the authors concluded that most young women do not experience long delays to diagnosis. The study population was mostly white, college educated, and health insured, limiting the generalizability of this study. 7
In a report from the National Comprehensive Cancer Center Network (NCCN) Breast Cancer Outcomes Database Project, age was assessed as a risk factor for delay in diagnosis. 6 This study surveyed women with breast cancer within weeks to months of their diagnosis; delay in diagnosis was defined when time from initial sign or symptom to diagnosis was more than 60 days. Of 2,445 women aged 40 years and younger, 90% presented with symptoms. Younger women were more likely to have a delay in diagnosis. Thirty five percent (vs. 25% in the older group) had a delay of more than 60 days, and 13% experienced a delay of over 180 days. On multivariable analysis, symptomatic presentation was associated with delay in diagnosis and advanced stage at diagnosis, which was independent of age at diagnosis. 6
Delay in diagnosis of six different cancers was assessed using mailed questionnaires in a study from the National Health System in England. 9 Patients with breast cancer had the lowest mean delays (8 weeks). Delays were mainly due to patient and primary care delays.
Since patients in MHS do not need a referral from a general practitioner to make an appointment with a surgeon, many women with breast symptoms will first present to a surgeon. It is difficult to estimate the proportion of women who present to a surgeon with a breast-associated symptom other than a mass who ultimately are diagnosed with breast cancer, since we cannot confirm that all these visits were due to a breast symptom. However, almost a quarter of this group had a breast imaging study done within 1 year of the index visit (n = 35,289; 24%). In the group referred to breast imaging 0.6% of the women younger than 40 years and 0.9% of the 40–44 age group were diagnosed with breast cancer (compared to 3.3% and 6.6% of the women presenting with a breast mass).
A substantial proportion (n = 248; 37%) of the women who were ultimately diagnosed with cancer were coded with a nonspecific diagnosis (33% of the women younger than 40 years of age and 41% of the older group).
To assess generalizability and potential selection bias, we assessed the proportion of all breast cancer cases in MHS during the study period that were included in our data. Based on the most recent INCR data, 12 during the study years, the median number of new breast cancer cases every year in women younger than 45 years of age was 581 (standard deviation 45.4). The expected number of new breast cancer cases (invasive and in situ) in this age group over 11 years in MHS is 1,597 in total (25% of total). We estimate that our data capture almost half of the women in the health care plan diagnosed with breast cancer during these years, as during the study period 676 women were diagnosed with breast cancer within 1 year. Another 71 women diagnosed with breast cancer were excluded because imaging was done before the index visit.
This study was designed to examine the workup of young women presenting to a surgeon with breast symptoms. But it is limited by several factors. As coding is limited in its accuracy, we are unable to confirm what proportion of the cases presented was in fact due to breast symptoms. We chose to include general codes (i.e., observation) to include all types of visits, with the assumption that nonspecific visit codes may be associated with low clinical suspicion. Since we are not able to confirm the association between the cancer diagnosis and the index-visit, we chose an arbitrary cutoff of 12 months for time elapsed from index visit to breast imaging and biopsy. These cutoff points may include cases not associated with the index visit or miss cases in which the delay was longer.
We captured almost half of the incident cancers, suggesting that there are different diagnostic pathways (primary care physician, gynecologist, or private medical services). We are unable to assess other reasons for delay, specifically patient delays. Pregnancy was ascertained through delivery dates, limiting our ability to capture all pregnancies, including those that did not end in a live newborn.
This is a large cohort study capturing all first visits of young women with breast complaints to a surgeon, enabling us to examine prospectively the workup of these women, and therefore not subject to recall bias. This is the first study to examine delays in diagnosis of breast cancer in young women using a very large cohort of women, enabling us to focus on the difficulty of the health care system in evaluating young women with breast symptoms. These difficulties arise from the low incidence of cancer in these women on the one hand and the high proportion of women presenting with nonspecific symptoms on the other hand. A large proportion of women younger than 40 years of age diagnosed with breast cancer present with nonspecific breast symptoms. These women will suffer from delays in referral and scheduling of studies, probably due to low suspicion.
Overall, these findings suggest that the diagnosis of breast cancer in young women is challenging even for experienced surgeons.
Conclusion
In this large population-based study examining delays to cancer diagnosis in women younger than 45 years of age presenting to surgeons, we found that there were higher proportions of delay to biopsy (over 90 days) in women with a nonspecific visit code (vs. breast mass). In women with a diagnosis of breast cancer within 1 year of the index visit, age younger than 40 years, being postpartum, and a nonspecific visit code were all associated with higher ORs for diagnostic delay. Physicians should be aware that a significant proportion of women younger than 40 years of age with breast cancer might present with nonspecific breast symptoms. In these women, the diagnosis of breast cancer can be challenging.
Ethical Approval
The study was performed in accordance with the Declaration of Helsinki.
Footnotes
Authors' Contributions
T.S.M. designed the study, performed data analyses and interpretation, and wrote the article. T.S. and G.H. designed the study, obtained the data, and contributed to data analyses, interpretation, and writing the article. G.H. supervised the study.
Author Disclosure Statement
T.S.M. and G.C. have no conflict of interest to declare. T.S. received remuneration from Roche.
Funding Information
No funding was received for this article.
Appendix
List of Visit Codes
| Code | Code description | n |
|---|---|---|
| V67.5 | Follow-up | 136 |
| V67.9 | Follow-up | 2,811 |
| V71 | Observation and evaluation for suspected condition | 215 |
| Y15638 | Observation | 16,085 |
| Y20385 | Observation | 34,092 |
| V70.0 | Routine general medical examination | 337 |
| Y22644 | Health check-up | 11,256 |
| Y20352 | Screening of unspecified condition | 3,053 |
| V71.9 | Observation for unspecified condition | 2 |
| Y23556 | Consultation | 19 |
| Y21406 | Breast examination | 54,661 |
| V76.1 | Screening of the breast | 3,182 |
| 611.71 | Mastodynia | 9,567 |
| Y20670 | Unspecified breast disorder | 770 |
| 611.9 | Unspecified breast disorder | 5,241 |
| 611.2 | Fissure of nipple | 29 |
| Y20661 | Signs and symptoms of breast | 25 |
| Y18682 | Swelling mass/lump in chest | 25 |
| Y20662 | Other signs/symptoms of breast/nipple/induration | 8 |
| Y15683 | Subinvoltion of breast duct | 12 |
| 611.72 | Lump/mass breast | 15,880 |
| Y22539 | Breast biopsy | 17 |
| 85.11 | Percutaneous breast biopsy | 14 |
| 85.91 | Aspiration of breast | 65 |
| Y15654 | Mastitis | 796 |
| 610.9 | Benign mammary dysplasia | 3,065 |
| Y15647 | Mastitis periductal | 12 |
| Y15640 | Cystic breast | 7,438 |
| Y15637 | Fibrocystic changes | 8 |
| Y15639 | Fibrocystic changes | 8 |
| 610 | Breast cyst | 4 |
| Y15653 | Mastitis | 867 |
| Y15641 | Chronic, cystic, diffuse, periodic segmental | 2,323 |
| Y15652 | Mastitis | 371 |
| Y15646 | Fibrosclerosis of breast | 171 |
| 217.9 | Neoplasm breast female benign | 48 |
| Y21135 | Neoplasm breast female benign | 3 |
| Y20672 | Neoplasm breast female benign | 1 |
| Y21134 | Neoplasm breast female benign | 1,092 |
| Y11419 | Neplasm of uncertain behavior | 17 |
| Y16231 | Galactorrhea | 239 |
| Y16232 | Galactorrhea | 147 |
| Y16226 | Engorgment of breast associated w/childbirth | 261 |
| 676.9 | Galactorrhea | 164 |
| Y16224 | Associated with child birth | 51 |
| 611.5 | Galactocele | 41 |
| Y15681 | Nipple | 25 |
| Y15682 | Nipple | 21 |
| Y15680 | Nipple | 9 |
| Y18168 | Breast | 7 |
| Y16225 | Nipple | 5 |
| Y23481 | Breast | 148 |
| Y15665 | Breast | 5 |
| Y15679 | Nipple | 1,199 |