
Abstract
Background:
Racial and ethnic minority women in the United States have an elevated risk of depression or depressive symptoms compared with White women. There is evidence to suggest that these women are more likely to report somatic symptoms. The objective of this systematic review was to determine whether there are racial and ethnic differences in somatization in women with depression or depressive symptoms.
Materials and Methods:
The study focused on peer-reviewed, English-written publications of adult women that compared two or more racial or ethnic women and used reliable measures. Quantitative studies conducted in the United States were considered. Articles were reviewed from March 2017 to April 2019, with no publication start date.
Results:
Seven studies met the inclusion criteria. Results suggest that African American women were more likely to endorse somatic symptoms compared with White women and, in one instance Hispanic/Latinas. Three of four studies found that Hispanic/Latinas were significantly more likely to endorse somatic symptoms compared with White women; one study found that White women were significantly more likely to report somatic symptoms than Hispanic women. Another study found that White women endorsed significantly higher somatic symptoms than Chinese American women. One study did not find significant differences.
Conclusions:
A pattern emerged with African American and Hispanic/Latina women with depression or depressive symptoms more likely to report somatic symptoms compared with White women. However, it is not clear whether differences were a function of culturally acceptable presentation of symptoms or if the stress of being depressed increased somatization in minority women. Future studies should assess how depression/depressive symptoms affect racial and ethnic minority women to identify mechanisms involved in increased somatization.
Introduction
Somatic symptoms are an important component of depression and can be explained as the clinical expression of psychological and emotional problems with physical symptoms, 1,2 including general aches and pains, decreased energy, and feelings of heavy limbs. 3 Although depression is usually diagnosed by the presence of psychological symptoms (e.g., low mood, low self-esteem, guilt, lack of concentration, sensitivity to criticism, and suicidal ideation), ∼66% of patients with depression in primary care present with somatic symptoms that are difficult to diagnose and treat. 4,5
Somatic symptoms are important because they can improve our understanding of depression, particularly in women who are at higher risk of somatization. Studies have shown that women who present with a higher number of physical symptoms, such as pain, fatigue, and bodily aches, are more likely to be diagnosed with depression than those with fewer physical symptoms. 6 Therefore, it is important to consider the presence and number of physical symptoms in depressed women.
Somatic symptoms are especially relevant in women because they have been shown to be more likely to report somatic symptoms than men 7 –9 and experience depression at a higher rate on average than men (5.5% in women and 3.2% in men) in the United States. 10 Although depression disparities by gender might be explained by evidence that suggests women experience symptoms differently than men, 11 less is known about differences in the somatization across women from different racial and ethnic backgrounds. This study aims to address the lack of clarity in the literature with a systematic review of the empirical U.S. literature on somatization, race, and ethnicity in depressed women.
Several studies have identified racial and ethnic differences in the diagnosis and treatment of depression in adult women in the United States. 12,13 The prevalence of depression in the United States among adult Black women is highest at 11%, whereas Asian women have the lowest rate at 3.9%, and both White and Hispanic women have a 10.5% rate. 14 Studies have also reported racial disparities in the prevalence of maternal depression, with Black mothers reporting higher depression rates compared with their Hispanic or White counterparts. 15 –17 Racial and ethnic disparities in depression might be explained by socioeconomic status (SES) factors like income, education, and employment status. 18 For instance, low-income and low-education mothers have an increased risk of developing depression than their counterparts. 18
Screening for and diagnosing depression in women from diverse cultures can be complicated by the fact that depression might present differently in women according to culture and implicit acceptability of specific symptoms. 19,20 A recent systematic review identified cultural differences in the prevalence of depressive symptoms with the lowest rates in Asia and the highest rates in Latin America, the Caribbean, and Anglophone countries. 21 Somatization is a common sign of depression in Hispanic, Asian, and African cultures, whereas feelings of sadness and guilt are more characteristic signs of depression in Western cultures. 22,23
Researchers have also reported that there are racial and ethnic differences in the presentation of somatic symptoms with some ethnic groups endorsing somatic symptoms more than the others. 4,24 Racial discrimination can be associated with these racial differences in somatic symptoms and has been found to be associated with depression in women; Black women in the United States who reported experience of racial discrimination had higher depressive symptoms than White women. 25 In addition, in a study of matched African American and White depressed patients, African Americans were more likely to report somatic symptoms than Whites with similar demographic characteristics. 26 Furthermore, the effect of discrimination is higher in those who have low education levels or low SES. 27 For example, older African Americans were more likely to report symptoms such as fatigue, back pain, and headaches compared with elderly White Americans. 4,28
Although some researchers have reported racial differences in the presentation of somatic symptoms, there is no consensus as race and low SES are usually conflated or co-vary. For instance, mothers of low SES report more somatic symptoms than their more affluent counterparts. 18 Immigration can also be a predictive factor of somatic symptoms. U.S.-born Latinos were significantly more likely than Latino immigrants to have psychiatric disorders, and the investigators suggested that acculturation may contribute to psychiatric morbidity. 29 Still, this issue remains unclear as does the role of race and ethnicity on somatization in depression among women in the United States.
Thus, the objective of this systematic review was to determine whether racial and ethnic minority women (e.g., Asian/Asian American, Black/African American, and Hispanic/Latina) with depression or depressive symptoms are more likely to report somatic symptoms compared to White, non-Hispanic women in the United States with depression or depressive symptoms. A focus on the United States is necessary given the racial and ethnic disparities in the diagnosis and treatment of depression among women. 19 Determining whether there are differences by race and ethnicity will inform the evaluation and diagnosis of depression in women in the United States, where racial and ethnic diversity is high.
Materials and Methods
The selection process for this systematic review followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 30 The search was performed by two of the three authors [TA and JW] to ensure a comprehensive review of the literature. The search was conducted between March 2017 and April 2019, with no restrictions on publication dates. The electronic search was conducted using the following databases: PubMed, CINAHL, PsycINFO, PsycARTICLES, Academic Search Premier (EBSCO), Social Services Abstracts, and Scopus. The keywords and search terms were combined using a Boolean search method and included depression, mental illness, depressive symptoms, somatic symptoms, somatization, racial differences, ethnicity, race, women, culture, cultural, non-Hispanic White, Caucasian, Black, African American, Asian, Asian American, Latina, and Hispanic. Manual searches of the reference list of articles selected for full-text review were also conducted.
Selection criteria
The literature search was conducted based on the following eligibility criteria, publications should be peer-reviewed, published in English, contain a sample consisting of adult women 18 years and older, use reliable and validated measures of depression or depressive symptoms, assess somatic symptoms, be conducted in the United States, and used a study design (i.e., cross-sectional, longitudinal, observational, or controlled trial) that compared two or more racial or ethnic women (e.g., Hispanic vs. African American, Asian immigrants vs. native-born Asians, etc.). Although this systematic review focused on women, publications with samples including men were not excluded from the study. However, results had to be reported with race, ethnicity, and gender to be included. Duplicate publications were excluded. Discrepancies between the two researchers on eligibility for inclusion were resolved through discussion and consultation with the lead author [SL-C] until a consensus was reached.
Screening process and data extraction
Studies were selected for inclusion in this systematic review through a series of steps. First, the titles and abstracts were screened. Selected abstracts were saved for an eligibility review in a spreadsheet and were independently screened by the authors [TA and JW] to determine whether each abstract met the eligibility criteria. Reviewers then independently examined the full text to assess final eligibility of inclusion. Discrepancies at each step were discussed until a consensus was reached. Figure 1 shows the number of articles initially identified, screened, excluded, and included in the systematic review according the criteria set. The following data were extracted from each study: (1) objective, (2) sample description, (3) recruitment site/strategy, (4) independent variables and outcome measures, and (5) outcomes/results.
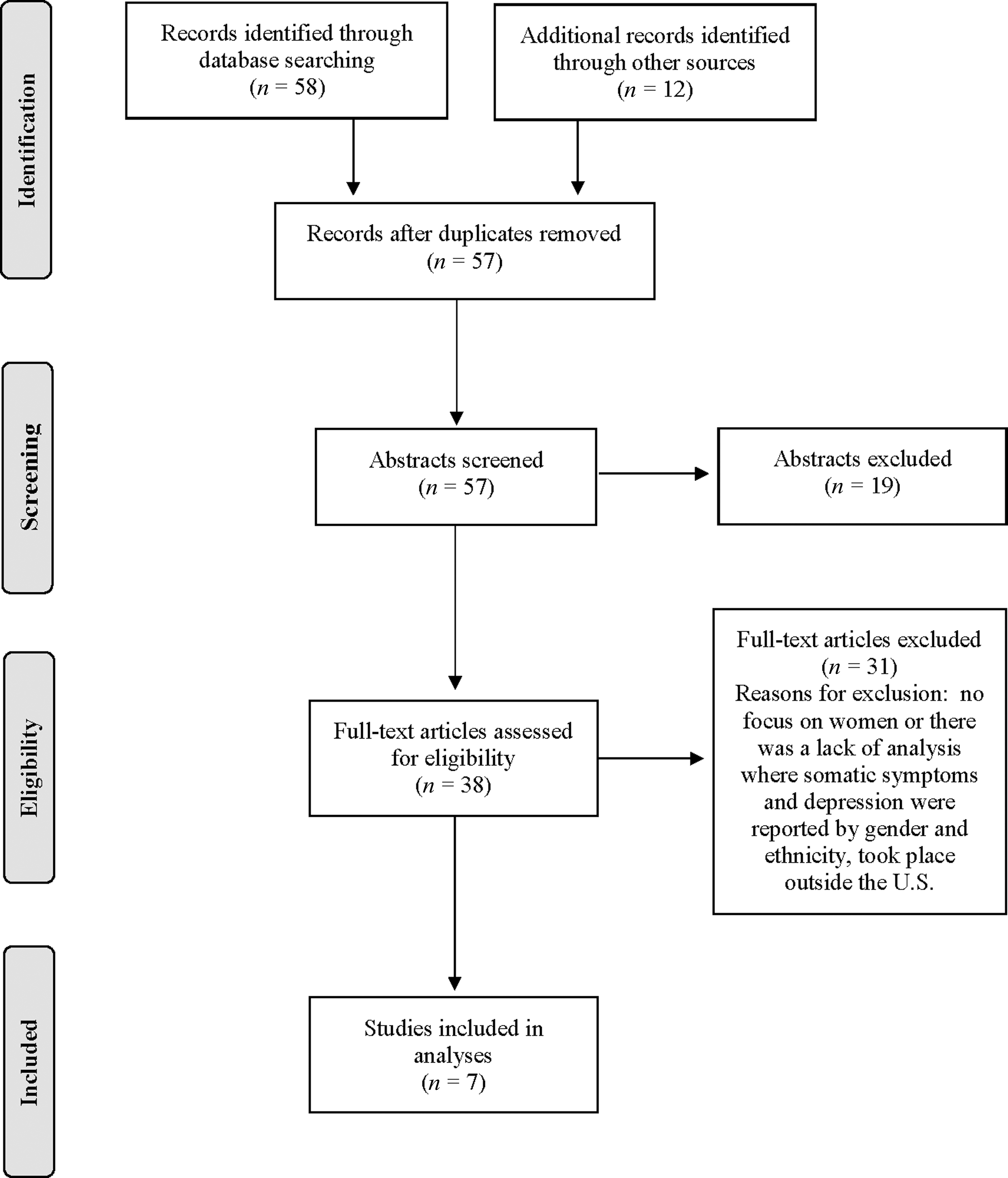
PRISMA flow diagram showing the number of articles identified, screened, excluded, and included in the final review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality appraisal and risk of bias
The studies selected for full-text review were then appraised for quality using the 10 questions from the Critical Appraisal Skills Programme (CASP). 31 The study type (e.g., systematic review, cohort study, and qualitative study) was determined and appropriate evaluation questions were used to assess the quality of each study. Using these questions, a quality rating of “Good,” “Fair,” or “Poor” was assigned to each study based on the guidelines provided by the U.S. Preventative Services Task Force Quality Rating Criteria. 32 A “Good” designation indicated that a study met all the criteria: reliable and valid measures that were applied equally to groups, follow-up of at least 80%, consideration of “all important outcomes,” and appropriate consideration of confounds. A designation of “Fair” indicated that a study presented with any of the following issues: comparable groups but differences in follow-up existed, acceptable measures, and not “all important outcomes” and potential confounders were considered. Finally, a study was designated as “Poor” if any of the following limitations were present: incomparable groups, invalid or unreliable measures, and important confounds were not considered. The studies selected were evaluated for the risk of bias using the following criteria: (1) sample selection, (2) inclusion criteria, (3) exclusion criteria, (4) validity of measures, (5) reporting bias, (6) rate of attrition, (7) if the study included an intervention, the effect of outcomes, and (8) the generalizability of results. Both the quality appraisal and risk of bias were evaluated independently by two authors [TA and JW] and reported in Table 1. The quality and bias tables were discussed between the two reviewers and the lead author [SL-C] until an agreement was reached for each study.
Study Characteristics, Summary of Results and Quality Ratings
BDI, Beck Depression Inventory; CES-D, Center for Epidemiological Studies—Depression; DIS, Diagnostic Interview Schedule; PHQ-15, Patient Health Questionnaire-15; PRIME-MD, Primary Care Evaluation of Mental Disorders; SD, standard deviation; WIC, Women, Infants and Children.
Results
Study selection
The search yielded 57 records after removing duplicates (Fig. 1). Of those, 19 abstracts were excluded because they did not meet the screening criteria. Of the 38 abstracts selected for full-text review, 31 were excluded because they did not meet the inclusion criteria (e.g., no focus on women and no analysis of somatic and depressive symptoms by gender) resulting in a final sample of 7 studies to review.
Study characteristics
Of the 7 studies selected, sample sizes ranged from 125 to 13,753. Two studies used secondary data. 33,34 All studies used a cross-sectional research design. With the exception of one study, 33 all studies recruited women within mainland United States. Participants ranged from 18 to 65 years of age. Six of the studies included Hispanic/Latinas (e.g., Puerto Rican and Mexican origin) and Whites; all but two studies 33,35 included African American/Black women. Asian or Asian Americans, 34,35 immigrant Blacks, 36 and American Indians or Alaskan Natives 34 were also included. Participants were recruited from community programs (e.g., “Women, Infants and Children” [WIC]), 36,37 outpatient psychiatric clinics, 38,39 communities, 33 university campuses, 35 and samples drawn from nationally representative studies. 34 Although all the studies included women as stipulated by the inclusion criteria, four studies that included men reported results by gender. 33 –35,39
Study quality
Quality ratings for each study included in the review are given in Table 1. Five studies were rated as good 33 –35,37,38 and two as fair 36,39 ; none were rated as poor. Studies rated as fair lacked generalizability, adequate information on informed consent, and assumptions concerning the sample (e.g., physical symptoms not of concern because of age of the sample).
Measures used across studies
Depression/depressive symptoms
As given in Table 1, two of the seven studies used the same instrument to assess depressive symptoms. Myers et al. 38 used the Beck Depression Inventory (BDI) to capture depressive symptoms, and Liefland et al. 39 used the second edition of the BDI. 40 Myers et al. 38 also used the Hamilton Rating Scale for Depression 41 to assess severity of self-reported symptoms and the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) 42 to verify participants' major depression status. Escobar et al. 33 used the Diagnostic Interview Schedule (DIS), 43 an interview schedule based on the DSM-III criteria 44 by the National Institute of Mental Health and was designed to enable lay interviewers and clinicians to make psychiatric diagnoses. Nadeem et al. 36 used the Primary Care Evaluation of Mental Disorders also known as the PRIME-MD to identify women who were depressed. 45 Kalibatseva and Leong 35 and O'Neil et al. 37 relied on the Center for Epidemiological Studies—Depression (CES-D), self-report measure designed to capture depressive symptomatology in the general population. 46 Uebelacker et al. 34 used the Alcohol Use Disorders and Associated Disabilities Interview Schedule 47 to determine DSM-IV major depressive disorder in their sample.
Somatic symptoms
As with the depression measures, various instruments were used to assess somatic symptoms across the seven studies. Escobar et al. 33 and Nadeem et al. 36 used the Somatic Symptoms Index (SSI), a shortened somatization instrument derived from Diagnostic Interview Schedule developed by Escobar et al. 33 Myers et al. 38 used the Brief Symptom Inventory, 48 a self-report scale of psychological distress, including somatization. Uebelacker et al. 34 captured somatic symptoms using the DSM-IV. O'Neil et al. 37 implemented the somatic domain from the CES-D. Liefland et al. 39 used the somatic-affective symptoms from the BDI-II, including appetite and sleep. Kalibatseva and Leong 35 used the Patient Health Questionnaire-15 (PHQ-15), a self-report measure that assesses severity of 15 somatic symptoms. 49 Specific somatic symptoms included in each study are given in Table 1.
Racial and ethnic differences in somatization
Five studies found racial and ethnic differences 33,34,37 –39 ; however, Whites did not always endorse lower somatic symptoms compared with racial and ethnic minorities. Three of the five studies also found differences between minorities. 33,37,39
Uebelacker et al. 34 conducted a secondary data analysis of 13,753 racially and ethnically diverse adults who had a lifetime history of depression or anhedonia and completed the DSM-IV symptoms of major depression. These researchers found that Hispanic and African American men and women were significantly more likely to report appetite/weight changes than Whites (p < 0.05) with similar levels of depression severity as measured on a scale from −3 to 3. Although Uebelacker et al. 34 included Hispanics, Asians, and American Indian/Alaskan Natives, only African American and White women were compared because they had different proportions of women in those groups. This analysis enabled the investigators to determine whether the number of women in those groups accounted for the observed racial differences. Results indicated that when depression severity was equivalent, African American women were significantly more likely to endorse more psychomotor symptoms than White women (p < 0.05). No significant differences in fatigue, sleep disturbances, or appetite/weight changes were observed between African American and non-Hispanic White women. In addition, no significant differences in any somatic symptoms were observed between Asians and non-Hispanic Whites and American/Indian/Alaska Natives and Whites.
When conducting pairwise comparisons, Myers et al. 38 found that in a sample of 125 clinically depressed women, African Americans (p = 0.02) and Latinas (p = 0.05) reported significantly more somatic symptoms than Whites/Caucasians. In a racially and ethnically diverse sample of adult community members seeking mental health services, Leifland et al. 39 found that Latinos endorsed significantly more somatic/affective symptoms than White and African American participants (F = 8.96, p < 0.001). These researchers also found that except for Black women, Latinas reported higher somatic/affective symptoms than all others, including White women (F = 8.03, p < 0.001).
In a study of 607 racially and ethnically diverse low-income mothers, using one-way analysis of variance, O'Neil et al. 37 found significant group differences in somatic symptoms by race and ethnicity (F = 7.01, p < 0.01). A comparison of mean somatic symptoms indicated that African American women (mean [M] = 10.49, standard deviation [SD] = 9.36) reported significantly higher mean levels compared European American (M = 9.36, SD = 5.43) and Hispanic (M = 7.80, SD = 5.74) women. As these mean values show, O'Neil et al. 37 also found that Hispanic women had significantly lower mean somatic scores compared with European American women (p < 0.05).
Escobar et al. 33 conducted comparisons of Latinos and Whites, and also explored differences between Latino subgroups (e.g., Puerto Ricans and U.S.- and foreign-born Mexicans). These researchers found that Puerto Ricans reported significantly higher somatic symptoms compared with Mexican-descent (U.S.- and foreign-born Mexicans) and non-Hispanic Whites (p < 0.001); Mexican-descent individuals had higher somatic symptoms than non-Hispanic Whites (p < 0.001). This difference persisted even after repeating the analysis to account for potential differences in editing processes of somatic symptoms by site (e.g., Puerto Rico had more stringent procedures compared with other sites; p < 0.001). A comparison of women 40 years and older reflected the group-level findings, with Puerto Rican women reporting the highest number of somatic symptoms, followed by Mexican-descent women; non-Hispanic White women reported the lowest number of symptoms. Escobar et al. observed a similar pattern in women 40 years and older diagnosed with major depression/dysthymic disorder, with 58% of Puerto Rican women meeting the criteria for somatization compared with 48% Mexican-descent and 19% non-Hispanic White women.
Kalibatseva and Leong 35 found that in a sample of 519 college students, European American women reported higher somatic symptoms than Chinese American women (p < 0.01) on the somatic items in the CES-D and the PHQ-15. In contrast to the other studies reviewed, although Nadeem et al. 36 found differences in the proportion of women who reported somatization (immigrant Blacks = 75.5%, U.S. Whites = 69.6%, immigrant Latinas = 68.9%, U.S.-born Latinas = 64.3%, and U.S. Blacks = 64.3%), racial and ethnic minorities differences were not observed.
Discussion
The objective of this study was to determine whether racial and ethnic minority women (e.g., Asian/Asian American, Black/African American, and Hispanic/Latina) with depression or depressive symptoms were more likely to report somatic symptoms compared with White, non-Hispanic women in the United States with depression or depressive symptoms. Seven studies met the criteria for full-text review. Samples were recruited from a range of settings, including mental health clinics, community programs, and national samples. The selected studies assessed various somatic symptoms, such as fatigue, appetite, and weight disturbances, and musculoskeletal pain, indicating that differences in somatization are not limited to specific symptoms. All the selected studies compared racial and ethnic minority women with White, non-Hispanic women, three compared Hispanic/Latinas with African Americans, 37 –39 and one compared subgroups of Hispanic/Latinas. 33
Although racial and ethnic disparities in somatization were observed, minority women did not always report more symptoms than White women, 35,37 and disparities were not always observed across all somatic symptoms under investigation. 34 Still, one clear pattern emerged, African American women tended to be more likely to endorse somatic symptoms compared with White women and, in one instance Hispanic/Latinas. Furthermore, except for one study, 37 three of the four studies that compared Hispanic/Latina and White women found that Hispanic/Latinas were significantly more likely to endorse somatic symptoms. 33,38,39
Racial and ethnic disparities observed in the studies reviewed might be explained by some evidence that suggests it is more culturally acceptable for racial and ethnic minorities to present depressive symptoms as physical manifestations because they are less stigmatized and serve as gateway symptoms to seeking medical care. 50,51 An alternative explanation might be that depression is evaluated as a stressor that consequently increases the physical symptoms in an already burdened group of women. It is well established that African American and Hispanic/Latina women in the United States encounter higher levels of explicit and implicit discrimination and other psychosocial stress compared with White women. 52,53
There is also evidence to suggest that lifetime or cumulative stress increases risk of depression 54,55 and takes a toll on the individual's ability to respond physically to additional stress. 56,57 Given the physical demands depression places on individuals, it is arguably plausible that women of color with depressive symptoms experience this added stress at a physical level. However, this is a speculation that should be tested empirically by asking a diverse sample of women how depression affects their lives and how they perceive depression. Indeed, results from a systematic review of 65 studies found that patients with depression attributed their depressive symptoms to one or more factors, but most believed external factors, such as life events and stress, caused their illness. 58 By assessing the meaning racial and ethnic minority women give to feeling or being depressed, we can better understand how they evaluate and report symptoms to allow for better diagnosis, treatment, and education.
Determining if and how contextual factors (e.g., discrimination) and culturally acceptable endorsement of symptoms is especially important among racial and ethnic minorities given the studies reviewed here also revealed significant differences between racial and ethnic minorities. O'Neil et al. 37 found that in a sample of low-income women, African American women reported higher mean somatic symptoms compared with Hispanic/Latina and White women. Escobar et al. 33 found a significant difference in somatization between Puerto Rican women living on the island and Mexican American women living in the United States, even when accounting for the depression diagnosis. These results held up even after controlling for level of education, which often serves as a proxy for SES. Early studies of Puerto Rican women living in the mainland suggest that traditional gender role affiliation is associated with higher somatization compared with Puerto Rican women living in the United States. Escobar et al. 33 also found that higher levels of education and acculturation among Puerto Rican women in the United States was associated with less somatization of depressive symptoms, suggesting that somatization might be learned or associated with assertiveness. 59,60
If education and assertiveness are associated with disparities in somatization, then providing education about depression that helps empower racial and ethnic minority women might help decrease differences observed in this systematic review. However, this hypothesis should be tested with a diverse sample of women who are matched on key demographic characteristics, such as education and SES, who are randomized to a depression education arm, treatment as usual, and passive education arm (e.g., brochure) to determine if education and confidence in depressive symptomatology decreases reports of somatic symptoms and disparities in somatization by race and ethnicity.
One attempt at comparing women with similar levels of education revealed that White/European American women in college reported higher somatization than Chinese American college women. 35 However, it is important to note that the Chinese American students in this study were significantly older and had significantly higher class standing compared with European American students in the study, which might suggest that age and confidence in academic performance might contribute to somatization. This speculation that should be tested empirically.
Although this review suggests that African American and Hispanic/Latina depressed women are more likely to report somatic symptoms than their non-Hispanic White counterparts, the study has several limitations that need to be addressed. First, Asian immigrants and Asian American women are underrepresented in the literature, highlighting the need to engage further with this population. Of importance is that, although one of the studies included Chinese American women, 35 they were college students who might have differing levels of acculturation that may distinguish them from immigrant Chinese women. Second, because of limitations around the generalizability of many of the studies reviewed, the findings reported here should be interpreted with caution.
A third limitation is the inconsistent use of measures and lack of control of potential confounding variables in the studies reviewed. For instance, although three studies used the SSI developed by Escobar et al., 33 two found racial and ethnic differences within the United States and as a function of place of residence, suggesting that other factors, such as acculturation, might mediate those associations. In addition, the use of the same measure might not yield similar results if depression is measured differently. For instance, although Nadeem et al. 36 also used the SSI with women in the United States, they used the PRIME-MD to assess depression and not the Diagnostic Interview Schedule used by Escobar et al. 33 This might explain the fact that Nadeem et al. 36 did not find significant differences in somatization. Instead, Nadeem et al. 36 found that perceived need for mental health treatment was associated with disparities in somatization, highlighting the need to assess the role of other explanatory variables.
Furthermore, the studies reviewed did not compare somatic symptoms in the same way. For example, one study compared specific symptoms, 35 whereas others compared scores on a somatic scale, highlighting the importance of comparable comparison across studies. Finally, the studies reviewed did not include data on the meaning women ascribed to depression and related symptoms, limiting our understanding about potential unknown factors that might explain observed differences in somatization by race and ethnicity. As such, subsequent studies should include a qualitative component to learn why women of color believe they are depressed, how depression affects how they feel, and assess how symptoms are reported.
Conclusions
In sum, the results from this systematic review suggest that race and ethnicity does matter when examining somatic symptoms in women with depressive symptoms or diagnosed depression. However, so do other meaningful variables, such as education and possibly context, highlighting the need to examine differences using a multifactorial approach.
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors.
Informed Consent
Informed consent was not necessary as human subjects were not involved in data collection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was provided for this research.