
Abstract
Background:
Grand rounds and named lectureships are forums in academic medicine for sharing research, scholarly achievements, and clinical expertise. An invitation to speak at grand rounds is regarded as an honor and is part of the pathway to academic promotion. We describe gender representation relative to the national academic medical workforce among invited speakers at departmental grand rounds and annual named lectures at a large academic medical center.
Materials and Methods:
Lists of external speakers for grand rounds from 2015 through 2017 were obtained from 18 departments and for annual named lectures from 2007 to 2017 from 7 departments.
Results:
Of the 783 invited speakers to the 25 speaker series, there were 178 women (22.7%). The proportion of women speakers for departmental grand rounds ranged from 0% to 59.3%; representation of women speakers was lower than representation in their specialty in 14 of the 18 departments and significantly lower in 4 of the 18 departments. In four departments, there was a higher proportion of women than available in the specialty-specific academic medicine workforce. The proportion of women who spoke at annual named lectures was significantly lower in two of seven lecture series and ranged from 0% to 21.2%. Three departments had no women speakers.
Conclusions:
The underrepresentation of women as speakers is a potential target to improve gender representation and role modeling and provide equitable opportunity for academic advancement. Solutions may include formal diversity and inclusion training, intentional overrepresentation of invited female speakers, and inclusion of women on grand rounds planning committees.
Introduction
Invited speakerships in academic medicine are part of the pathway to promotion as well as a means to network, share ideas and research, and build one's professional reputation. Despite decades of a growing pipeline of women entering medical school, women are less likely than men to attain the highest academic ranks of associate and full professor. 1,2 Recent studies have described a discrepancy between the proportion of women and men presenting at international conferences 3 –7 as well as among grand rounds speakers. 8,9
Grand rounds and named lectureships are forums in academic medicine for disseminating new research, clinical expertise, and scholarly achievements. Grand rounds series are regularly scheduled educational conferences, the vast majority of which are held weekly. Named lectureships are annual events, and the invited speaker typically serves in a visiting professor role, performing additional teaching activities while on campus.
An invitation to speak at grand rounds at another academic institution is generally regarded as an honor and recognition of the speaker's prominence in their field and can provide an opportunity to disseminate their research and to enhance their national reputation and may improve citations of the speakers' published work. In addition, visiting professors are viewed as role models to trainees and junior faculty, and exposure to a diversity of speakers and topics may contribute to retention of women and minorities in academic medicine. 10
In the present study, we sought to determine the gender distribution of external invited speakers at regularly scheduled prominent lecture series, namely grand rounds and named lectureships, at a large academic medical center.
Materials and Methods
This was a retrospective observational study of external invited speakers for major department and divisional grand rounds presentations and named lectures at Mayo Clinic's Minnesota, Florida, and Arizona campuses. The study was deemed exempt by the Mayo Clinic Institutional Review Board. Archived lists of speakers for grand rounds were obtained from departments and divisions who host grand rounds and other regularly scheduled educational conferences for the calendar years 2015 through 2017. In addition, we collected the names of external speakers for annual named lectures for the years 2007–2017 from the Departments of Cardiology and Obstetrics and Gynecology as well as departments that did not have regular invited speakers for grand rounds. An external speaker was defined as one who is not affiliated with Mayo Clinic.
The gender of each speaker was confirmed for the majority of the speakers by using Google and Doximity, the remaining confirmed by an author who knew the speaker. As a surrogate for the pool, we based the expected percentage of women speakers used for our analyses on data from the Association of American Medical Colleges (AAMC), which summarizes the gender representation among medical specialties in a national sample of academic medical centers. For each department, we treat this expected percentage as a constant and compare the observed percentage with the expected using a one-sample test of proportions. The report used is prepared and updated annually for Mayo Clinic by the AAMC.
In addition, for both grand rounds and the named lecture series, a logistic regression analysis was performed to obtain an overall comparison of observed versus expected speaker gender across all departments simultaneously. For the logistic regression model, woman speaker was the dependent variable and the logit of the expected percentage of women speakers for the given department was included as an offset. From this model, the test assessing whether the intercept term was significantly different from zero was used to test whether the overall observed percentage of women speakers was different than expected. In all cases, two-tailed p-values are reported with p < 0.05 used to denote statistical significance.
Results
We obtained speaker lists for grand rounds presentations from 18 departments and divisions (Table 1) and named lectures from 7 departments (Table 2) at Mayo Clinic's Minnesota, Arizona, and Florida campuses. Data in Table 1 reflect speakers at all three campuses except as noted. A total of 664 non-Mayo speakers accepted invitations to present at grand rounds from 2015 to 2017 and 119 non-Mayo speakers spoke at named lecture series from 2007 to 2017.
External Grand Rounds Speaker Gender Versus National Gender Availability by Specialty
Expected percentage of women speakers. Source: Association of American Medical Colleges.
Rochester, MN, only.
Critical Care is composed of consultants from anesthesiology, critical care medicine, and pulmonary critical care medicine and this value represents the mean.
Arizona and Florida only.
CI, confidence interval.
Named/Annual Lectures Speaker Gender Versus National Gender Availability by Specialty
Data are from speakers invited to Rochester, MN, campus of Mayo Clinic.
Expected percentage of women speakers. Source: Association of American Medical Colleges.
Mayo Clinic Cardiovascular Surgery Department does not include thoracic surgery.
No named lectures were held in 2007.
Named lecture series began in 2013.
For grand rounds series, the proportion of external, non-Mayo Clinic women speakers ranged from 0% to 59.3% (Fig. 1). Both Critical Care Medicine and Physical Medicine and Rehabilitation grand rounds had no women speakers during the time frame. Comparatively, 14 of the 18 departments had a lower percentage of women speakers than national representation and statistically significantly lower for 4 of the 18 departments. From the logistic regression model, which included all departments simultaneously, the observed percentage of female speakers was found to be significantly less than expected (p < 0.001).
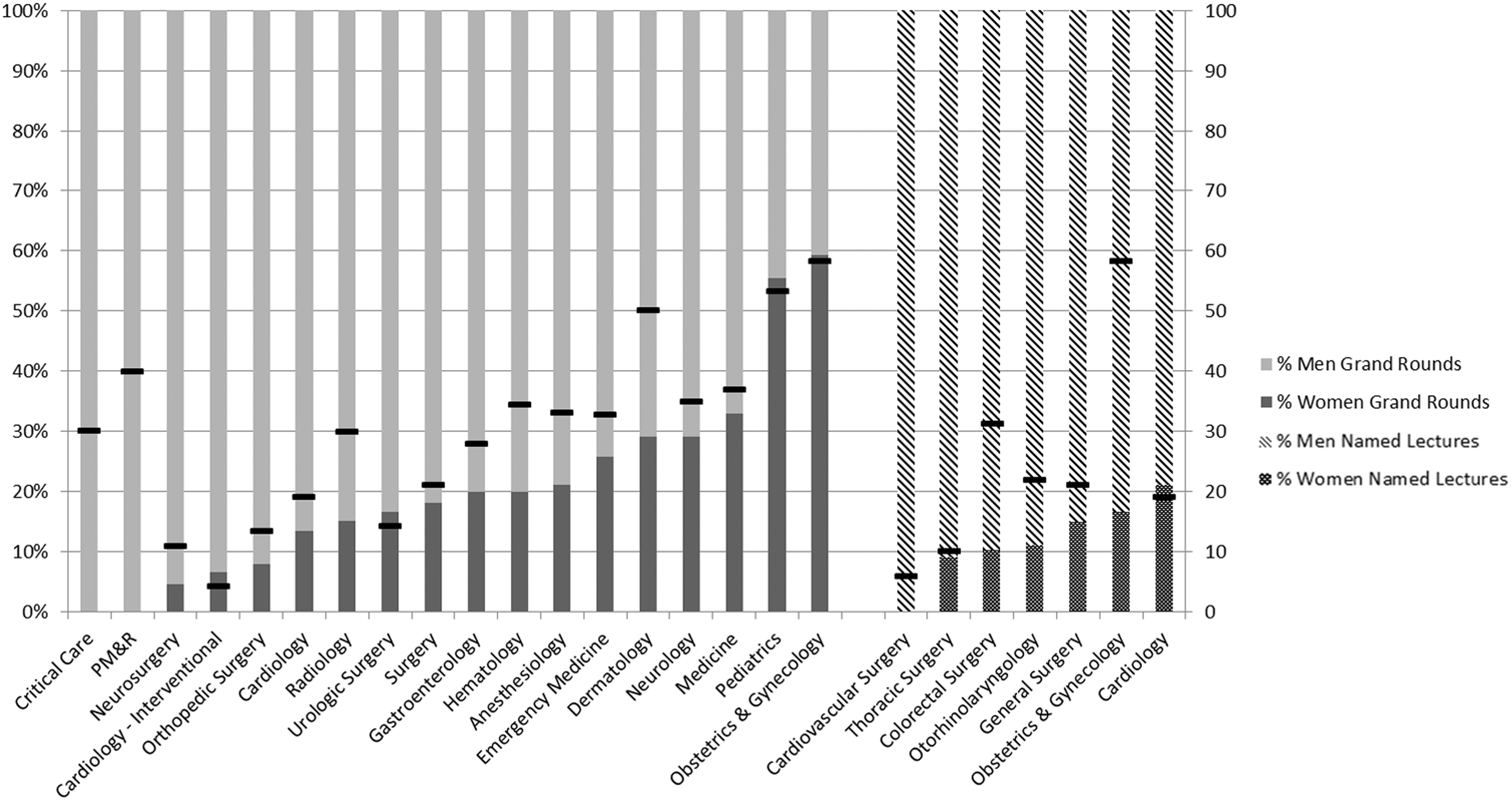
Proportion of women and men speakers for grand rounds and named/annual lectures by specialty. The black line represents the gender representation among medical specialties in a national sample of academic medical centers (Source: Association of American Medical Colleges). PM&R, Physical Medicine and Rehabilitation.
From the department-specific comparisons, the departments with a significantly lower representation include Anesthesiology, Critical Care, Dermatology, and Physical Medicine and Rehabilitation. Four departments (Interventional Cardiology, Obstetrics and Gynecology, Pediatrics, and Urologic Surgery) had a higher percentage of women speakers than the percentage available nationally, but none were statistically significantly higher than the national representation.
Among speakers at annual named lecture series from seven departments, women speakers ranged from 0% to 21.2% (Fig. 1). Compared with the available academic workforce, the proportion of women who spoke at a named lecture was qualitatively lower for six of seven series and two of these were statistically significantly lower. From the logistic regression model which included all departments simultaneously, the observed percentage of female speakers was found to be significantly less than expected (p = 0.016). Cardiovascular Surgery had no women speakers (not significantly different from national representation). Cardiology was the only department that was observed to have higher representation by women than the proportion of women in the specialty, but this difference was not statistically significant (21.2% vs. 19%, p = 0.75).
Discussion
We described the proportion of women as invited, external speakers who presented at grand rounds and named lectures at a large academic medical center. When all departments were analyzed simultaneously, the observed percentage of female speakers was significantly less than expected. Only 5 of the 25 lecture series had a higher representation by women than national availability in that specialty, although not statistically significantly higher. Women speakers comprised a lower proportion of external invited speakers compared with the academic workforce in 19 of 25 speaker series evaluated and were significantly underrepresented in 6 of the 25, and no women spoke in three of the departments' series.
Our findings are similar to recent studies evaluating the gender of speakers at grand rounds and specialty scientific sessions. 6,7 Boiko et al. 8 evaluated grand rounds speakers of nine different specialties over 1 year from various academic medical institutions in the United States and found that women speakers were significantly underrepresented than expected relative to the workforce in all specialties except Obstetrics and Gynecology as well as Surgery. Buell et al. 9 evaluated speakers at internal medicine grand rounds at major academic hospitals in Canada and found 17% more men speakers than women speakers.
Our study evaluated a wider variety of specialties than previous studies. In addition, we elected to focus exclusively on invited external speakers since these individuals are theoretically selected from a national pool of experts whose gender is representative of each specialty. While this national pool of experts has more men than women on average, and more men may hold the academic rank of associate or full professor, which tend to be the rank of those invited, there is still a substantial number of qualified women who could be invited to achieve gender parity. 11 Internal speaker availability is limited to the department or division's gender composition.
The disproportionately low number of women speakers at prestigious speaker venues may be a reflection of both the unconscious and overt bias experienced by women in academic medicine. Numerous studies have demonstrated when compared with men, women physicians are less likely to be promoted to associate and full professor, 1,2 are paid less, 12,13 have fewer scientific publications overall, 14,15 fewer first- and last-author publications, 16 are less likely to receive recognition awards, 17 and are less likely to receive the National Institutes of Health (NIH) funding. 2,18,19 These disparities may also reflect gender differences in access to sponsorship, mentorship, and professional networks.
Although we do not know the gender of the individuals responsible for extending invitations to these speaking opportunities, the narrower networks and low numbers of women in some specialties may render women experts less well known. Presenting in academic forums provides visibility to the speaker, which in turn provides additional opportunities for recognition and academic connections. 20 Even when women are included as speakers at grand rounds, compared with men, they have a higher likelihood of not being acknowledged as experts. 6 Women grand rounds speakers who were introduced by men were less likely to be addressed by their professional title compared with men. 21
Gender disparities can create a vicious cycle in that to be invited to grand rounds, a speaker must be established as an expert in their field; however, this often occurs through speaking engagements and publications. The absence of diversity in speakers sends a clear, if subliminal, message to members of the audience, as to what a leader or expert “looks like.” Since these educational venues are by design aimed at learners and junior faculty, these gaps further perpetuate social norms portraying leaders and experts as men.
Although the majority of departments in this study had a proportion of woman speakers that was not statistically significantly different from the proportion expected from the available workforce, the absolute number of women speakers remained overall small relative to the number of departmental conferences, with only 5 of the 25 lecture series having a higher representation by women than national availability in that specialty. Three departments in the study had no women speakers over the time period of the study. Silver et al. 17 use the term “inexorable zero” as a sign of hidden attitudes that work to exclude women or minorities and may relate to an underlying organizational climate issue.
While it may require more effort to achieve equitable representation of men and women in academic venues, it is important, especially where women have been historically underrepresented as speakers or when the specialty and/or the inviting department have few women faculty. 22 One way to achieve the goal of equitable representation of women and minorities as speakers is for departments and institutions to include this as an accountable metric. Departments could articulate a deliberate goal of “overrepresentation” of women speakers in these prestigious venues, especially in specialties with a very low proportion of women. In addition, women should be represented on grand rounds planning committees. When women are included on a planning committee for scientific symposia, the proportion of women speakers has been shown to increase. 23
We do not have data on the speaker invitation acceptance rate in our study, and theoretically, this could have affected the results, evidence shows that women do not decline speaking invitations more often than men. 20 When women decline an invitation, every effort should be made to identify another woman who could serve as an expert. Implicit bias affects both men and women and can lead to decisions that propagate inequalities and formal unconscious bias training should be implemented.
A limitation of this study is our inability to assess the representation of other dimensions of diversity, especially groups who are underrepresented in medicine such as racial and ethnic minorities and people with disabilities or to account for nonbinary gender representation. Future research could assess some of these factors so as to assure a truly representative agenda of invited speakers at academic medical institutions and medical conferences. In addition, the number of speakers in each series were low and we are likely underpowered to reach statistical significance and resulting in wide 95% confidence intervals. The degrees of the speakers were not included in the analysis, and some of the speakers may not have been physicians, potentially confounding the conclusions we made about woman physician speakers. In addition, assessing gender representation alone does not fully reflect the pool of potential speakers as most invited speakers generally hold the rank of professor or associate professor.
In 2018, 27.8% of male U.S. medical school faculty were full professors and 21.7% were associate professors compared with 13% of women were full professors and 18.6% were associate professors. 11 Furthermore, we were unable to collect data on the individuals responsible for inviting the speakers to these academic conferences or on acceptance rates.
Conclusions
This study provides evidence of gender disparities in the representation of women as invited speakers at a large U.S. academic medical center. Invited speakers are role models for the junior faculty and trainees attending grand rounds. Among other strategies, one way to inspire and encourage women to enter fields historically dominated by men is to expose them to strong successful women in these fields. In addition, when women are invited to speak at another institution's grand rounds, it is an opportunity to increase her visibility, enhance her national reputation, and contribute to her academic promotion.
We should take the findings of this assessment and seek opportunities to increase the number of women speakers in science and medicine, especially in prestigious venues such as grand rounds and named lectures at academic medical centers. There must be a concerted effort to ensure gender equity in invitations to academic forums for all specialties.
Footnotes
Acknowledgment
The authors thank Darrell R. Schroeder, MS, of the Department of Health Sciences Research, Mayo Clinic, Rochester, MN, for statistical support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.