
Abstract
Background:
While many women experience prenatal symptoms of anxiety and/or depression (PSAD), treatment uptake rates are relatively low. Left untreated, symptoms can unfavorably affect maternal and infant health. The first aim of this study was to identify the treatment uptake rate and modalities of treatment received in a community sample of Dutch pregnant women. The second aim was to investigate reasons for not engaging in treatment and to describe facilitators for treatment uptake. The third aim was to determine facilitators and barriers for self-disclosure of feelings to midwives.
Materials and Methods:
Data were collected from a convenience sample of 1439 Dutch women with low-risk mid-term pregnancies in midwifery care. PSAD was assessed with online questionnaires on symptoms. Reasons, facilitators, and barriers were determined with checklists and open questions. Data were analyzed using conventional content analysis and open code quantification.
Results:
Only 15% of women with PSAD (scoring above cutoffs; 22% of the full sample) received treatment. Psychotherapy was the most commonly received treatment. The main reason for not engaging in treatment was regarding PSAD as a natural part of pregnancy (71%). The main facilitator to engage in treatment was referral by midwives (16%), and for self-disclosure was the midwife asking about PSAD (59%), whereas not asking formed the main barrier for self-disclosure (23%).
Conclusions:
Relatively few pregnant women received treatment for PSAD. Midwives play an essential role in identifying and referring women for treatment. Routine screening may be a starting point to offer support and, if needed, referral.
Introduction
Around 20
In midwifery care, taking pregnant women's perspectives into consideration forms an important part of woman-centered care, 18 –21 defined as “the collaborative relation between the woman and the midwife that is shaped through co-humanity and interaction; recognizing and respecting one another's respective fields of expertise.” 21 Applying a woman-centered care approach has been suggested to improve the quality of maternity care. 18,19 Moreover, this approach helps to deliver care in a way that is responsive to pregnant women's preferences and needs, 20 and may beneficially impact women's health status and outcomes. 22,23 Hence, possibilities for detecting maternal PSAD are expected to be larger in woman-centered midwifery care as compared with traditional care. However, before the best woman-centered midwifery care can be implemented, it is essential to first investigate women's perspectives on PSAD, treatment for symptoms, and self-disclosure of feelings.
Previous studies have identified factors that influence treatment uptake in women with PSAD in midwifery and obstetric care settings. These factors can be differentiated at the individual level (i.e., pregnant woman), care provider level (i.e., midwife), and health care system and society level. For example, at the individual level, women with PSAD may not perceive PSAD as a problem that requires treatment. 24 Since depressive symptoms and somatic complaints of pregnancy commonly overlap, women may believe that PSAD is a natural part of pregnancy. 13,25 Additionally, lower self-acknowledgement and self-acceptance of PSAD among women may form a barrier to initiate mental health care treatment. 7 At the care provider level, insufficient detection and low referral rates by care providers contribute to low treatment rates. 13,25 –30 For example, an American study in an obstetrician-provided care setting found that symptoms of depression or anxiety were detected in only 41% of women with PSAD, and of these women only 43% were referred to mental health care professionals for treatment. 13 In the specific case of midwives, a potential cause for low detection includes lack of self-disclosure of feelings by pregnant women. 1 This may lead to less awareness of symptoms by midwives, and consequently, less referral for treatment and treatment uptake. At health care system and society level, long waiting lists and stigma, among others, seem to contribute to low treatment rates. 26,28 –30 Although many factors have been identified that can hinder detection and treatment of PSAD, most studies were conducted in the United States and in obstetrician-provided care settings, and less in midwifery care settings. The investigation of women's perspectives in different maternity care settings is of importance, because they may influence whether women want to engage or not in treatment, and self-disclose feelings to maternity care providers. 31 –33 Moreover, cultural differences exist in women's attitudes toward mental health treatment, making it valuable to study reasons to engage or not in treatment in different populations and cultures. 34,35
This study builds upon previous studies by determining women's perspectives on treatment for PSAD and self-disclosure of feelings to midwives. The sample consists of low-risk Dutch pregnant women, mostly in the second trimester of pregnancy. The aims of the study are (1) to identify the treatment uptake rate and modalities of treatment received in a community sample in The Netherlands; (2) to identify the most mentioned reasons for not engaging in mental health care treatment, as well as to determine facilitating factors for starting treatment; and (3) to determine facilitating factors and barriers of self-disclosure of feelings to midwives. The results of this study may assist midwives and mental health care providers to resourcefully optimize the delivery of maternity care and/or adjust existing approaches for low-risk pregnant women with PSAD. 36
Materials and Methods
Design and setting
The present study employed a cross-sectional study design. Quantitative and qualitative methods were used to provide descriptive information related to the prevalence of PSAD, and women's perspectives on treatment and the provision of care provided by midwives. Ethics approval was obtained from the Faculty of Social Sciences of the Radboud University (ECSW2016-1710-42). Pregnant women were recruited in collaboration with two echo centers, two midwife practices, and one lactation consultant practice. Women from the echo centers received an email with an invitation to fill in the online questionnaire. At the midwife practices and lactation consultant practice, potential participants received a folder with information on the study and a web link to the online questionnaire. The questionnaire was additionally distributed through pregnancy-related Facebook groups.
Participants
A convenience sample of 1439 primarily second trimester pregnant women was included in this study. Participants were recruited from March 2017 to September 2018. After women signed informed consent, they completed the online questionnaire. The majority of the women (95%) were recruited through the two echo centers. The remaining 78 participating women were recruited through the midwife centers (n = 21), lactation consultant practice (n = 11), and pregnancy-related Facebook groups (n = 46) (see Table 1).
Characteristics of Women With and Without Prenatal Symptoms of Anxiety and/or Depression (n = 1439)
Significant differences (p < 0.05) are highlighted bold.
Unless otherwise indicated.
Scores below validated cutoff scores for EPDS (9 or less) and for STAI-S (39 or less).
Scores above validated cutoff scores for EPDS (10 or more) and/or STAI-S (40 or more).
Independent samples t-test was used to determine differences in age, educational level, general health, midwife contact between women with high and low psychosocial distress.
Chi-square test was used to determine the differences in proportions between the two groups.
Other birthplaces were Afghanistan, Bangladesh, Belgium, Brazil, Brunei, Bulgaria, China, Columbia, Dutch Antilles, Philippines, Germany, Greece, Guinea, Hawaii, Ireland, India, Iraq, Italy, Japan, Kuwait, Kosovo, Croatia, Morocco, Nigeria, Norway, Poland, Romania, Ukraine, USA, Sri Lanka, Tunisia, United Kingdom, former Yugoslavia, Vietnam, South Africa, South Korea, and Sweden.
The large number of missing values is due to these questions not being obligatory and being added later to the questionnaire.
Mann–Whitney U test was used to determine differences in STAI-S scores and EPDS scores between women with high and low psychosocial distress.
STAI-S (Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983); scale: 20–80.
EPDS (Cox, Holden, & Sagovsky, 1987); scale: 0–30.
EPDS, Edinburgh Postnatal Depression Scale; IQR, interquartile range; PSAD, prenatal symptoms of anxiety and/or depression; SD, standard deviation; STAI-S, State-Trait Anxiety Inventory.
Inclusion and exclusion criteria
Pregnant women with sufficient knowledge of the Dutch language were included. Exclusion criteria were complicated pregnancies that required specialized maternity care (n = 36), no informed consent (n = 18), and incomplete surveys for demographic data (i.e., age, trimester, parity, ethnic background, education, and employment; n = 493) (see Supplementary Fig. S1).
Demographic measures
The demographic measures included questions on factors that have been associated with maternal prenatal depression and/or anxiety. 37 –42 Respondents reported on marital status, planned pregnancy, smoking, alcohol, common medical problems of pregnancy (yes/no, choices were: “anemia,” “bladder infection,” “hypertension,” “placental malformation,” “pelvic pains,” “infection, namely,” and “other”), stressful life events (yes/no, choices were: “death of a relative/close family member,” “relational/marital problems,” “sickness of oneself,” “sickness of partner,” “divorce/separation,” “financial problems,” “domestic violence,” “other”), pregnancy-related history of mental health (yes/no, choices were: “prenatal depression,” “postnatal depression,” “experienced traumatic birth,” “experienced traumatic pregnancy”), level of education and general health. Level of education was women's highest completed education level ranging from 1 (“primary school”) to 5 (“university or post-graduate education”). For general health, respondents were asked to rate their perceived health on a five-point Likert scale ranging from 1 = poor to 5 = excellent. 41
Furthermore, prenatal depressive symptoms have been associated to more obstetric care visits. 42,43 Therefore, respondents were asked about the total number of appointments they had had with their midwife throughout their pregnancy.
Depressive symptoms
The EPDS, a 10-item questionnaire validated in the Dutch pregnant population, was used to measure depressive symptoms. 17,44 The EPDS inquired on the frequency of depressive symptoms in the preceding 7 days on a four-point Likert scale. Total score ranges between 0 and 30, with a score of ≥10 being indicative for elevated depressive symptoms during pregnancy, and potentially prenatal depression. 44,45 Internal consistency in this sample was good (Cronbach's α = 0.88).
Anxiety symptoms
General symptoms of anxiety during pregnancy were measured using the state scale of the STAI-S. 16 The STAI-S is a validated 20-item tool that measures how anxious one feels at the present moment on a four-point Likert scale. The total score ranges between 20 and 80, with a score of ≥40 indicating increased feelings of anxiety, reflecting an increased likelihood of prenatal anxiety disorders. 45 Internal consistency was excellent in this sample (Cronbach's α = 0.97).
Maternal self-perceived symptoms of anxiety and/or depression
Given that PSAD is a multidimensional concept 1 and outcomes of the EPDS and STAI-S were moderately positively correlated in this sample (Spearman's rho (rs ) = 0.68, p < 0.001), PSAD (STAI/EPDS) was defined as scoring ≥10 on the EPDS and/or ≥40 on the STAI-S. We additionally measured self-perceived PSAD with the question: “Have you experienced depressive symptoms or feelings of anxiety during your pregnancy?” (yes/no). A positive response to the question was classified as PSAD (self-perceived).
Note that only women with PSAD (STAI/EPDS) and PSAD (self-perceived), n = 231 were asked about treatments, reasons for not engaging in treatment and facilitating factors to start treatment.
Treatments
Women were queried on whether they received treatment (yes/no) and, if applicable, what treatment they received (treatment modalities) and the treatment effect on symptoms (no effect/neutral/positive effect). Treatment modalities included “cognitive behavioral therapy,” “eye movement desensitization and reprocessing (EMDR),” “psychoanalysis,” “schema-focused therapy,” “light therapy,” “mindfulness,” “problem solving therapy” (i.e., support with problems in daily life or work), and “other.”
Reasons for not engaging in treatment
A literature search revealed several reasons for not engaging in mental health care treatment among pregnant women. 1,26,28 –30,46 These reasons were combined into a 21-item checklist, where women could choose all reasons that were applicable to them (Table 2).
Reasons for Not Wanting to Receive Mental Health Treatment as Reported by Women with Prenatal Symptoms of Anxiety and/or Depression (n = 124)
Percentages for each reason are calculated from the total number of times reasons were chosen from the list (n = 459). Reasons are ordered from most reported reasons to least reported reasons. The original order in which the items were presented is also provided.
Facilitating factors to start treatment
Facilitating factors to start treatment was assessed by the use of the open-question: “What helped you to start treatment with your mental health care provider?”
Facilitators and barriers for self-disclosure
All women (n = 1439) were asked whether they shared their worries, anxieties, or feelings with their midwife (see care processes, self-disclosure (yes/no), in Table 1). Only women with PSAD (STAI/EPDS) who self-disclosed were asked about facilitating factors for self-disclosing to the midwife: “What helps you to share your worries, anxieties, or feelings with your midwife?” (facilitators). Women with PSAD (STAI/EPDS) who did not self-disclose were queried about barriers for self-disclosing to the midwife: “What withholds you from sharing your worries, anxieties and feelings with your midwife?” (barriers).
Data analysis
Descriptive statistics were used to describe the baseline characteristics of the total group of women. Differences between groups for categorical data and continuous data were calculated by chi-square tests and t-tests, respectively. To answer the research questions, respondents were divided into two groups on the basis of their EPDS (≥10) and STAI-S (≥40) cutoff scores. The prevalence of women scoring above one or both cutoffs, that is, screening positively for PSAD (STAI/EPDS), was determined as a percentage of the total number of included women. To evaluate the relative popularity of each of the 21 reasons for not wanting to receive mental health care among women with both self-perceived and STAI/EPDS PSAD, the percentage of times each specific reason was chosen was calculated. This was done by dividing the total of number of times X reason was chosen by the total number of times all the reasons were chosen, and multiplying this by a hundred. The prevalence of treatment modalities was also calculated in this manner. The prevalence of reasons, facilitators, and barriers was also calculated as a percentage of the total number of reported reasons, facilitators, or barriers. Quantitative data were analyzed using the statistical software R (Version 1.1.463; R studio, 2018) and R-package “car.” 47 Qualitative analyses were based on principles of the Framework method and conducted by two independent coders (P.D.B. and E.M.A.v.T.). 48,49 Both coders coded >50% of the responses to establish a codebook, providing each code with a concrete definition and example quotes from data. The codebook was thereafter finalized through discussion and reaching consensus on codes and definitions. P.D.B. and E.M.A.v.T. then independently used the codebook to analyze all open-ended responses and create a coding table in Microsoft Excel. 50,51 The interrater reliability (IRR) was measured by Cohen's kappa coefficient and percent agreement (i.e., the number of agreed codes over the total number of codes). Good agreement threshold was defined as (κ) >0.60 and >80%, respectively. 52
Results
Preliminary analyses
Maternal characteristics
A total of 1439 questionnaires were analyzed. Participants were predominantly highly educated, employed, married/cohabiting with partner, and around thirty years old. The majority of women were in their second trimester of pregnancy, currently nonsmoking/nondrinking, and considered their physical health to be good. There were significant differences between the women with high and low PSAD (EPDS/STAI) as summarized in Table 1.
Maternal prenatal psychosocial distress
Twenty-two percent of all women scored above the threshold for PSAD (EPDS/STAI) (n = 318; Table 1). Of these women, 63 women (20%) had depressive symptoms (≥10 on EPDS) without comorbid anxiety; 97 women (30%) had symptoms of anxiety (≥40 on STAI-S) without comorbid depressive symptoms; and 158 women (50%) had comorbid depressive symptoms and heightened anxiety. Of the 318 women with PSAD (EPDS/STAI), 231 (73%) had PSAD (self-perceived).
Interrater reliability
IRR between the two authors was good with aκ of 0.84 and 85% agreement for coding of the data.
Main analyses
As mentioned previously, due to the setup of the questionnaire only women with PSAD (EPDS/STAI) and PSAD (self-perceived) (n = 231) were queried about treatments, reasons for not engaging in treatment and facilitating factors to start treatment. All women (n = 1439) were asked about facilitators and barriers for self-disclosure (i.e., sharing worries, anxieties, or feelings with the midwife).
Treatments
A minority of women with PSAD (EPDS/STAI and self-perceived) received treatment for PSAD (n = 35, 15%). Eleven treatment modalities were used, including problem-solving therapy (n = 17, 37%), cognitive behavioral therapy (n = 7, 15%), psychoanalysis (n = 7, 15%), EMDR (n = 6, 13%), schema-focused therapy (n = 3, 7%), mindfulness (n = 1, 2%), and other (n = 5, 11%); that is, grief counseling (n = 1), body-oriented therapy (n = 1), acupuncture (n = 1), counseling by a general practitioner (n = 1), prayer therapy (n = 1)). Two women were unaware of the type of treatment they received (n = 2, 6%). The majority of women (80%) found their treatment effective in reducing symptoms.
Reasons for not engaging in treatment
Of the 231 women with PSAD (EPDS/STAI and self-perceived), 80% indicated that they did not want to engage in treatment, and 124 (48%) of them provided reasons for not wanting to engage in treatment. The most chosen reason was: “depressive and anxiety symptoms are a natural part of pregnancy” (n = 88, 71%) (see Table 2).
Facilitating factors to start treatment
Thirty-nine women (17%) with PSAD (EPDS/STAI and self-perceived) who currently did not receive treatment, indicated that they would like to receive treatment. Twenty-four of them (62%) provided reasons what would help them start treatment. The main facilitating factor included receiving a referral of the midwife for treatment (n = 5, 15%) (Table 3). In addition, of the 39 women with PSAD (EPDS/STAI and self-perceived) currently receiving treatment, 27 women (70%) reported the reasons that had helped them engage in treatment. The main facilitating factor was encouragement by partner/family members (n = 8, 17%) (Table 3).
Facilitating Factors What Would Help to Start Treatment, as Reported by Women with Prenatal Symptoms of Anxiety and/or Depression Not Receiving Treatment (Total N Provided Reasons = 28), and Facilitating Factors that Had Helped to Start Treatment, as Reported by Women with Prenatal Symptoms of Anxiety and/or Depression and Receiving Treatment (Total N Provided Reasons = 37)
Self-disclosure to midwives
Of all women (n = 1439), a total of 1310 women provided a response to the self-disclosure question on whether they shared their worries, anxieties, or feelings with the midwife (yes/no; see Table 1). As shown in Table 1, the proportion of women with PSAD informing their midwives about their feelings was significantly smaller compared with women without PSAD (p < 0.001). Of the women with PSAD, 202 women responded “yes” and were then asked about what facilitated their self-disclosure, and 88 women responded “no” and were asked about what constituted a barrier for their self-disclosure.
Facilitating factors for self-disclosure to midwives
Of the 202 women with PSAD that reported self-disclosure to midwives, 156 (77% out of these 202 women) reported facilitating factors for self-disclosing their feelings to midwives. Facilitating factors fell under seven categories, including self-efficacy, personal gain, midwife style or approach, midwife skills, relationship with midwife, procedures and processes, and other (Supplementary Table S1). The most important facilitating factor for self-disclosure were midwives specifically asking about feelings of depression or anxiety (n = 91, 23%) (Fig. 1A).
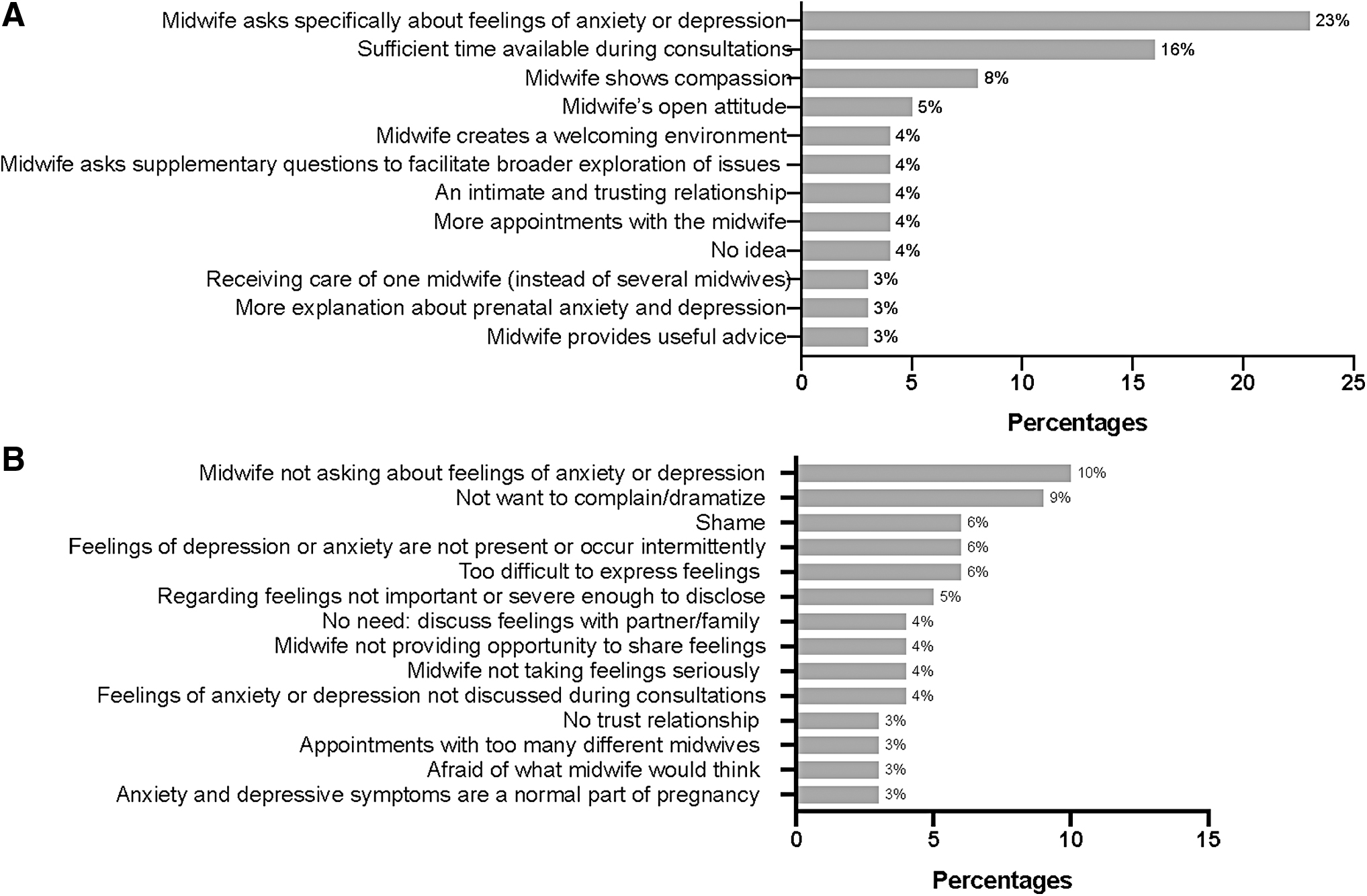
Barriers for self-disclosure to midwives
Of the 88 women with PSAD that reported no self-disclosure to midwives, 87 women reported barriers that withheld them from disclosing their feelings. Perceived barriers were allocated to nine categories, including self-efficacy, perception of anxiety and depression, emotional barriers, personal gain, obliviousness, midwife style or approach, midwife skills, relationship with midwife, procedures and processes, family/friends' support, and professional support (see Supplementary Table S2). The main perceived barrier that withheld women from sharing feelings was midwives not asking about PSAD (n = 17, 10%) (Fig. 1B).
Discussion
The present study sought to contribute to the understanding of the relatively low treatment uptake rate for PSAD. To this end we determined the main reasons, facilitators, and barriers for mental health care treatment and self-disclosure of feelings, among low-risk pregnant women in mid pregnancy with PSAD in a Dutch community sample in the midwifery care setting.
An important finding of the current study is that a midwife specifically asking a woman whether she experiences anxious or depressive feelings improves the chance of self-disclosure. The study findings indicate that this is especially relevant for women with PSAD as they are less likely to share their feelings with midwives compared wit women without PSAD. Additionally, posthoc analyses showed that women with PSAD who shared their feelings with midwives significantly more often received a referral for treatment than women with PSAD who did not share feelings. The present study also found that, for women who desired treatment, receiving a referral for treatment from midwives was the main facilitating factor for engaging in treatment. These findings are in line with the results of previous studies, which reported that patients receiving primary care were more likely to engage in self-disclosure when care providers asked them directly about psychosocial issues, 53 and that a referral for treatment for PSAD during pregnancy is related with improved treatment uptake rate. 13 However, previous studies have reported that maternity care providers sometimes experience barriers for addressing PSAD with pregnant women. These barriers can be internally derived (e.g., lack of experience or general knowledge on how to discuss psychosocial issues) and externally derived (e.g., insufficient time or limited insight into health referral networks). 1,54 –57 Training maternity care providers in how to approach and discuss PSAD with women, and providing them with adequate resources to refer women to specialized mental health care providers, should help overcome these barriers. 58 –60 These barriers can also be addressed by strengthening midwifery practices with easily accessible mental health care providers (e.g., psychologists, nurse practitioners, social workers). 26,61 This method would suit pregnant women's preferences to receive mental health care for symptoms at their maternity clinic. 26
The study results regarding PSAD prevalence and treatment uptake confirm those of previous studies: PSAD was highly prevalent among women with low-risk pregnancies (22%), and relatively few of these women (15%) received treatment. 13,15 The main reason for not engaging in treatment was that women considered PSAD as a natural phenomenon during pregnancy. In contrast to previous studies, almost no women reported structural reasons (i.e., financial and time constraints) or reasons at health care system or society level (i.e., long waiting lists, stigma). 26,28 –30,35,46 The discrepancies may be due to different maternity care settings in previous studies, namely mostly obstetrical care settings. 31 –33 Moreover, previous studies included more women of lower socioeconomic status (SES) 30,46,62 and immigrant background 35 than the current study. Hence, a next step in this line of research would be to replicate our study in populations of low-risk pregnant women of lower SES and more diverse cultural backgrounds. Results of such studies may enable the development of tailored approaches and interventions that enable targeting untreated PSAD for all women in midwifery care. 35 Furthermore, future qualitative research should investigate women's and care providers' perceptions on how it is best to frame and facilitate discussion around PSAD and treatment in the midwifery care setting. These future studies could additionally assess, for example, whether maternity care providers offering psychosocial support and information that places emphasis on resilience and salutogenesis (i.e., focus on promotion of women's wellbeing as a manner of indirectly improving mental wellbeing) 63 may also effectively diminish PSAD in low-risk pregnant women.
The present study found that, for women who desired treatment, receiving a referral for treatment from midwives was the main facilitating factor for engaging in treatment. For midwives to refer women for treatment, they first need to be aware of PSAD. 13 As mentioned above, one way to facilitate midwives' awareness is by directly asking women whether they experience anxiety or depressive symptoms. Another way is by routinely using short questionnaires such as the EPDS and STAI in their practices. These questionnaires should be complemented with questions on relevant risk factors that have been associated with increased risk of mental disorders during pregnancy, such as alcohol use and unplanned pregnancy. 64,65 Elevated scores on these screening instruments can form the basis for discussing PSAD with the woman, facilitating self-disclosure, and offering a referral when necessary. 66,67
As routine screening may facilitate self-disclosure, increased referral rates, and hence increased treatment uptake, implementation of routine screening should be considered for standard care. 66 –70 For routine screening to lead to successful outcomes it needs to be accompanied by sufficient time for women and midwives (and eventually also the mental health care providers associated to the midwife practice) to reflect on outcomes and, in the case of PSAD, to discuss possibilities for addressing PSAD. Sufficient time to reflect on outcomes may also provide time for a possible natural reduction of PSAD. 71 This approach is in line with the Lancet 2016 editorial on screening for perinatal depression, which states that maternity care providers should discuss with positive-screened women the possibility of referral or treatment through sensitive inquiry. 72 Based on the results of the current and previous studies, sensitive inquiry would include maternity care providers demonstrating genuine interest, a readiness to listen, an open attitude, and taking sufficient time to discuss symptoms. 73 –77
Strengths and Limitations
A strength of the study is its relatively large population (n = 1439) of low-risk women in standard midwifery practice. Furthermore, it is the first study to describe the most frequently reported reasons, facilitators, and barriers at the individual care provider and health care system/society levels that contribute to untreated PSAD among low-risk pregnant women in a midwifery care setting in the Netherlands. The methods used allow deriving practical recommendations for maternity care providers from the findings and help inform the development of future interventions. Also, the current study is characterized by its novel approach of combining the qualitative research method of conventional content analysis with open-coded quantification.
Despite the strengths of the present study, limitations should also be noted. First, the current sample may not accurately reflect the Dutch population of low-risk pregnant women, as most women that filled in the online questionnaires were relatively highly educated (only 37% had lower secondary education or lower). Moreover, depressive symptoms and heightened anxiety was defined as scoring above the threshold on validated questionnaires, and not by clinical evaluation. 78 Furthermore, treatment uptake rate was only calculated among women scoring above the threshold for PSAD and with a positive answer on the “self-perceived PSAD” question. This method may have produced a less exact estimation of treatment uptake, as there were women that scored above the cutoffs but did not report perceiving PSAD. Given that these women did not report experiencing PSAD, it is reasonable to assume that most of them did not receive treatment. Hence, the calculated treatment uptake rate may be an overestimation of treatment uptake in low-risk women with heightened pregnancy PSAD.
Future directions
Next to pregnant women, partners also go through the process of transformation toward parenthood, which may negatively affect partners' levels of distress. 79 –81 Therefore, future studies should include partners when assessing mental health needs and views on interventions to inform about or manage partner psychosocial distress. Efforts to reduce potential partner distress are of importance as they can positively influence maternal wellbeing during pregnancy, with potential benefits for infants as well. 82 –84 Preventive interventions that could be assessed include psychoeducation on psychosocial distress during childbirth preparation classes and peer support groups for couples. 46 These interventions may help to prevent psychosocial distress in both pregnant women and their partners, as they provide the opportunity to share experiences, improve symptom recognition among partners, discuss changes during pregnancy, and increase acknowledgment and validation of the woman's and partner's feelings by one another. 85,86 Results of the current and a previous study showed that especially the latter two can help women to open up about PSAD and can empower them to initiate treatment. 7 Evidence of this type of research may inform midwives on how to adjust management strategies for parental psychosocial distress according to couples' needs and preferences, and hence facilitate personalized, client-centered care. 87 Furthermore, the current study highlights the many different treatments offered to women with PSAD. Given the relatively small number of women receiving treatment (n = 35), we were unable to provide separate analyses with sufficient statistical power on the specific treatment options for prenatal depressive symptoms or anxiety separately. Given the importance of recommending women with PSAD suitable and effective treatments, further research should investigate specific treatment options used for prenatal depression and anxiety separately in larger groups of women receiving treatment.
Conclusions
PSAD is often present among low-risk pregnant women in mid pregnancy. However, few of these women engage in treatment. Midwives, in their role as gatekeepers in maternity care, play an essential role in identifying PSAD and, if necessary and desired, referring for treatment. Routine screening for PSAD may offer a starting point for midwives, and possibly also for maternity clinic mental health care professionals, to execute these tasks, offer support, and provide psychoeducation for women and their partners.
Footnotes
Acknowledgments
The authors thank all the women that participated in the study and gratefully acknowledge Christy Bowerman (C.B.), Carola Groen (C.G.), Emma Baljet (E.B.), Gea Vogelzang (G.V.), Henrike Haugke (H.H.), Hilal Sekban (H.S.), Ilse van de Ven (I.v.V.), Loes Maurits (L.M.), Martine Hollander (M.H.), Monique van Tooren (M.v.T.), Olga van den Berg (O.v.B.), Petra Kuiper (P.K.), Petra Schermers de Bruijne (P.S.B.), Sabine Speel (S.B.), and Siegrid Hoekstra (S.H.) for their contributions to this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
C.d.W.'s work was supported by the Jacobs Foundation Advanced Research Fellowship and the VICI grant from the Netherlands Organization for Scientific Research (
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.