
Abstract
Background:
Inadequate and excessive gestational weight gain (GWG) is associated with adverse health outcomes for mother and child. Health care providers are well positioned to help women achieve appropriate GWG. This systematic review examined associations between women's report of provider advice on GWG and women's compliance with the Institute of Medicine (IOM) GWG guidelines.
Materials and Methods:
In March 2019, PubMed, EMBASE, and Cochrane CENTRAL databases were searched. Observational studies were eligible if published from 1990 to 2019, described provider advice on GWG, and determined whether women's target or actual GWG was consistent with the 1990 or 2009 IOM guidelines. Heterogeneity across studies precluded the use of meta-analytic methods.
Results:
Seventeen cross-sectional and cohort studies of poor to good quality, representing 20,717 women were included. Approximately 69% of women reported provider advice on GWG during pregnancy; however, only 50% reported provider advice consistent with IOM guidelines. Eleven studies found that provider advice on GWG was significantly associated with women's compliance with IOM guidelines, and six studies found no association.
Conclusions
: While a high percentage of women report provider advice on GWG, accuracy of reported advice is less than optimal. The evidence examining associations of provider advice and women's compliance with guidelines is mixed and limited by methodological concerns. Future studies using more robust methods in diverse populations are needed to confirm the role of provider advice in optimizing GWG. Intervention studies are also necessary to increase the proportion of providers who accurately counsel their patients on appropriate GWG to improve health outcomes.
Introduction
The Institute of Medicine (IOM) first published gestational weight gain (GWG) guidelines in 1990 with the goal of optimizing health outcomes in women and their offspring. 1 These guidelines were then updated in 2009 to reflect the current state of maternal and fetal medical research. 2
Weight gain outside the ranges recommended by the IOM is associated with adverse health outcomes for both mother and child. Inadequate GWG increases the risk of infant mortality, preterm birth, and intrauterine growth restriction. 2 –4 Women with excessive GWG are at increased risk for gestational diabetes, 5 –7 preeclampsia, 8 –10 and cesarean delivery. 9 Furthermore, infants born to mothers with excessive GWG are more likely to experience low 5 minute Apgar scores, meconium aspiration syndrome, and large-for-gestational-age compared to women who gain within the recommended guidelines. 11,12 After birth, women with excessive GWG are at increased risk for postpartum weight retention and the development of new or persistent obesity, 13 –15 and their children also have a higher risk of obesity. 16 –20
Despite the known adverse health outcomes associated with inadequate or excessive GWG, less than one-third of women gain weight within the recommended guidelines during pregnancy. 3,21 Due to the low prevalence of appropriate weight gain in pregnancy, the American College of Obstetrics and Gynecology (ACOG) issued a statement in 2013 that all health care providers who care for pregnant women (henceforth referred to as providers) should determine a woman's body mass index (BMI) at the initial prenatal visit and counsel her on the benefits of appropriate weight gain, nutrition, and exercise, as well as the need to limit excessive weight gain to achieve optimal pregnancy outcomes. 22 The implication of this statement is that providers are well positioned to play an important role in helping women achieve appropriate weight gain during pregnancy, and there is evidence that diet and physical activity interventions during pregnancy, many with provider involvement, may limit GWG. 23 –25
Several studies since the release of the 1990 and 2009 IOM guidelines have examined patient–provider communication on GWG in the prenatal care setting, including a recent narrative review highlighting inconsistencies in weight communication. 26 Studies have additionally examined women's report of provider advice on GWG and consistency with the IOM guidelines, including whether provider advice concordant with guidelines was associated with women's compliance with IOM guidelines. However, to date there has been no systematic review to synthesize the existing literature on this topic. The objectives of this study were to determine (1) the prevalence of reported provider advice on GWG consistent with the IOM guidelines during pregnancy and (2) whether report of provider advice is associated with women's compliance with IOM guidelines.
Materials and Methods
A systematic review of the literature was performed to assess the association between provider advice on GWG and women's compliance with IOM guidelines. The study was registered by The International Prospective Register of Systematic Reviews (PROSPERO) (CRD42019142638) and followed the criteria outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 27,28 This study was exempt from Institutional Review Board review.
Information sources and search strategy
The searches were developed and conducted by a health sciences librarian trained in systematic review searching. Search strategies using subject headings and keywords were created for PubMed, Embase (Elsevier), and Cochrane CENTRAL (Wiley). The databases were searched from 1990 to 2019. The date restriction was applied to retrieve results published after the publication of the 1990 IOM weight gain guidelines. The searches were conducted on March 1 of 2019, and the results were limited to human studies published in English. The database search strategies are available in Supplementary Table S1. Database records were deduplicated using the Bramer method. 29 Reference lists of included articles were also screened.
Eligibility criteria
Studies were included if they described provider advice on GWG (exposure), reported women's target or actual GWG, and described whether women's GWG was below, within, or above the 1990 or 2009 IOM guidelines (outcome). The PICOS selection criteria (population, intervention or exposure, comparison, outcome, and study design) are presented in Table 1. We excluded case studies, experimental study designs, articles published before 1990, and studies not in English. Experimental study designs (clinical trials and other intervention studies) were excluded because recently published systematic reviews of GWG interventions illustrate that these are multicomponent programs; 24,30,31 thus, we would be unable to disentangle the effect of women's report of provider advice on GWG compared to the other program components (e.g., nutrition counseling).
PICOS Criteria, Provider Advice, and Gestational Weight Gain: a Systematic Review
BMI, body mass index; GWG, gestational weight gain; IOM, Institute of Medicine.
Study selection
Two independent reviewers (C.B. and H.T.) screened the titles and abstracts yielded by the search against the inclusion criteria. Abstracts judged to have met the initial screening criteria were retrieved as full-text articles. The same two independent reviewers screened the full-text articles for relevant PICOS information for inclusion in the final review. Disagreement between the two reviewers was resolved by a third reviewer (K.M.W.). Reasons for exclusion were recorded.
Data extraction and synthesis
Data were extracted with the use of a predesigned template and included details of the study (e.g., year published, enrollment period, and sample size) and data on study participants (e.g., age, race/ethnicity). In addition, several aspects of the study methods were extracted, including but not limited to how provider advice on GWG was determined, how women's GWG was estimated, methods for categorizing provider advice and women's GWG according to IOM guidelines, and statistical approach. For the results, we extracted details of provider advice on GWG, details of women's GWG, and effect estimates. Two reviewers (C.B. and K.M.W.) extracted the data independently. Disagreement between the two reviewers was resolved through discussion, with a third reviewer (R.R.) consulted as needed.
To enhance comparability across studies, we calculated the percentage of women who reported provider advice below, within, or above IOM guidelines using only those who reported receiving GWG advice as the denominator (rather than the total study population, as reported in several studies 32 –37 ). Similarly, we calculated the percentage of women with a target or actual GWG below, within, or above IOM guidelines using only those who had data on GWG as the denominator (rather than the total study population, as reported in one study 32 ). When possible, percentages were calculated if not reported in the study, but adequate detail provided for calculations. 38 –42 Details of calculations are reported in Supplementary Table S2.
Formal meta-analytic methods were not used to estimate the effect of the exposure on the outcome because of the heterogeneity in included studies. However, pooled averages were calculated by summing the mean values multiplied by the sample size and dividing this number by the sum of the sample sizes. The pooled averages represented the average percentage of providers who advised women on GWG, whether provider advice was below, within, or above IOM guidelines, or if provider advice was reported but not quantified, and women's target or actual GWG, classified as below, within, or above IOM guidelines. Pooled averages were reported overall and stratified by women's GWG assessment method (target or actual). As we did not have the sample variance for each study estimate, we calculated the standard deviation of the population proportion
Risk of bias of included studies
The quality or bias of each study was assessed using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 43 Two reviewers (C.B. and K.M.W.) independently rated the studies on 13 unique criteria, with 96% agreement. Differences were resolved and specification of study quality (good, fair, or poor) was determined through discussion between the reviewers.
The NIH Quality Assessment Tool does not have prespecified scoring thresholds to facilitate classification. 43 Therefore, the writing group outlined 5 contextually appropriate criteria that were necessary for the study to receive a good quality rating: (1) cohort study design; (2) exposure assessed before outcome; (3) provider advice on GWG assessed >20 weeks gestation but before delivery; (4) women's GWG measured or ascertained through medical chart abstraction; and (5) gestational age at delivery accounted for in the study design or analyses. Studies rated as fair quality met 3–4 of these criteria, and studies rated as poor met <3 of the criteria.
Results
Study selection
For this systematic review, we identified a total of 3,917 distinct references in the electronic databases. We excluded 3,860 references on the basis of their titles and abstracts not describing provider advice on GWG and/or reporting women's GWG. We retrieved the full text of the remaining 58 articles. After critical evaluation, 41 of the articles did not meet the selection criteria and were excluded. No additional studies were identified by reviewing reference lists. We included a total of 17 articles in the systematic review. Figure 1 shows the flowchart of the selection process.
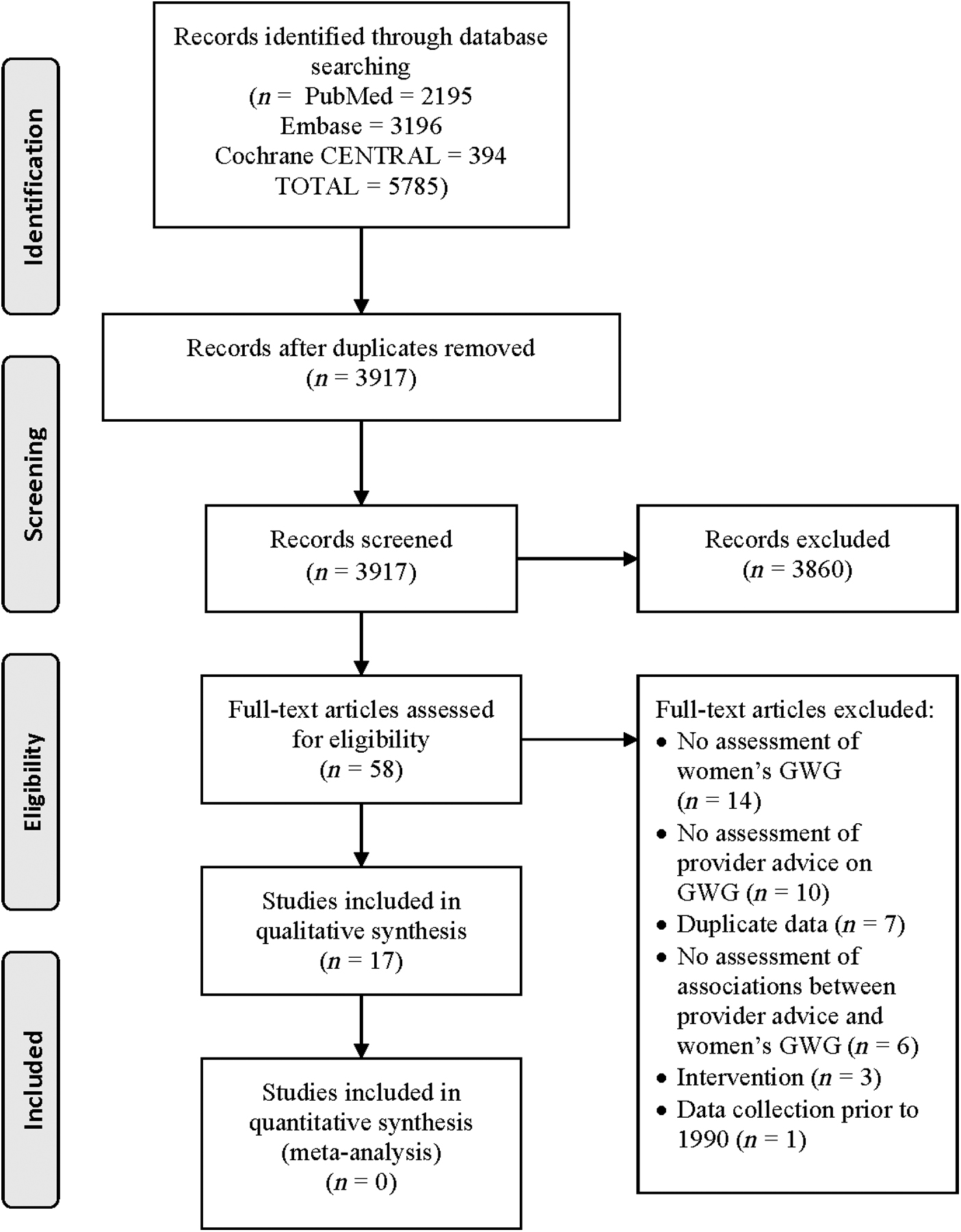
PRISMA 2009 flow diagram. Figure depicts the PRISMA flow diagram for studies identified and excluded. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
Table 2 depicts the characteristics of the included studies and populations. Of the 17 articles included in the review, 10 were cross-sectional surveys 32,33,36,37,42,44 –48 and seven were cohort study designs. 34,35,38 –41,49 The articles included a total of 20,717 participants, with sample sizes ranging from 91 to 7,125. The pooled average age was 29.9 years, with an approximate age range of 16–44 years. The majority of studies included predominately (>50%) white participants. However, three studies were conducted primarily with black/African American participants, 34,35,42 two with Hispanic/Latina participants, 36,44 and one particularly diverse study included Asian, black, Latina, and white women. 38 The majority of the studies were conducted in the United States, with three including participants from Canada 32,41,48 and one from Australia. 47
Study Characteristics
NR, not reported.
Enrollment period not reported in the article text but requested and received from corresponding author.
Sample size used for analysis (n = 310) differed from what was reported in the article (n = 330).
Risk of bias of included studies
Using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies, 3 studies were rated as good quality, 35,42,49 10 as fair, 32 –34,36–41,48 and 4 as poor, 44 –47 (Supplementary Table S3).
Assessment methods
As seen in Table 3, women self-reported provider advice on GWG in all studies with one exception, where provider advice on GWG was extracted from audio recordings of prenatal visits. 42 The majority of studies assessed women's report of provider advice on GWG during pregnancy; however, in five studies, women recalled provider advice in the postpartum period. 33,34,36,37,47
Methods of Assessing Provider Advice on Gestational Weight Gain, Women's Gestational Weight Gain, Compliance with the Institute of Medicine Gestational Weight Gain Guidelines, and Statistical Approach
Using the 1990 IOM guidelines, the recommendation for GWG is 28–40 lbs for underweight women (BMI <19.8 kg/m2), 25–35 lbs for normal weight women (BMI 19.8–26.0 kg/m2), 15–25 lbs for overweight women (BMI >26.0–29.0 kg/m2), and ≥15 lbs for obese women (≥29.0 kg/m2). Using the 2009 IOM guidelines, the recommendation for GWG is 28–40 lbs for underweight women (BMI <18.5 kg/m2), 25–35 lbs for normal weight women (BMI 18.5–24.9 kg/m2), 15–25 lbs for overweight women (BMI 25.0–29.9 kg/m2), and 11–20 lbs for obese women (BMI ≥30 kg/m2).
The 1990 IOM guidelines did not indicate an upper weight gain limit for obese women; thus to categorize obese women into compliance categories the same upper weight gain limit used for overweight women (25 lbs) was applied to obese women.
Not reported in the article, but adequate detail provided to calculate.
Women's self-reported target GWG was reported in six of the studies, 32,38,44 –46,48 with the remaining studies reporting actual GWG. The method of estimating actual GWG varied across studies, including self-report, 39,47 study measured weight, 41 birth certificate data, 33,36 and medical chart abstraction. 34,35,37,40,42,49 Women's self-reported target GWG was assessed during pregnancy, while actual GWG was determined between 32 and 36 weeks gestation using study measured weights, 41 at the last prenatal visit weight, 35,40,42,49 or in the postpartum period. 33,34,36,37,39,47
Given that the IOM guidelines for GWG vary by prepregnancy BMI, the method for determining prepregnancy BMI was extracted. Nearly half of the studies used self-reported prepregnancy weight and self-reported height to calculate prepregnancy BMI. 32,33,39,41,46 –49 Four studies used self-reported prepregnancy weight and measured height, 34,42,44,45 while others used measured weight and height in the first trimester, 35 medical record abstraction, 37,40 or birth certificate data. 36
When examining whether women's target or actual GWG was consistent with IOM guidelines, nearly all studies classified weight gain as below, within, or above IOM guidelines based on the woman's prepregnancy BMI category (underweight, normal weight, overweight, and obese). Due to small sample sizes, three studies dichotomized compliance with IOM guidelines as below/within versus above and below/above versus within. 40,42,48 Two studies used a ratio of observed weight gain to expected weight gain, which accounts for gestational age at delivery. 36,49 Six of the studies used the 1990 IOM guidelines, 36,38,39,45,46,49 one did not specify if the 1990 or 2009 guidelines were used, 47 and the remaining studies used the 2009 IOM guidelines for classification.
The majority of the studies used logistic regression in their analyses examining the associations of women's report of provider advice with women's compliance with IOM guidelines, and adjusted for a variety of potential confounders, including but not limited to prepregnancy BMI, age, race, education, marital status, parity, and gestational age at delivery.
Given that GWG will vary based on gestational age at delivery, methods for accounting for gestational age at delivery were extracted among the studies reporting actual (not target) GWG. Of the 11 studies examining actual GWG, less than half accounted for gestational age at delivery in their methods or statistical approach. 35,36,42,46,49 However, the remaining studies restricted analyses to women with full-term pregnancies (37–42 weeks) 33,34,37,40,41 or excluded women who had infants weighting <5 pounds at birth or an infant stay of >3 days in the ICU, which would indicate preterm delivery. 39
Provider advice on GWG
The percentage of women who reported receiving any provider advice on GWG varied widely from 24.0% to 81.1% across studies (Table 4). When calculating pooled averages, ∼68.5% (95% CI: 67.8–69.1) of participants reported receiving GWG advice from their provider. Of those who reported provider advice, 16.7% (95% CI: 16.1–17.3) reported advice below IOM guidelines, 50.1% (95% CI: 49.3–50.9) reported advice within guidelines, and 20.9% (95% CI: 20.3–21.6) reported advice above guidelines across studies.
Associations of Provider Advice on Gestational Weight Gain and Women's Compliance with the Institute of Medicine Gestational Weight Gain Guidelines, Stratified by Method of Assessing Women's Gestational Weight Gain (Target or Actual)
aOR, adjusted odds ratio; aPR, adjusted prevalence ratio; aRR, adjusted risk ratio; CI, confidence interval; NA, not applicable; NR, not reported.
Original values reported using total sample as denominator, authors recalculated percent using those who reported receiving advice as the denominator.
Original values reported using total sample as denominator, authors recalculated percent using those who reported target or actual GWG as denominator.
Women's ideal and expected GWG reported in article; expected GWG reported in present study.
Not reported in article, but adequate detail provided to calculate.
Reporting doctor advice only (not midwife) due to incomplete data.
Women's target and actual GWG reported in article; actual GWG reported in present study.
Pooled averages were calculated using available data by summing the mean values multiplied by the sample size for each sample, and dividing this number by the sum of the sample sizes. The standard deviation of the population proportion
Figure 2 depicts the percent of women who reported any provider advice on GWG and those who reported IOM-consistent advice by study enrollment year (not publication date) to examine trends over time and potential differences before and after the release of the 2009 IOM guidelines. More than 50% of women reported receiving provider advice on GWG in six of the nine represented studies in 2009 or prior (67%), compared to five of the eight studies with enrollment after 2009 (63%). Similarly, >50% of women reported provider advice on GWG consistent with IOM guidelines in five of the five studies in 2009 or prior (100%), compared to two of the six studies after 2009 (33%).
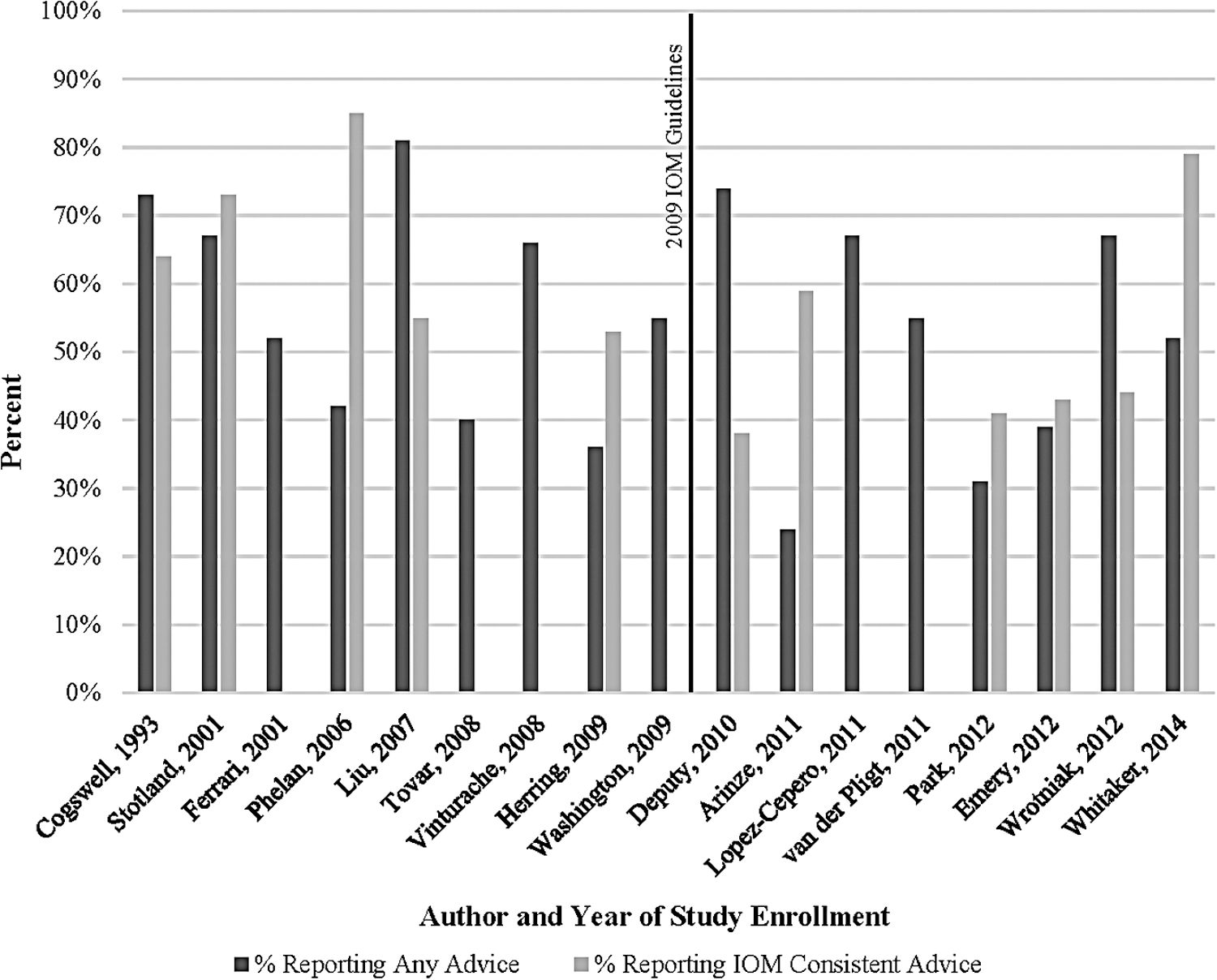
Percent of women reporting any provider advice on GWG and advice consistent with IOM guidelines by study enrollment year. Figure depicts the percentage of women who report any provider advice on GWG, and among those reporting any provider advice, whether or not this advice was consistent with IOM guidelines by study enrollment year. GWG, gestational weight gain; IOM, Institute of Medicine.
Women's GWG
Across studies, ∼21.2% (95% CI: 20.6–21.8) of women had a target or actual GWG below IOM guidelines, 35.5% (95% CI: 34.8–36.1) within guidelines (13.0%–78.9%), and 43.6% (95% CI: 42.9–44.3) above guidelines (range 9.3%–70.0%). When stratifying studies by target or actual GWG, a higher percentage of women reported a target GWG within IOM guidelines (62.6%) (95% CI: 60.7–64.6) compared to studies reporting actual GWG (31.7%) (95% CI: 31.0–32.4).
Associations of women's report of provider advice and women's compliance with IOM guidelines
As seen in Table 4, 10 of the 17 studies included in this systematic review (59%) found a significant association between women's report of provider advice on GWG and women's compliance with IOM guidelines, using target or actual GWG. 32,33,35,36,38,39,42,44,46 Women who reported receiving any advice on GWG were more likely to have an accurate GWG target or goal 44 and were less likely to experience excessive GWG. 42 Women who did not report provider advice on GWG were at higher risk for both inadequate and excessive GWG. 33,36,38,39
When women's report of provider advice was classified according to the IOM guidelines (below, within, and above), four studies found that advice below guidelines was associated with increased risk of inadequate GWG, 33,36,38,39 and four studies found that advice above guidelines was associated with increased risk of excessive GWG, 32,33,36,39 with odds or prevalence ratios ranging from 1.4 to 5.5. Three studies dichotomized provider advice on GWG, concluding that discordant advice was associated with excessive GWG 35 and target weight gain outside of IOM guidelines, 48 and concordant advice was associated with a target weight gain within IOM guidelines. 46 Lopez-Cepero et al. found that women's report of provider advice was not associated with women's GWG; however, women who reported following advice had lower odds of excessive GWG. 40 The remaining six studies found no association between women's report of provider advice on GWG and women's compliance with IOM guidelines. 34,37,41,45,47,49 The risk of bias (assessed as good, fair, or poor) was distributed relatively equitably across studies reporting an association between women's report of provider advice and women's GWG and those finding no association.
Discussion
Main findings
This systematic review presents a summary of the existing literature examining the association of women's report of provider advice on GWG with women's compliance with the IOM weight gain guidelines. Overall, 17 studies met our inclusion criteria, including 20,717 participants. Across studies, ∼69% of women reported receiving provider advice on GWG during their pregnancy. However, only 50% of women reported provider advice consistent with IOM guidelines based on the woman's prepregnancy BMI category. When examining the associations of women's report of provider advice with women's compliance with IOM guidelines, results were mixed, with 10 studies reporting significant associations, one study showing significant associations among women who reported following provider advice, and six studies reporting no significant association.
Comparison with existing literature
An important finding in this study is the relatively high percentage of women who reported provider advice on GWG across studies. It is encouraging that more than two-thirds of women report provider advice on weight gain during their pregnancy, which indicates that providers are aware of the risks of inappropriate weight gain during pregnancy. This finding is in line with a study by Power and Schulkin who found that over 75% of Obstetrician/Gynecologists agreed that excessive GWG is a major health concern. 50 Furthermore, a narrative review by Weeks et al. found that providers report counseling their pregnant patients on the risks of excessive GWG. 26
However, it is problematic that only 50% of women across studies reported provider advice consistent with IOM guidelines. This contradicts findings by Power and Schulkin, where nearly all providers (80%) reported modifying GWG recommendations based on a woman's prepregnancy BMI, 50 yet is consistent with Weeks et al., where IOM consistent advice ranged widely from 9% to 85% across studies. 26 These variations in findings may be due to (1) inaccurate reporting of provider GWG advice by women, which is of particular concern when assessment of advice occurs in the postpartum period; (2) inaccurate classification of women's prepregnancy BMI; and/or (3) providers not accurately modifying GWG recommendations using prepregnancy BMI.
Interestingly, women's report of provider advice on GWG and advice consistent with IOM guidelines did not appear to improve after release of the 2009 IOM guidelines. While ACOG and many other organizations globally have adopted the IOM GWG guidelines, these updates were met with controversial reactions from some providers who believed that the weight gain targets were too high for overweight and obese women. 22 Little is known about the extent to which the IOM guidelines have been adopted, which may partly explain the less than ideal prevalence of women reporting IOM consistent advice.
When comparing women's target and actual GWG, over 60% of women reported a target within IOM guidelines; yet, only 32% of women gained weight within guidelines, with ∼50% exceeding guidelines. There is a clear disconnect between the amount of weight women intend to gain during pregnancy and the amount of weight women actually gain, indicating a critical need to develop more effective interventions to facilitate appropriate GWG.
Lifestyle interventions have shown to be effective at reducing the risk of excessive GWG and related complications. 24,25,51 However, the high cost of dietary and physical activity interventions currently limit dissemination to the larger public despite evidence that these interventions are cost-effective. 52 Enhancing provider counseling on GWG throughout pregnancy could be a cost-effective and feasible intervention approach with broad dissemination potential if shown effective. Notably, a one size fits all approach emphasizing that provider counseling alone may not be adequate to modify behavior for all women. This was illustrated by Daley et al., who observed no difference in excessive GWG among women randomized to an intervention of regular weighing and feedback from community midwives compared to usual maternity care. 53 This indicates that stratified approaches with more intensive interventions may be needed for some, particularly those at higher risk for excessive GWG.
To our knowledge, no previous systematic reviews have examined the associations of women's report of provider advice on GWG with women's compliance with IOM guidelines. However, others have explored the relationship of provider weight loss counseling and weight-related behavior change in adult populations. Rose et al. published a literature review and meta-analysis in 2017, reporting a positive effect of weight loss advice on overweight and obese patient's weight loss behavior. 54 In random effects meta-analysis, the mean weighted effect size for patient weight loss efforts was an odds ratio of 3.85 (95% CI: 2.71–5.49), indicating a statistically significant impact of provider advice. It is important to note that this review examined weight loss behaviors and not weight loss itself. However, this gives credibility to the concept that provider advice can play an important role in facilitating lifestyle behavior change.
Methodological concerns of reviewed studies
The present study findings should be interpreted with caution due to several methodological concerns. First, over half the studies were cross-sectional surveys, thus limiting our ability to establish temporality. Second, assessment of provider advice in the postpartum period may increase the likelihood of recall bias, compared to assessment in late pregnancy. Notably, several studies assessed women's report of provider advice on GWG early in pregnancy (e.g., 10 weeks gestation) and thus did not capture provider advice that may have occurred at subsequent prenatal visits. Third, all but one study assessed women's report of provider advice on GWG and did not verify or confirm provider report of advice. However, it is arguably more important to assess women's perceptions of provider advice, as this is a clear indication of what type of advice women remembered receiving. Fourth, the majority of studies used self-reported prepregnancy weight and height to calculate BMI. While prepregnancy weight has shown to be reliable and valid, 55,56 there is also literature showing that overweight and obese women are more likely to underreport their weight, 57 potentially leading to differential misclassification of prepregnancy BMI and concordance with IOM guidelines. Fifth, there was variation across studies in the use of the 1990 or 2009 IOM guidelines to classify women's GWG. The difference in guidelines may lead to altered conclusions, with women classified according to the 2009 IOM guidelines being more likely to be categorized as gaining weight in excess of guidelines compared to women classified according to the 1990 guidelines. 21 This is due to the differences in BMI thresholds between guidelines and because that the 1990 IOM guidelines had no upper GWG limit for obese women. Sixth, it is concerning that less than half of articles reporting actual GWG accounted for gestational age at delivery in their methods or statistical approach. However, authors who did not account gestational age at delivery did attempt to control for this indirectly by only including women with full-term pregnancies in analyses.
Strengths and limitations
This study contributes to the existing literature by systematically reviewing the available evidence examining associations of women's report of provider advice on GWG with women's compliance with the IOM guidelines. However, several limitations of the present review should be noted. Nearly, all studies were conducted in North America, which limits generalizability to other geographical areas and populations, such as Asian populations who use different regional BMI categories when assessing GWG. 58 Publication bias may be present as the current review only included studies in English that were published as peer-reviewed journal articles or abstracts. In addition, there was heterogeneity in the study sample, exposure, and outcome measures, which prevented the use of meta-analytic methods.
Conclusion
Based on this systematic review, it appears that a high percentage of women recall GWG advice from their providers during pregnancy. However, only 50% of women report advice consistent with IOM guidelines. When examining associations of provider advice on GWG with women's compliance with IOM guidelines, study findings were mixed, and it is difficult to draw clear conclusions given the methodological limitations of the articles. However, when significant effects were found, they favored the finding that accurate advice was associated with appropriate GWG.
To further advance the field, more studies are needed to assess the impact of provider advice on women's GWG using prospective cohort study designs, where women's report of provider advice is ideally assessed at multiple points during pregnancy and confirmed by the provider. Furthermore, medical chart abstraction should be used to ascertain prepregnancy BMI and total GWG, and authors should use appropriate methods to account for gestational age at delivery to accurately classify weight gain according to IOM guidelines. Interventions are needed to better prepare providers to accurately counsel women on appropriate weight gain during pregnancy.
Footnotes
Acknowledgments
The authors acknowledge University of Iowa undergraduate students Ms. Hailee Talbot and Ms. Rachel Ryan for their assistance in reviewing titles, abstracts, and data extraction forms.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.