
Abstract
Introduction:
Chronic diseases in the United States are the leading drivers of disability, death, and health care costs. In women of reproductive age (WRA), chronic disease and related risk factors can also affect fertility and reproductive health outcomes. This analysis of trends from 2011 to 2017 adds additional indicators and updates an analysis covering 2001–2009.
Methods:
Data from the 2011–2017 Behavioral Risk Factor Surveillance System were analyzed for 265,544 WRA (18–44 years). To assess trends in 12 chronic conditions and related risk factors, we calculated annual prevalence estimates and adjusted prevalence ratios (APRs) with predicted marginals accounting for age, race, Hispanic ethnicity, education, and health care coverage.
Results:
From 2011 to 2017, prevalence decreased for current smoking (20.7%–15.9%; p < 0.001), gestational diabetes (3.1%–2.7%; p = 0.003), and high cholesterol (19.0%–16.7%; p < 0.001); prevalence increased for depression (20.4%–24.9%; p < 0.001) and obesity (24.6%–27.6%; p < 0.001). After adjustment, in 2017 WRA were more likely to report asthma (APR = 1.06; 95% confidence interval [CI] = 1.01–1.11), physical inactivity (APR = 1.08; 95% CI = 1.04–1.12), obesity (APR = 1.15; 95% CI = 1.11–1.19), and depression (APR = 1.29; 95% CI = 1.25–1.34) compared with 2011. They were less likely to report high cholesterol (APR = 0.89; 95% CI = 0.85–0.94) in 2015 compared with 2011, and current smoking (APR = 0.86; 95% CI = 0.82–0.89) and gestational diabetes (APR = 0.84; 95% CI = 0.75–0.94) in 2017 compared with 2011.
Conclusions:
Some chronic conditions and related risk factors improved, whereas others worsened over time. Research clarifying reasons for these trends may support the development of targeted interventions to promote improvements, potentially preventing adverse reproductive outcomes and promoting long-term health.
Introduction
In the United States in 2017, about one-third (32.9%) of deaths in women of reproductive age (WRA) (15–44 years) were the result of chronic conditions, including cancer, heart disease and stroke, chronic liver disease, cirrhosis, diabetes, and chronic lower respiratory diseases. 1 Some chronic conditions and related risk factors (e.g., smoking, obesity, asthma, high blood pressure, diabetes, depression, and heavy and binge drinking) are associated with adverse perinatal health outcomes, including perinatal infections and complications, preterm delivery, low birthweight, macrosomia, infant illness and death, and higher hospital charges. 2 –15 In addition, many of these same chronic conditions and related risk factors (e.g., smoking, obesity, high blood pressure, diabetes, physical inactivity, high cholesterol, and depression) contribute to heart disease, a leading cause of maternal death. 16 This is particularly concerning because the decline in heart disease mortality from 2000 to 2015 among women younger than 45 years (6.6% relative decline) was about half that of men younger than 45 years (12.5%) and lower than declines among women in other age groups (21.5% for women 45–64 years of age and 39.0% for women 65 years and older). 17
The American Heart Association emphasizes the importance of promoting healthy lifestyles to prevent and control coronary heart disease in women. 18 These strategies include quitting cigarette smoking and avoiding exposure to secondhand smoke, maintaining a healthy weight, engaging in physical activity, maintaining a heart-healthy diet, and controlling high cholesterol, high blood pressure, and diabetes. 18 Preventing and managing these risk factors and conditions in WRA is an integral goal of preconception care and can improve pregnancy outcomes and the overall health of women. 19,20 However, WRA are not commonly receiving all recommended preventive health services including preconception counseling, diabetes screening, high blood pressure screening, flu vaccination, and smoking cessation counseling, and disparities in receipt of services have been reported by age, race/ethnicity, and federal poverty level status. 21
The surveillance of trends in chronic disease and related risk factor measures guide public health prevention and management efforts. Recent studies have examined some population-level trends in the prevalence of individual chronic diseases and risk factors among WRA. 5,22 –25 However, the last review that we are aware of covering a broad spectrum of risk factors and chronic conditions among WRA covered the years 2001–2009. 26 This previous analysis showed that nearly all risk factors worsened over the time period evaluated and now is an important time to determine if trends continued to worsen or have stabilized. Since that publication, there has also been an increasing recognition of other chronic conditions impacting long-term health including depression, binge drinking, gestational diabetes mellitus, and pregnancy-related high blood pressure. The objective of this study was to build on that previous analysis by assessing trends covering the years 2011–2017 and adding additional indicators to this analysis among WRA.
Methods
We performed serial cross-sectional analyses of data from the Behavioral Risk Factor Surveillance System (BRFSS). The BRFSS is a state-based, random-digit telephone survey of the US noninstitutionalized, civilian population, 18 years of age and older. We analyzed self-reported data from 265,544 women 18–44 years of age who participated in the 2011, 2013, 2015, and 2017 BRFSS surveys, and lived in one of the 50 states or the District of Columbia. The survey includes both landline and cellular phone numbers and follows a standardized protocol to collect responses. This large survey includes core questions that are rotated with odd numbered-years having the specific chronic conditions and risk factors assessed in this study. Additional information is available online (
Measures
We examined five chronic conditions (high blood pressure, high cholesterol, diabetes, depression, and asthma), five traditional chronic disease risk factors (current smoking, physical inactivity, heavy alcohol consumption, binge drinking, and obesity), and two pregnancy-related chronic disease risk factors (pregnancy-related high blood pressure and gestational diabetes) among WRA. The pregnancy-related risk factors were included because they are associated with adverse birth outcomes and increased risk of chronic disease for the mother. 29 –34 We refer to these measures collectively as chronic conditions and related risk factors.
The chronic conditions were considered present if the woman reported she had ever been told by a doctor, nurse, or other health professional that she had the condition, with the exception of high cholesterol, which also required a self-report of ever having had her cholesterol checked. Because of changes in the 2017 survey collection of self-reported history of having cholesterol checked, we limited data analysis to the years 2011–2015. For diabetes, the question did not differentiate between type 1 or type 2 diabetes.
Current smoking was defined by self-report of smoking at least 100 cigarettes in one's lifetime and still smoking at the time of the survey. Physical inactivity was defined as a “no” response to the question: “During the past month, other than your regular job, did you participate in any physical activities or exercises such as running, calisthenics, golf, gardening, or walking for exercise?” The wording in questions about the frequency of alcohol use changed slightly over time, and that measure is referred to as heavy drinking in this article. In 2011 and 2013, it was defined for women as self-reported alcohol consumption of >1 drink/day for the past 30 days. In 2015 and 2017, it was defined for women as having more than seven total drinks in the past week. Binge drinking was defined for women as having four or more drinks on one or more occasions in the past month and that definition was consistent over the time period studied (
The pregnancy-related risk factors were determined from follow-up questions among women who said they had been diagnosed with diabetes or high blood pressure. Those women were asked if the condition occurred only during pregnancy.
Covariates
Covariates were selected based on a literature review of characteristics that are commonly associated with chronic disease and based on their inclusion in the BRFSS data set. Age was categorized into three groups (18–24, 25–34, and 35–44 years). Self-identified race and Hispanic ethnicity were categorized as non-Hispanic white, non-Hispanic black, Hispanic (any race), Asian, American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, or All Others. The “All Others” group comprised women who identified themselves as other racial groups, those who indicated more than one race, and those who did not report a race. Education level, based on highest grade or year of school completed, was categorized as not completing high school (<12 years), completing high school or its equivalent (12 years), 1–3 years of college or technical school, or college graduate (four or more years of college). Access to health care was defined as having any health care insurance coverage based on the question: “Do you have any kind of health care coverage, including health insurance, prepaid plans such as HMOs, or government plans such as Medicare?”
Exclusions
A total of 276,510 WRA were surveyed over these four time periods. Women who were pregnant at the time of the survey (4.0%, n = 10,966) were excluded because they are likely to change their behaviors and report different risks owing to social concerns, perceptions, and health recommendations such as not smoking or drinking alcohol. 35,36 This resulted in an overall sample of 265,544 nonpregnant female respondents. Women with missing information on any chronic condition or related risk factor were excluded from their respective analyses. Missing information ranged from 0.1% for high blood pressure (n = 369) to 7.9% for physical inactivity (n = 21,038). In the full multivariate models, observations for each individual model were excluded from each analysis if there were any missing information on covariates. Missing information on covariates ranged from 0% (age and race/ethnicity) to 0.4% (health insurance coverage).
Statistics
Annual prevalence estimates and 95% confidence intervals (CIs) were calculated for each chronic condition and related risk factor. An unadjusted analysis of linear trends of prevalence estimates based on orthogonal polynomials using Proc Descript polynomial were performed across survey years. Using survey year as the dependent variable, predicted marginals were used to estimate adjusted prevalence ratios (APRs) individually for each risk factor and chronic condition. 37 This approach allowed the assessment of the overall trend accounting for differences in the covariates of age, race, Hispanic ethnicity, education, and health care coverage. The data were weighted to reflect each state's noninstitutionalized civilian population and combined into a national analysis. SAS (version 9.4) and SAS callable SUDAAN (version 11.0) were used to account for the complex sampling design to provide weighted population estimates and calculate accurate variance estimates.
Results
Selected population estimates
Overall, 26.7% of the sample population were 18–24 years of age, 36.3% were 25–34 years, and 37.0% were 35–44 years (Table 1). Just over half the population were non-Hispanic white (55.1%), and 20.3% were Hispanic. One-third attended some college (33.9%), and more than one-fourth were college graduates (28.2%). Four in five had health insurance coverage (80.8%). The distribution for many sociodemographic population estimates changed over time: higher estimates of non-Hispanic whites in 2011 and 2013 compared with the later years; lower estimates of Hispanics in 2011 compared with 2013, 2015, and 2017; lower estimates of Asians in 2011 and 2013 compared with the later years; higher estimates of those with less than high school education in 2011 and 2013 compared with 2017; lower estimates of college graduates in earlier years compared with 2017; and lower estimates of having health care insurance coverage in earlier years compared with 2015 and 2017.
Characteristics of Adult Women of Reproductive Age, Behavioral Risk Factor Surveillance System 2011–2017
Unweighted sample size.
Weighted estimate.
CI around the weighted estimate.
BRFSS, Behavioral Risk Factor Surveillance System; CI, confidence interval; GED, General Education Diploma; HS, High School; NHOPI, Native Hawaiian or Other Pacific Islander.
Changes in chronic conditions and related risk factors
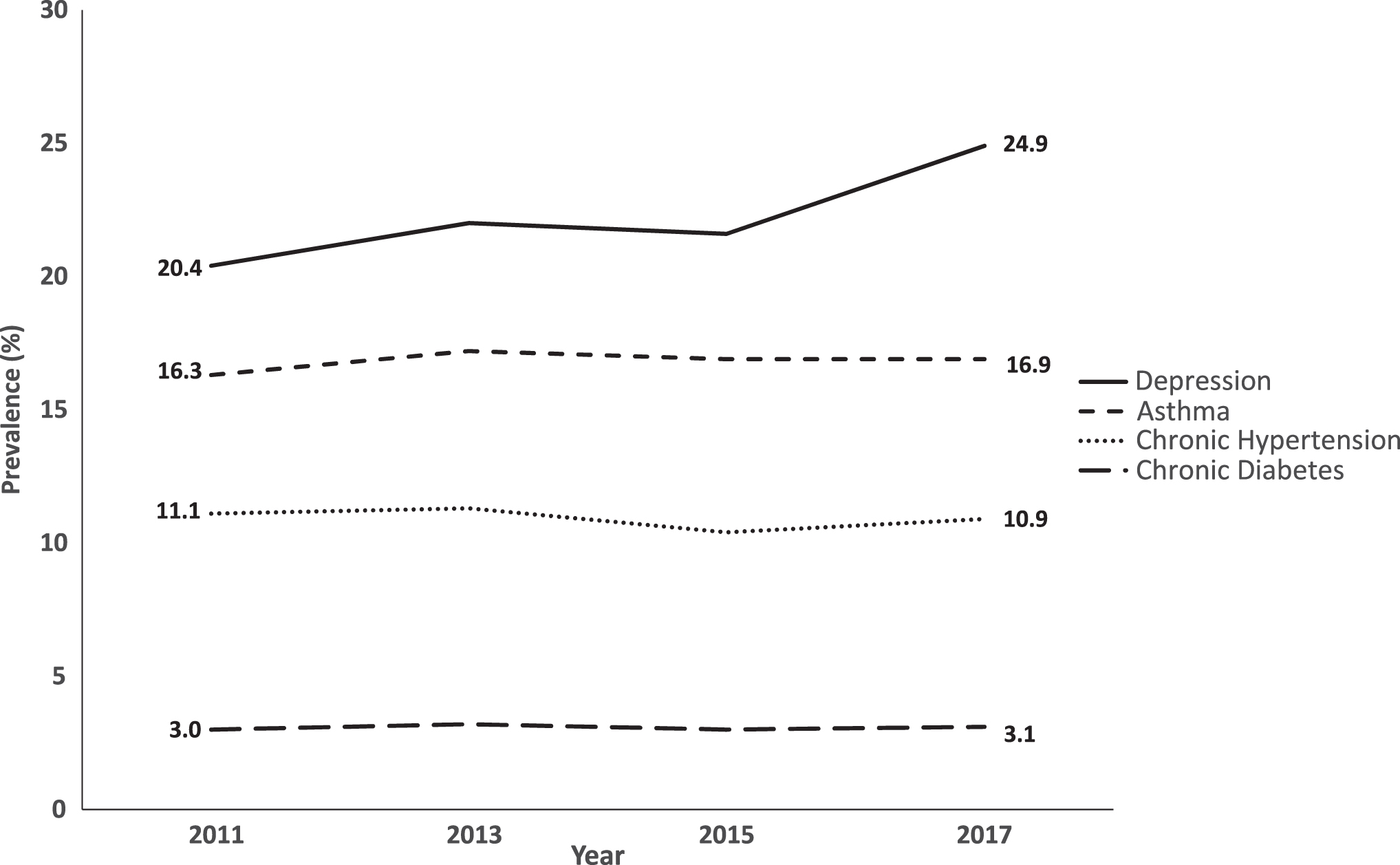
Among chronic conditions studied (Table 2 and Fig. 1), unadjusted prevalence estimates for depression (20.4% in 2011 and 24.9% in 2017; p < 0.001) increased and decreased for high cholesterol (19.0% in 2011 and 16.7% in 2015; p < 0.001). After adjustments (Table 3), WRA were less likely to have high cholesterol in 2015 compared with 2011 (aPR = 0.89, 95% CI = 0.85–0.94) and more likely to have asthma (aPR = 1.06, 95% CI = 1.01–1.11) and depression (aPR = 1.29, 95% CI = 1.25–1.34) in 2017 compared with 2011. There were no significant differences in the prevalence of diabetes or high blood pressure.
Trends in selected chronic conditions among women of reproductive age (18–44 years); 2011–2017.
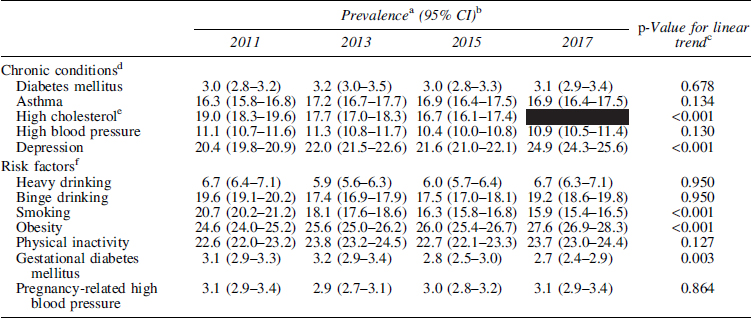
Prevalence of Chronic Conditions and Risk Factors by Year Among Adult Women of Reproductive Age, Behavioral Risk Factor Surveillance System 2011–2017
Weighted estimate.
CI around the weighted estimate.
Linear trend test based on orthogonal polynomials with comparison for 2017 prevalence to 2011 except for high cholesterol, which compares 2015–2011.
Women were categorized with a chronic condition if they had ever been told by a doctor or other health professional that they had the condition.
The BRFSS question for high cholesterol in 2017 was substantially different from that of the other years, and thus not included in the analysis. Shading refers to estimate not available.
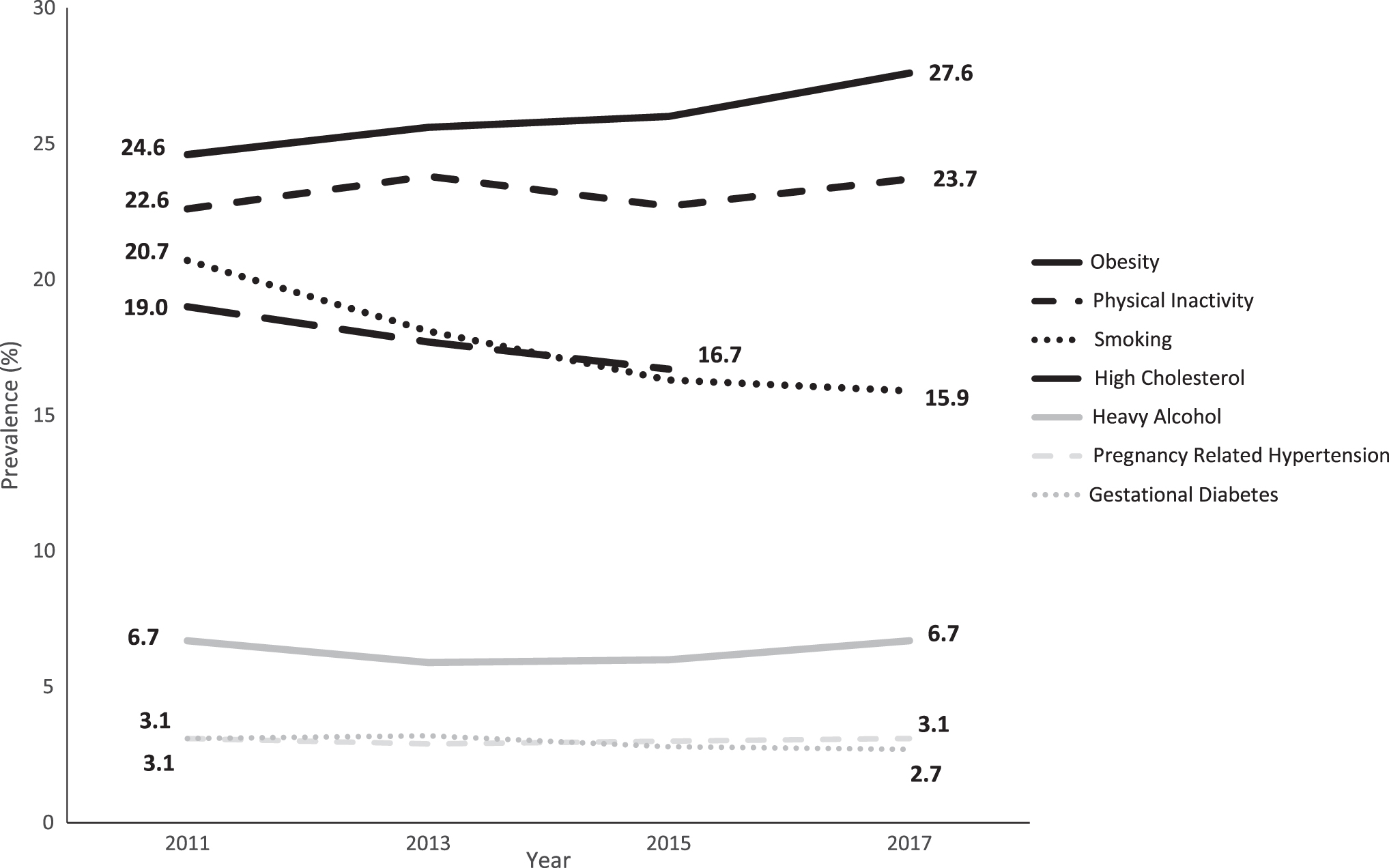
Heavy drinking defined as on average intake of >1 drink/day; Binge Drinking defined as intake of 4 or more drinks in one sitting in past 30 days; Smoking defined as having smoked >100 cigarettes in lifetime and currently smoking; Obesity defined as body mass index ≥30.0 kg/m2; and Physical Inactivity defined as no leisure time physical activity in past 30 days; Gestational diabetes mellitus and Pregnancy-related high blood pressure based on having the respective condition only during pregnancy.
Prevalence Ratios for Chronic Conditions and Related Risk Factors Among Adult Women of Reproductive Age, Behavioral Risk Factor Surveillance System 2011–2017
Ratios and CIs in bold depict significance at the p < 0.05 level; Individual models were used to assess difference between 2017 and comparison year of 2011 except for high cholesterol, which used 2015.
CI around the weighted prevalence ratio estimate.
Individual model for each risk factor and chronic condition were adjusted for age, race/ethnicity, education, and health care coverage.
Women were categorized with a chronic condition if they had ever been told by a doctor or other health professional that they had the condition.
The BRFSS question for high cholesterol in 2017 was substantially different from that of the other years, and thus not included in the analysis.
Heavy drinking defined as on average intake of more than 1 drink/day; Binge drinking defined as intake of four or more drinks in one sitting in past 30 days; Smoking defined as having smoked >100 cigarettes in lifetime and currently smoking; Obesity defined as body mass index ≥30.0 kg/m2; and Physical inactivity defined as no leisure time physical activity in past 30 days; Gestational diabetes mellitus and Pregnancy-related high blood pressure based on having the respective condition only during pregnancy.
Among the related risk factors studied (Table 2 and Fig. 2), unadjusted prevalence estimates increased for obesity (24.6% in 2011 and 27.6% in 2017, p < 0.001) and decreased for current smoking (20.7% and 15.9%, p < 0.001) and gestational diabetes (3.1% and 2.7%, p < 0.003). After adjustments (Table 3), WRA were less likely to smoke in 2017 compared with 2011 (APR = 0.86, 95% CI = 0.82–0.89) or have gestational diabetes (APR = 0.84, 95% CI = 0.75–0.95), yet were more likely to have obesity (APR = 1.15, 95% CI = 1.11–1.19) and be physically inactive (APR = 1.08, 95% CI = 1.04–1.12). There were no significant differences over time in the prevalence of heavy drinking, binge drinking, and pregnancy-related high blood pressure.
Trends in selected related risk factors for chronic conditions among women of reproductive age (18–44 years); 2011–2017.
Discussion
This study updates trends for the chronic conditions and related risk factors identified in a previous study of 2001–2009 data and also describes trends for new measures of pregnancy-related conditions, binge drinking, and depression. 26 This study shows continued worsening trends in obesity and asthma and continued improvement for smoking. In contrast with the previous study, the prevalence of high cholesterol has decreased, and physical inactivity levels worsened. We did not observe significant changes in high blood pressure or diabetes prevalence, which were previously reported to be worsening. 26 Of the new measures in this study, there were increases in depression, declines in gestational diabetes, and no changes in pregnancy-related high blood pressure or binge drinking from 2011 to 2017.
Measures demonstrating improved trends
In the general population, declines in smoking are attributed to increased prices, increased awareness of the dangerous health effects of smoking, improved access to cessation services, clinical interventions, and policies that limit smoking in public places. 38,39 These approaches are likely influencing the declines in smoking among WRA. The use of electronic cigarettes was not included in the survey over the full period studied, so we did not assess it. However, such use might explain whether the declining trend in smoking if WRA are substituting vaping for cigarette smoking. The US Preventive Services Task Force found insufficient evidence for the benefits or harms of electronic cigarettes to make a recommendation on cessation for adults, including pregnant women. 40 Because potential harms are unknown, it is important to include all potential forms of smoking in prevention messaging when possible to ensure continued reduction in smoking-related disease. 39,41
The reasons for declining prevalence of high cholesterol may be related to the changing cholesterol guidelines and clinical practice patterns. 42 –45 In the general population based on National Health and Nutrition Examination Survey (NHANES), there was no change from 2003–2004 to 2012–2014 in low-density lipoprotein serum levels 46 or from 2012 to 2017 in high-density lipoprotein serum levels. 45 The improvement in gestational diabetes seen in this study contrasts with worsening trends noted from birth certificate data (2012–2016) over a similar time frame. 24 These different findings may be the result of the data sources used. BRFSS data are self-reported, but birth certificate data are reported by clinicians. Earlier NHANES data showed a nonsignificant change in gestational diabetes from 8.4% in 2007–2008 to 10.4% in 2013–2014. 47 The BRFSS survey does not collect particular classes of medication used, so any association with changes in medication use over time on the trends could not be assessed in this article. The continued assessment of trends in the various data sources, including validation with medical records, can help guide clinical and public health programs in their efforts to reduce the prevalence of chronic conditions and related risk factors.
Measures demonstrating worsening trends
The overall prevalence of asthma has increased over time, particularly in women. 48 Asthma in pregnancy is increasingly recognized as a contributor to adverse outcomes in both mothers and children. 13,49 Therefore, improving awareness, prevention, clinical screening, and control of asthma could help improve birth outcomes and decrease the health and social consequences of asthma. The continued worsening trends of obesity among WRA reported in this study are consistent with the significant increases in obesity in the United States overall. 46 The increasing physical inactivity noted in this study coupled with the increasing obesity is concerning. The worsening trends for physical inactivity diverge from the improvements noted in the past decade (2001–2009) among WRA. 26 These results also contrast with the overall population trends from 2005 to 2017 that showed no change in physical inactivity. 50 Increasing physical activity among WRA can improve their health.
Of note, the largest worsening change in this study was observed with depression, and this pattern of worsening is consistent with the increases in depression rates reported among women who had a delivery from 2000 to 201522 and among nonpregnant WRA based on NHANES data from 2007 to 2014. 51 Nearly a quarter of WRA report a diagnosis of depression, representing a large opportunity for public health action, which may help reduce the impact of this chronic condition.
Chronic conditions and related risk factors may also be better detected owing to changes in health insurance coverage or an increased emphasis on screening in those with health insurance coverage, but the data to assess this were not available to characterize the impact. In addition, risk factors and chronic conditions are often co-occurring and addressing one may lead to improvement in another. For example, a meta-analysis of lifestyle interventions among overweight or obese WRA also demonstrated reduction in symptoms of depression and anxiety. 52 Therefore, surveillance and management efforts should consider individual chronic conditions and related risk factors and the possibility that they may co-occur.
Measures with no significant change
From 2011 to 2017, the prevalence of heavy drinking, binge drinking, diabetes, pregnancy-related high blood pressure, and high blood pressure did not change. The lack of change in heavy drinking from the previous to this study is concerning. 53 Nearly 1 in 5 WRA reported at least one binge drinking occasion in the past 30 days, which is alarming, given the general and reproductive health consequences of drinking during pregnancy. 54,55
The leveling of high blood pressure is consistent with that seen in the general population based on NHANES data from 2001–2002 to 2015–2016. 56 The lack of a significant change in pregnancy-related high blood pressure is somewhat opposed to that shown in previous time periods 1980–2010, 1987–2004, and 1993–2014 based on administrative hospital data. 57 –59 The lack of an increase seen in our study with more current data may represent a plateauing prevalence or use of a different data set, and further investigation may be warranted. Preventing complications of pregnancy-related high blood pressure through early clinical management was shown to be effective in a recent study and highlights the importance of early recognition and treatment of this risk factor. 60 Clinical recognition and management of high blood pressure among WRA who had high blood pressure during pregnancy could also reduce their risk of heart disease and stroke. 9,61
The lack of change in diagnosis of diabetes is consistent with stable estimates that are based on birth certificate data among women who had a live birth from 2012 to 2016. 24 Clinical and behavioral interventions to prevent type 2 diabetes are underused among WRA. 62 Improving clinical management and population-level awareness of chronic conditions and related risk factors may help women achieve better reproductive and long-term health.
The findings in this study are subject to limitations. The BRFSS collects self-reported information, which is subject to recall and social desirability bias (e.g., underreporting actual weight, smoking, and alcohol intake, and overstating physical activity). The chronic condition questions only reflect self-reported diagnosed conditions and thus miss undiagnosed chronic conditions. However, a recent study that aggregated 2011–2016 NHANES data based on both self-reported diagnoses and clinical measurements demonstrated very similar estimates of high blood pressure (9.3%) and diabetes (4.5%) among WRA. 63 Unawareness of having chronic conditions also varies by demographic characteristics, as demonstrated with diabetes. 64 Therefore, the assessment of trends over time may not take into account various population subgroups, which limits interpretation of these trends. Furthermore, misclassification is possible because of possible misunderstandings of the differences between pregnancy-related high blood pressure or gestational diabetes and chronic hypertension and diabetes. The finding of increasing prevalence of some chronic conditions could be related to increasing health insurance coverage as people are more likely to see a health provider if they have insurance and thus have more opportunities to be diagnosed with a condition. 65 –67 The survey data do not indicate how long respondents have been diagnosed with a condition, so any effects related to a new diagnosis because of recently obtaining health insurance coverage or having an increase in covered preventative services during the study period could not be assessed.
The purpose of this article was to provide an update of trends in the prevalence of chronic conditions and related risk factors, including pregnancy-specific conditions, among WRA. These conditions and risk factors can affect reproductive health and lead to chronic disease. Implementing the CDC guidance on preconception care (
Footnotes
Acknowledgments
The authors acknowledge the support and assistance from Fleetwood Loustalot in Division for Heart Disease and Stroke Prevention at the Centers for Disease Control and Prevention who assisted in oversight and general review of the analysis and article.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.