
Abstract
Background:
Few studies have investigated the association between violence against pregnant women in terms of recurrence, complications, and perpetrators of violence, and breastfeeding duration. This study verifies whether recurrent violence, violence with pregnancy complications, and intimate partner violence (IPV) against pregnant women are associated with shorter exclusive breastfeeding up to the infant's 6th month and breastfeeding up to the 12th month of life.
Materials and Methods:
A cohort study with a convenience sample of 1,146 pregnant women was performed. Follow-up assessments were conducted at birth, and at 12–36 months. Survival analysis was used to verify whether recurrent violence, violence with pregnancy complications, and IPV were associated with reduced duration of exclusive breastfeeding and breastfeeding.
Results:
The adjusted Cox regression revealed no difference regarding exclusive breastfeeding duration among mothers exposed or not exposed to violence and according to who perpetrated the violence. The risk of an infant not being breastfed within the first 12 months of life increased in cases of violence before/during pregnancy (95% confidence interval [CI] = 1.03–1.88), recurrent psychological/physical/sexual violence during pregnancy (95% CI = 1.11–1.92), recurrent psychological violence (95% CI = 1.05–1.96), and recurrent physical/sexual violence (95% CI = 1.01–2.39). Violence with pregnancy complications (95% CI = 0.94–2.22) was not associated with breastfeeding interruption. Similar risks of breastfeeding interruption were observed for IPV (95% CI = 0.96–1.87) and violence perpetrated by other family members (95% CI = 0.83–1.89).
Conclusions:
We observed a shorter breastfeeding duration up to 12 months of life in cases of recurrent violence.
Introduction
The World Health Organization recommends that infants be exclusively breastfed during the first 6 months of life and that from this age on they continue to be fed breast milk supplemented with other nutritionally adequate and safe foods until they are 2 years of age or older. 1,2 Even though the advantages of breast milk over any other food or liquid in the first 2 years of life are widely acknowledged, 1 –6 the most recent Brazilian survey on breastfeeding (2013) shows that 37.1% of Brazilian infants were exclusively breastfed until the 6th month of life and that 45.4% and 52.1% were breastfed until the first and second years of life, respectively. 7
While factors associated with exclusive breastfeeding cessation have been frequently investigated, 3,8 –18 few studies have assessed the effect of violence against pregnant women on breastfeeding duration. 19 –23 In addition, there is predominance of cross-sectional studies 21,23,24,26,28 –31 on intimate partner violence (IPV) 20 –23,26 –31 and studies on the recurrence 23,30 and severity 28 of violence are scarce; some studies have assessed exclusive breastfeeding at 6 months as outcome, 21,24,27,28 but no study has yet evaluated breastfeeding beyond 6 months of age or used survival analysis to determine whether violence against pregnant women could reduce breastfeeding duration. 19 –23
In the United States, the 2004–2014 and 2000–2003 Pregnancy Risk Assessment Monitoring System (PRAMS) did not find any association between IPV during pregnancy and breastfeeding practices for 4 and 8 weeks. 23,30 A cross-sectional study conducted in the city of Rio de Janeiro (Brazil) revealed shorter exclusive breastfeeding duration in cases of severe physical IPV during pregnancy. 28 In Campinas (Brazil), domestic violence against pregnant women did not interfere with exclusive breastfeeding up to 40 days of life. 25
Two hypotheses were formulated to explain conflicting results for the association between violence against pregnant women and breastfeeding duration. 19,21,28,32 The deficit hypothesis considered that physiological and emotional problems caused by violence would lead to breastfeeding difficulties. 19,21,28,32 Chronic stressful violence might reduce prolactin and/or oxytocin secretion by the hypothalamic/pituitary/adrenal axis and the activation of central and peripheral sympathomimetic areas with lower milk production and/or letdown. 28,33,35 The compensation hypothesis suggests that women exposed to violence would be more sensitive to the needs of their infants and would view breastfeeding as a way to protect them, to improve their own self-esteem, and to detach themselves from episodes of violence. 19,21,32,36
Accordingly, this study formulated the following hypotheses: recurrent violence, violence with complications, and IPV against pregnant women increase the risk of mothers not breastfeeding their infants exclusively for 6 months and of interrupting breastfeeding before their infants are 12 months old. Thus, the goal was to assess whether violence before and during pregnancy, recurrent psychological/physical/sexual violence, violence with complications, and IPV against pregnant women are associated with exclusive breastfeeding duration shorter than 6 months and a breastfeeding period shorter than 12 months. Since prevalence of violence against pregnant women is very high in Brazil, 25,37,38 close to 50% for violence caused by multiple perpetrators, 37 our power to detect a statistically significant association, in case it exists, was high.
Materials and Methods
This prospective cohort study used data from the prenatal component of Brazilian Ribeirão Preto and São Luís Birth Cohort Studies (BRISA in the Portuguese acronym) conducted for the city of São Luís, state capital of Maranhão (Brazil). The BRISA prenatal cohort investigated etiologic factors for preterm birth. Data were collected in the prenatal period, at birth, and at 12–36 months of age. The goals and methods of the BRISA prenatal cohort study were described by Silva et al. 40 Institutional Review Board approval was obtained from the Research Ethics Committee of the Teaching Hospital of the Universidade Federal do Maranhão.
São Luís, the capital of the state of Maranhão, is situated in the Brazilian Northeast. In 2010, year in which the data were initially collected, São Luís had 1,014,837 inhabitants, an average income per capita of R$ 805.36 (∼446 US dollars), a municipal Human Development Index of 0.768, and a Gini Index of 0.61, and its infant mortality rate was 18.10 per thousand. 41 São Luís occupied the 12th position among Brazilian capital cities regarding female homicide rates (6.3 in every 100,000 women). 42
Sampling and data collection
In the São Luís BRISA prenatal cohort, a convenience sample was used because it was not possible to obtain a random sample that was representative of the population of pregnant women in São Luís. Sample size was calculated using a 5% significance level and an 80% power for detection of hazard ratios (HRs) of at least 0.80, and 49.6% 37 rate of women exposed to some sort of violence, totaling 631 women. 43 A 20% rate was added to the sample size to compensate for occasional losses to follow-up and to increase the power of the study, thus totaling 758 women.
The data were collected from 2010 to 2013, in three stages: (1) in the prenatal period (from February 2010 to June 2011), from 20 to 25 weeks of gestational age; (2) at maternity wards (from May 2010 to November 2011); and (3) when infants/children were 12–36 months old (from April 2011 to March 2013).
Pregnant women were recruited from public and private prenatal services and from ultrasound clinics. The inclusion criteria were: (1) having a single gestation at less than 20 weeks; (2) having performed an obstetric ultrasonography before 20 weeks gestation; and (3) intending to give birth in one of the maternity hospitals in São Luís. For those who met the inclusion criteria and agreed to participate, data collection during the prenatal phase was scheduled for when gestation was 20–25 weeks. At this time, 1447 pregnant women were interviewed at the Clinical Research Center (CEPEC) of the Federal University of Maranhão (UFMA). In the second phase of data collection, interviewers visited maternity wards with more than 100 deliveries per year daily to conduct an interview on childbirth. One thousand three hundred eighty-two puerperal women were interviewed, and their newborns examined. At this time, there were 65 losses due to refusal or early discharge. In the third phase of collection, when children were 12–36 months old, data were obtained from 1,151 mothers/children at the Maternal and Child University Hospital.
Four instruments were used for data collection: (1) two at the prenatal interview (Prenatal Interview Questionnaire, applied by female interviewers, and the Self-Applied Prenatal Questionnaire); (2) one at birth, the Birth Questionnaire—Mother, applied by interviewers; and one in the third phase of data collection, the 1st Year Questionnaire—Interview, applied by interviewers.
Theoretical model and variables
The theoretical model (Fig. 1), depicted as a directed acyclic graph (DAG), shows the interrelationships between the exposure variable violence against pregnant women, the confounding variables, and the outcome variable breastfeeding (measured by the variables exclusive breastfeeding up to the 6th month of life and breastfeeding up to the age of 12 months). Violence against pregnant women was investigated in terms of recurrence, severity, and who the perpetrator of violence is. Recurrent violence was investigated with the following variables: (1) violence 12 months before pregnancy and maintained during pregnancy; (2) psychological/physical/sexual violence during pregnancy; (3) exclusive psychological violence during pregnancy; (4) physical violence during pregnancy; and (5) physical/sexual violence during pregnancy. Severity was measured with the variable violence with pregnancy complications.
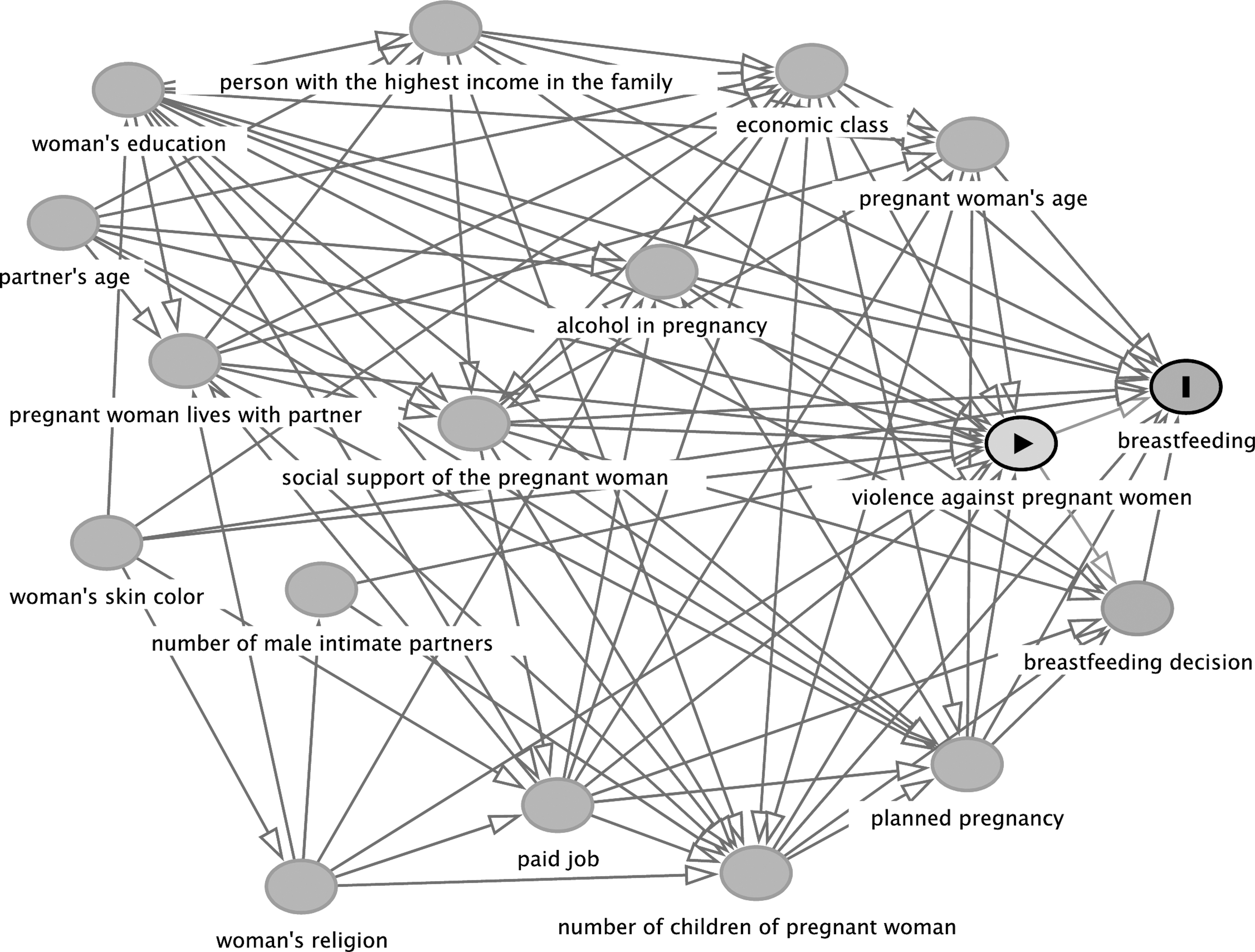
Directed acyclic graph with the exposure violence against pregnant women (measured by the variables violence 12 months before pregnancy and maintained during pregnancy, psychological/physical/sexual violence during pregnancy, exclusive psychological violence during pregnancy, physical violence during pregnancy, physical/sexual violence during pregnancy, violence with pregnancy complications and intimate partner violence), the outcome of breastfeeding (ascertained by the variables exclusive breastfeeding for 6 months and breastfeeding for 12 months), and confounding variables.
Violence was assessed through 13 questions from the World Health Organization's Violence Against Women (WHO VAW) questionnaire. These questions were part of the Self-Applied Prenatal Questionnaire. The Brazilian Portuguese version 44 of this questionnaire was validated by two studies, 45,46 including this population of pregnant women. 46 It was answered by the women alone in a quiet room during the visit to the research center. A supervisor was available to clear up any doubt. All the women interviewed were given a leaflet with information on the definition and types of violence against them and the location and contacts of agencies from which they could seek help.
WHO VAW includes questions about psychological violence (insults, belittling, constant humiliation, intimidation, and threats), physical violence (slapping, pushing, shaking, punching, kicking, strangling, burning intentionally, and using weapons), and sexual violence (forced sexual intercourse and sexual humiliation). 44
Violence 12 months before pregnancy and maintained during pregnancy was categorized as no violence, violence only before pregnancy, and violence only in pregnancy and before/during pregnancy (recurrent). Psychological/physical/sexual violence during pregnancy, exclusive psychological violence during pregnancy, physical violence during pregnancy, and physical/sexual violence during pregnancy were categorized as no violence, one episode, and recurrent (if the answer was “once” for two or more questions or “few times” or “many times” for any question).
Violence with pregnancy complications was categorized as no violence, violence without complications, and violence with complications. The question about pregnancy complications included the following possible answers: vaginal bleeding, threatened abortion, threatened preterm labor, and other complications, the latter of which was an open-ended question.
IPV was categorized as no violence, violence inflicted by family members other than an intimate partner, and IPV.
The dependent variables, exclusive breastfeeding for 6 months and breastfeeding for 12 months, were expressed in months after childbirth. The cutoff point at 6 months for exclusive breastfeeding duration was based on the WHO recommendation that breastfeeding be carried out up to the age of 6 months. 1 The cutoff point of 12 months for exclusive breastfeeding duration was adopted because only 14 (1.23%) infants had reached this age, and thus breastfeeding at 24 months was not assessed. We considered the infant was being exclusively breastfed when he/she was fed breast milk only, without supplementation with any other type of food or liquid, except vitamins, oral rehydration salts, mineral supplements, and medications. Breastfeeding was defined based on whether the infant was fed breast milk and other foods and/or liquids. 2 Questions on breastfeeding were asked when the children were 12–36 months of age.
For construction of the exclusive breastfeeding for 6 months variable, we first applied question C6, “Until what age was your child exclusively breastfed? (the following explanation should be read out to the mother: exclusive breastfeeding consists only of breast milk, no teas, water, other types of milk, other beverages or foods),” and the direct answer was expressed in months. After that, we asked “When did you include these foods or beverages in the diet of your child?,” according to four subitems (1) C8 Milk (liquid or powder); (2) C9 Formula; (3) C10 Other liquids (teas, juices)?; and (4) C11 Semisolid or solid foods?. We considered the shortest time in months as the answer for the exclusive breastfeeding for 6 months variable.
For construction of the breastfeeding for 12 months variable, we compared the answers to three questions: (1) “C4 Was your child breastfed YESTERDAY?”; (2) “C5 If NOT, until what age was your child breastfed” and (3) “C7 Considering only the past three months, do you have the habit of putting your child to the breast after he/she has already fallen asleep?.” When the mother or legal guardian could not recall the breastfeeding time, but she had answered about exclusive breastfeeding time, we replaced breastfeeding time by exclusive breastfeeding time.
Self-reported skin color was obtained at childbirth and dichotomized into white or nonwhite. The pregnant woman's age was categorized into younger than 20 years (adolescent), 20–24 years (young adult), and 25 years or older (adult). Planned pregnancy was ascertained at childbirth by asking the women the following question: “was your pregnancy planned?” and was dichotomized into yes or no. Formal employment, and alcohol consumption during pregnancy were also dichotomized into yes or no. Maternal schooling was categorized as up to 8 years, 9–11 years, and 12 or more years. Number of children was categorized into three categories (no child, one child, and two or more children). The variable “person with the highest income in the household” was categorized into intimate partner, pregnant woman, and other. The variable marital status was represented in the models as “pregnant women lives with partner,” which was dichotomized into yes or no.
Social support was assessed using the 19 questions from the Medical Outcomes Study Social Support Survey (MOS-SS), 47 dichotomized into inappropriate and appropriate, and the third quartile was used as cutoff point. The variable economic class was based on the possession of goods (color television, radio, bathroom, automobile, washing machine, videocassette and/or DVD player, freezer, and refrigerator), having hired a full-time maid, and the schooling of the household member with the highest income. In 2010, from a score ranging from 0 to 46, economic class was divided into A (35–46), B (23–34), C (18–22), D (8–13), or E (0–7), in which category A represented the highest and the category E the lowest purchasing power. 48
Statistical analysis
All variables were assessed as categorical variables. The confounding variables, selected by the backdoor criterion in a DAG and collected in the prenatal period, were as follows: age, maternal schooling, formal employment, number of children, social support given to the pregnant woman, alcohol consumption during pregnancy, person with the highest income in the household, and economic class. Low birth weight/preterm birth was not included as a confounding variable because there is strong evidence to support that low birth weight and preterm birth are mediators, located on the causal pathway between violence during pregnancy and breastfeeding.
The analyses were performed using Stata/SE 15.1. The following survival analysis techniques were used for exclusive breastfeeding for 6 months and breastfeeding for 12 months: the Kaplan–Meier estimator, the log-rank test, and Cox's proportional hazards regression model, which included the HR. The outcome variable was time in months to exclusive or any breastfeeding.
The two-sided log-rank test was used to verify whether breastfeeding duration differed statistically (p-value <0.05) among the strata of each type of violence assessed.
Survival time was determined based on the date of birth of each child—up to 6 months for exclusive breastfeeding for 6 months and 12 months for breastfeeding for 12 months. We considered a failure in exclusive breastfeeding for 6 months when a food or liquid other than breast milk was introduced before the 6th month of life and failure in breastfeeding for 12 months when the infant was no longer breastfed before the age of 12 months.
There were no left-censored data because all infants were included in the study according to their dates of birth. Sixteen observations were right censored because the mothers did not remember timing of breastfeeding, but they did remember timing of exclusive breastfeeding. Proportional hazards assumption was verified with the estat phtest command in Stata Stata/SE 15.1 and was not violated in any of the models.
Ethics
The BRISA São Luís prenatal cohort study was approved by the Research Ethics Committee of the Teaching Hospital of Universidade Federal do Maranhão (process no. 4771/2008-30). All mothers or guardians signed an Informed Consent Form.
Results
In this study, a pregnant woman was excluded from the prenatal assessment because she did not answer the questions about violence; thus, there were 1,446 observations. After excluding 295 losses to follow-up and two missing values in breastfeeding questions, the exclusive breastfeeding for 6 months final sample comprised 1,148 mothers and infants. The final sample for the breastfeeding for 12-month sample was 1,127, because 21 mothers did not remember timing of breastfeeding.
Most women reported having nonwhite skin color (84%). Their ages ranged from 14 to 44 years, with a median of 25 years. Approximately 79% of them lived with their husbands/partners, 76% had 9–11 years of schooling, 68% belonged to socioeconomic class C, 49.6% had formal employment, 20.3% were self-employed, 20.4% were unskilled manual workers, and 26.8% were wage earners/employees. Husbands/partners were the persons with the highest income in only 31.3% of the households. Approximately 34% of the mothers had planned pregnancy, 58% were primiparous, 22% had received appropriate social support, and 27% had drunk some kind of alcoholic beverage during pregnancy. Infants' ages in the second follow-up assessment ranged from 12 to 32 months, with a median of 16 months.
The rates obtained for psychological, physical, and sexual violence during pregnancy were, respectively, 47.5% (recurrent in 35.7%), 12.1% (recurrent in 5.6%), and 2.8% (recurrent in 1.8%).
Kaplan–Meier curves and the log-rank test (p-value > 0.05) indicated similar exclusive breastfeeding duration up to the 6th month of life, regardless of recurrence, complications, or who its perpetrator was, a family member or an intimate partner (Figs. 2A, 3A, C, 4A, C, and 5A, C). Cox regression did not reveal differences in breastfeeding duration between women who experienced some violence and those who did not (Table 1).
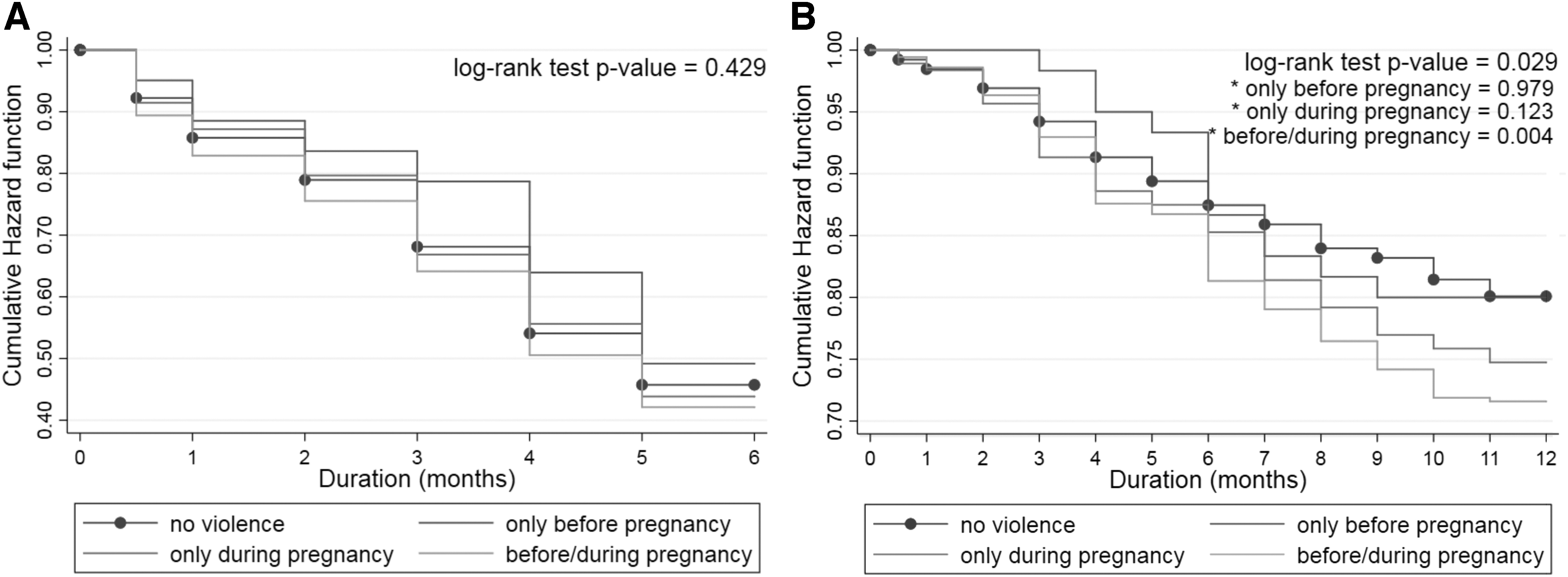
Violence 12 months before pregnancy and maintained during pregnancy.
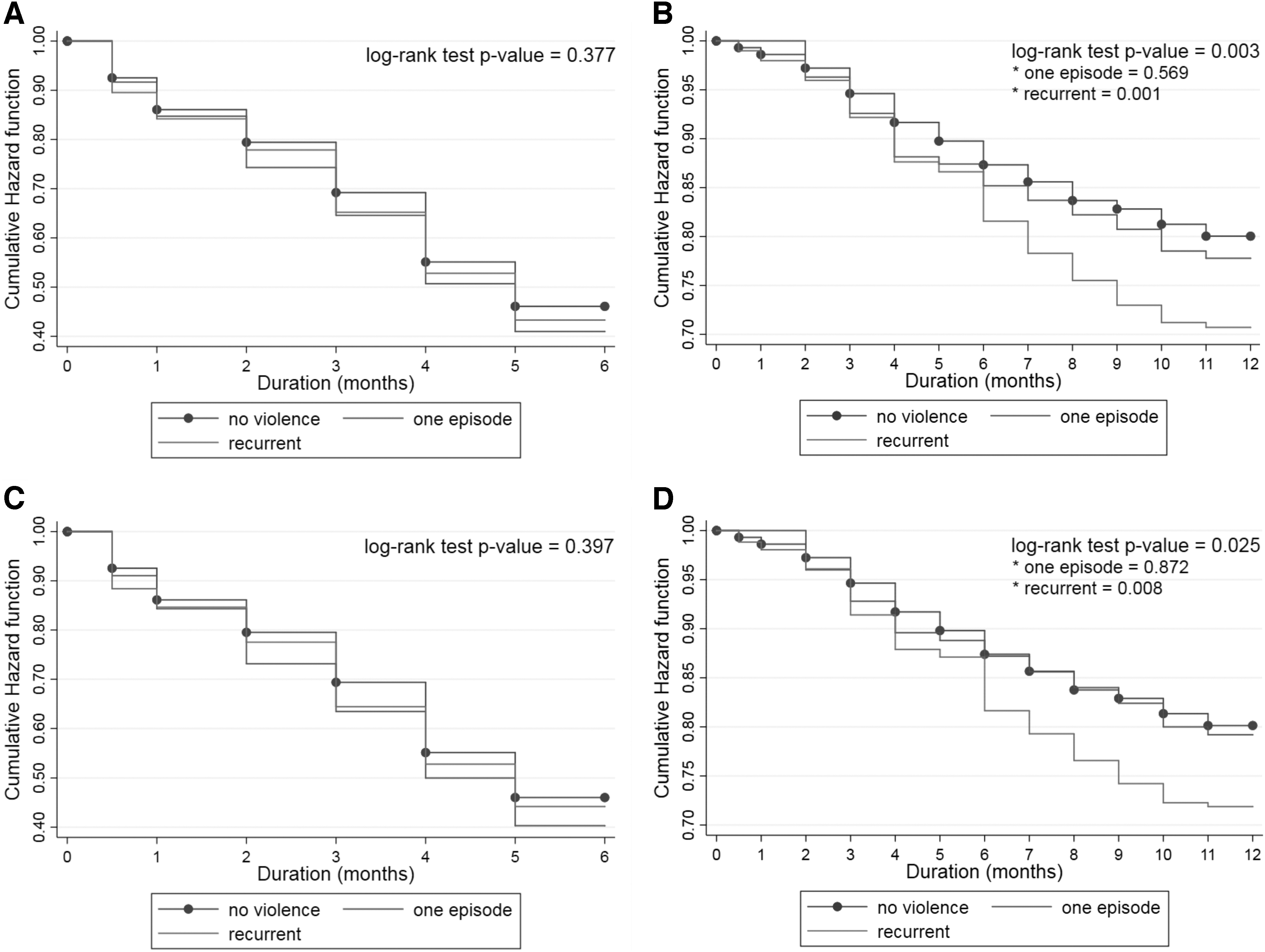
Violence during pregnancy and breastfeeding duration.
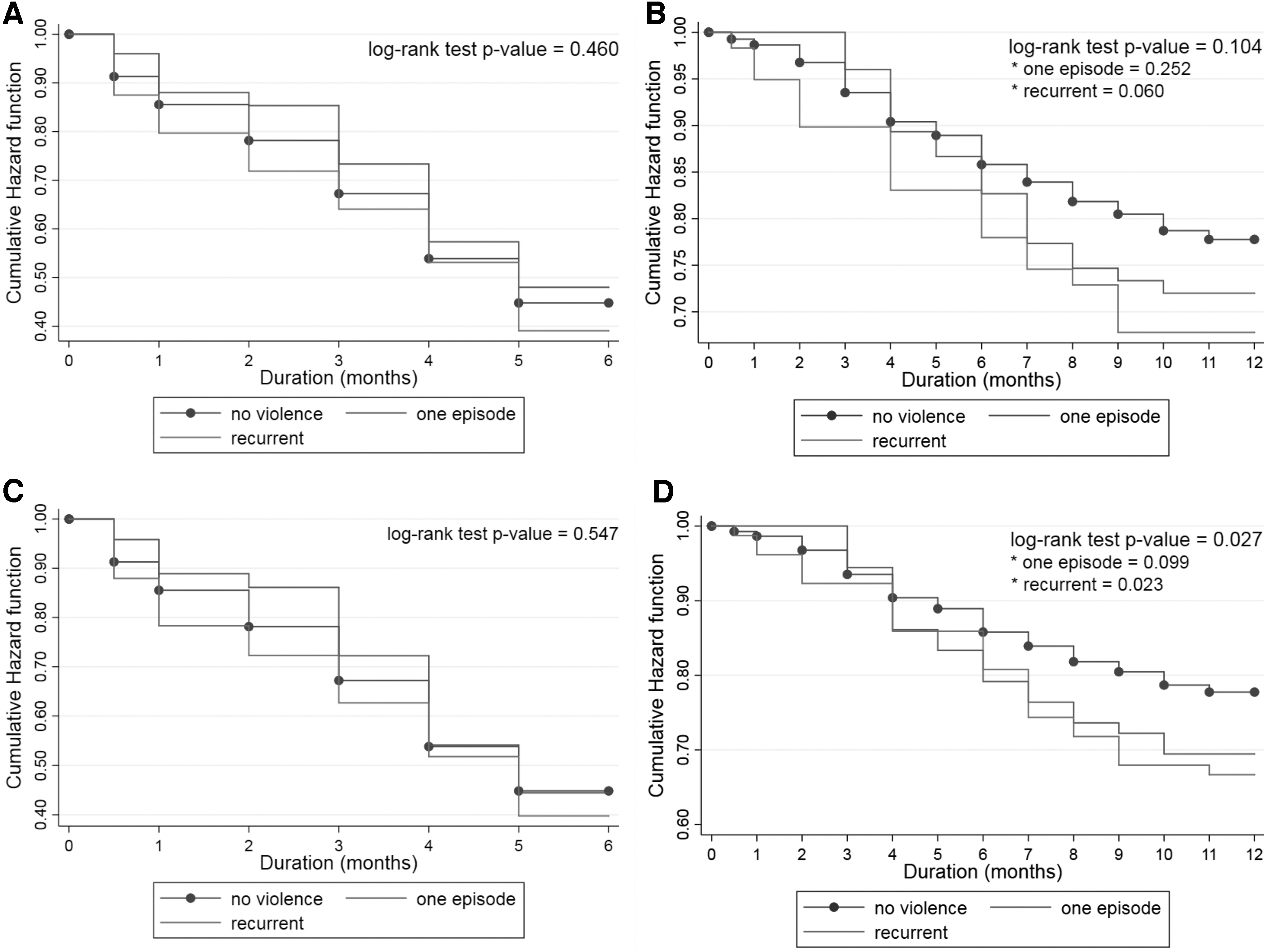
Physical and sexual violence during pregnancy and breastfeeding duration.

Violence with pregnancy complications and intimate partner violence during pregnancy and breastfeeding duration.
Descriptive Analysis and Estimates Obtained from Cox Regression for Recurrent Violence, Violence with Complications, and Intimate Partner Violence Against Pregnant Women and Breastfeeding Duration, São Luís Brisa Prenatal Cohort Study, Brazil, 2010–2011
Final sample = 1,148.
Final sample = 1,127.
Survival function at 6 months.
Survival function at 12 months.
CI, confidence interval; HR, hazard ratio.
Kaplan–Meier curves and the log-rank test showed different probability of breastfeeding continuing up to 12 months of age according to the presence or absence of violence against pregnant women (Figs. 2B, 3B, D, 4B, D, and 5B, D), except for physical violence during pregnancy (p = 0.104). These differences were observed after the 6th month of life. In adjusted analyses using Cox regression, the risk of a child not being breastfed up to 12 months of life was higher for violence that occurred before/during pregnancy (95% confidence interval [CI] = 1.03–1.88), recurrent psychological/physical/sexual violence during pregnancy (95% CI = 1.11–1.92), recurrent psychological violence (95% CI = 1.05–1.96), and recurrent physical/sexual violence during pregnancy (95% CI = 1.01–2.39). Violence with pregnancy complications (95% CI = 0.94–2.22) was not associated with breastfeeding for 12 months. There were no differences in breastfeeding duration according to who perpetrated the violence (a family members or an intimate partner) (Table 1). Proportional hazards assumption was not violated in any of the models.
Discussion
In the BRISA São Luís prenatal cohort study, contrary to our hypothesis, we did not observe differences in exclusive breastfeeding duration in mothers exposed or not to any kind of violence. However, the risk of breastfeeding cessation before 12 months of life was higher in cases of recurrent violence (assessed by violence before/during pregnancy, recurrent psychological/physical/sexual violence during pregnancy, recurrent psychological violence during pregnancy, and recurrent physical/sexual violence during pregnancy). No difference in risk was found according to who perpetrated the violence (a family members or an intimate partner).
The lack of association of recurrent violence, violence with pregnancy complications, and IPV with exclusive breastfeeding duration may be explained by two hypotheses. According to the compensatory hypothesis, some women may have developed the ability to overcome the trauma of violence and as a consequence may have been able to breastfeed exclusively until their infants have reached 6 months of age. 19,21,32,36,49,50 In the second hypothesis, episodes of violence may have decreased or ceased for some pregnant women as pregnancy approaches its end and childbirth becomes imminent. 39,51,52 This decrease may be explained because women separate from their violent partners 51 or develop strategies to avoid confrontation with their agressors, 52 or because some offenders may fear the social consequences of their violence. 52
In Brazil, a qualitative study described the significance of maternal care experience, especially breastfeeding, for 11 women who suffered marital violence. In general, women sought to isolate the child from the environment of violence and provide adequate care to recognize themselves in the role of “good mother” (emphasis of the authors). Breastfeeding and feeding the child well was one of the manifestations of taking good care of the baby and having good experiences, despite the suffering of violence. 50
Our findings for exclusive breastfeeding for 6 months are at odds with those of two studies mentioned in this article. 21,28 In a cohort study undertaken in Kilimanjaro (Tanzania), researchers observed twice as high a risk for early cessation of exclusive breastfeeding in the concomitant presence of psychological, physical, and sexual violence perpetrated by intimate partners. 21 In the city of Rio de Janeiro (Brazil), exclusive breastfeeding duration was shorter in the presence of severe physical IPV during pregnancy. This finding was not sustained when variables related to child health, use of health services in the prenatal period, and maternal self-esteem were added to the model. 28 However, a cross-sectional study with Swedish women 24 and a cohort study with adolescent and young adult U.S. women 27 did not detect differences in exclusive breastfeeding duration in the presence or absence of domestic violence 24 and IPV during pregnancy. 27
Regarding breastfeeding up to the age of 12 months in the BRISA São Luís prenatal cohort study, violence before/during pregnancy, recurrent psychological/physical/sexual violence during pregnancy, recurrent psychological violence during pregnancy, and recurrent physical/sexual violence during pregnancy increased the risk of breastfeeding cessation within the first year of life. When compared to those mothers who did not report violence, the risk of not breastfeeding their infants until they were 12 months old was 39% higher when violence occurred before pregnancy and persisted during pregnancy; 46% higher for recurrent violence during pregnancy; 44% higher for recurrent psychological violence only during pregnancy; and 55% higher for recurrent physical/sexual violence during pregnancy.
A possible explanation for the association between some forms of recurrent violence with breastfeeding shorter than 12 months is that violence may have increased after childbirth due to new conflicts with intimate partners and with other family members. 39,52 The women's incapacity to follow gender-related social rules (such as caring for the home and family and meeting the sexual expectations of their partners) can generate or aggravate existing conflicts and produce or aggravate violence against women. 51,52 It is possible that small sample sizes prevented us to detect associations between recurrent physical violence and violence with complications with breastfeeding for 12 months.
IPV did not increase the risk of exclusive breastfeeding and breastfeeding cessation. When compared to other family members, intimate partners were more frequently the perpetrators of violence against pregnant women. IPV might have decreased or ceased as a result of relationship breakups 51 or because pregnant women may have been protected 53 from IPV by living with other family members in over 50% of the cases.
Limitations of this study include lack of representativeness of the population of São Luís, assessment of violence during 22–25 weeks' gestation, and collection of breastfeeding data when the infant was 12–30 months old. Even though the sample was not a probabilistic one and its results cannot be extrapolated to the city of São Luís, the minimum number necessary to assess associations between types of violence and breastfeeding duration was attained. Regarding the WHO VAW instrument, it should be preferably applied at the end of pregnancy. However, this was not possible because the goal of the BRISA cohort study was to evaluate risk factors for preterm labor and because data collection took place from 22 to 25 weeks of gestational age. As for the ages of the infants at the time of data collection, two studies have shown that maternal information on breastfeeding duration was valid and reliable for a period shorter than or equal to 3 years. 54,55 Moreover, asking more than one question to determine exclusive breastfeeding for 6 months and breastfeeding for 12 months outcomes might have reduced measurement bias. 54 Some confounding factors (e.g., resilience) were not ascertained and thus could not be controlled for.
The strengths of this study include the following: (1) it is a cohort study, in which exposure to violence against pregnant women was assessed before breastfeeding had begun; (2) use of a validated instrument to measure violence against pregnant women; (3) assessment of different types of violence against pregnant women, specifying the effects of recurrence, severity, and perpetrator; (4) investigation into breastfeeding at 12 months, which is uncommon in studies on breastfeeding; and (5) survival analysis for determining the risk of breastfeeding cessation due to violence against pregnant women.
Conclusions
In the BRISA São Luís prenatal cohort study, violence against pregnant women did not interfere with exclusive breastfeeding up to the 6th month of life. However, mothers who experienced recurrent violence were at greater risk of breastfeeding cessation up to the end of the infant's first year of life. These findings suggest that professionals in charge of prenatal care and child health care in the first year of life should investigate the presence of domestic/family violence on a routine basis, especially when breastfeeding difficulties arise.
Footnotes
Acknowledgments
The authors wish to thank the women who kindly agreed to participate in the prenatal BRISA investigation, as well as the interviewers.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Project was funded by CNPq (Brazilian National Research Council) grant numbers 471923/2011-7 and 561058/2010-5, FAPESP (São Paulo State Research Foundation) grant number 2008-53593-0 and FAPEMA (Maranhão State Research Foundation grant numbers 0035/2008, 00356/11 and 01362-11.