
Abstract
Background:
Sex and gender, two important factors affecting health care, should be routinely taken into consideration in clinical practice. Members of the Sex and Gender Health Collaborative Scholarship Committee reviewed clinical guidelines published by the American College of Cardiology (ACC) from 2008 to 2018 to determine if the number of women authors on the writing committee influenced the presence of sex- and gender-specific content and recommendations in each guideline.
Methods:
We reviewed 33 ACC clinical guidelines from 2008 to 2018 and determined the number of women authors on the writing committee for each guideline. We then reviewed each guideline to identify specific content on sex and/or gender differences as it pertained to the guideline's subject cardiac condition.
Results:
The median proportion of women authors among the 33 ACC guidelines was 22.2% (interquartile range 4.4–81.1). Only two guidelines (6%) had writing committees with >50% women authors. Overall, 25 of 33 guidelines (75.8%) contained sex and gender content; however, the depth and detail of the sex and gender content varied widely among guidelines. The proportion of women authors was not associated with the presence of sex- and gender-specific content.
Conclusions:
Our findings demonstrate continued gender disparities in authorship, and changes should be made to increase the inclusion of women in clinical practice guideline writing committees. We propose selecting a sex and gender champion for guideline writing committees and/or including a specific section on sex- and gender-related content in each guideline to ensure inclusion of sex- and gender-specific recommendations in clinical guidelines.
Introduction
According to the National Institutes of Health (NIH) Office on Women's Health Research, 1 increasing numbers of women have been included in research studies, and women now account for half of all participants in NIH-supported clinical research. 2 This increased inclusion of women participants in research has led to an increased amount of information regarding sex and gender, which ultimately improves the health care of women. 3,4
Precision medicine—medical care that takes variability in genes, environment, and lifestyle into account for each person—calls for the inclusion of genetic information and the assessment of social determinants of health. Two important factors affecting health care are sex, a genetic variant that divides all humans into two distinct populations with some variants, and gender, social roles leading to differing social determinants of health for females and males. Sex and gender, however, are not routinely taken into consideration in clinical practice. 5,6
When translating research into clinical practice, clinical practice guidelines (CPGs) often serve to establish standards of clinical care. While CPGs can often guide changes in clinical practice, they frequently result in a one-size-fits-all set of recommendations. Several articles suggest methods to address sex and gender in CPGs. 7 –9 One option is to increase the number of women authors: Nielsen et al. 10 reviewed over one and a half million published research articles and found a positive correlation between women authorship and the inclusion of sex and gender analysis. While Nielsen et al. did not specifically focus on CPGs, Merman et al. evaluated the representation of women on CPGs across multiple medical specialties and suggested efforts to improve the representation of women authors on CPGs, including publication of methods used to select authors and reporting metrics of women's representation. 11 Sardar et al. reviewed the representation of women in American College of Cardiology (ACC)/American Heart Association (AHA) Guideline Writing Committees and highlighted the importance of including women authors in cardiology guidelines. Specifically, the authors emphasized that including more women authors has the potential to help identify knowledge gaps pertaining to sex- or gender-specific data, diversify the perspective of the writing group, and increase attention to the need for recommendations specific to women. 12 Other authors have suggested different approaches to increase sex and gender content in CPGs. For example, Tannenbaum et al. suggest including a sex/gender champion on all guideline writing committees. 6
According to Wenger, 9 the 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease fails to include sex and gender considerations. As there are known differences between men and women in the epidemiology, presentation, rates of diagnosis, and management of heart disease, we sought to review the ACC CPGs over the last 10 years (2008–2018) for inclusion of sex and gender content. Specifically, we examined the presence of sex- and gender-specific recommendations in prevention, presentation, diagnosis, and treatment beyond pregnancy and lactation and the number of women authors on the writing committee of each guideline. Our objectives were to determine (1) if a greater proportion of women authors on ACC CPG writing committees increased the likelihood that sex- and gender-related content would be included in their CPGs; (2) if the proportion of women authors and/or the inclusion of sex- and gender-specific content increased over time; and (3) if the inclusion of a discussion of the reasons for which sex and gender content was excluded increased over time.
Methods
Authors of this article are members of the Sex and Gender Health Collaborative (SGHC) Scholarship Committee. The SGHC exists within the American Medical Women's Association and was created to foster a sex and gender approach to education and clinical practice. The scholarship committee is made up of 10 women health care providers and/or researchers (8 physicians, 1 pharmacist, and 1 PhD researcher) whose goal is to further scholarship in this area.
Five members of the SGHC Scholarship Committee and one statistician participated as authors on this article. Before undertaking this review, the scholarship committee met several times and outlined the process for review. Our authors include physicians in the fields of emergency medicine (T.E.M.) and internal medicine (M.R., I.T., J.T.) and have expertise in managing patients with cardiovascular disease. In addition, all SGHC Scholarship Committee authors are national content experts in sex- and gender-based medicine and have all participated actively in continuing medical education on the importance of sex and gender content in medical education and CPGs. For the purpose of this study, authors determined the presence of sex and gender content within a guideline and also reviewed if CPG writing committees provided an explanation as to why sex and gender content may or may not have been excluded.
Inclusion/exclusion criteria
The Scholarship Committee selected the ACC CPGs published from 2008 to 2018 for review (Table 1). We specifically reviewed the ACC guidelines given the breadth of known clinical differences in cardiac disorders between women and men. A total of 39 guidelines were released during this 10-year period. Six of the 39 guidelines were excluded from our review, as they were nonclinical in nature. The six nonclinical guidelines which were excluded are the 2017 CPG Implementation Strategies, 2015 CPG Recommendation Classification System, 2014 CPGs, the Evolution and Future: A 30-Year Journey, 2014 Cost/Value Methodology in Guidelines and Performance Measures, 2012 Guideline Methodology Summit Report, and 2010 Methodology Manual and Policies and are listed in Figure 1.
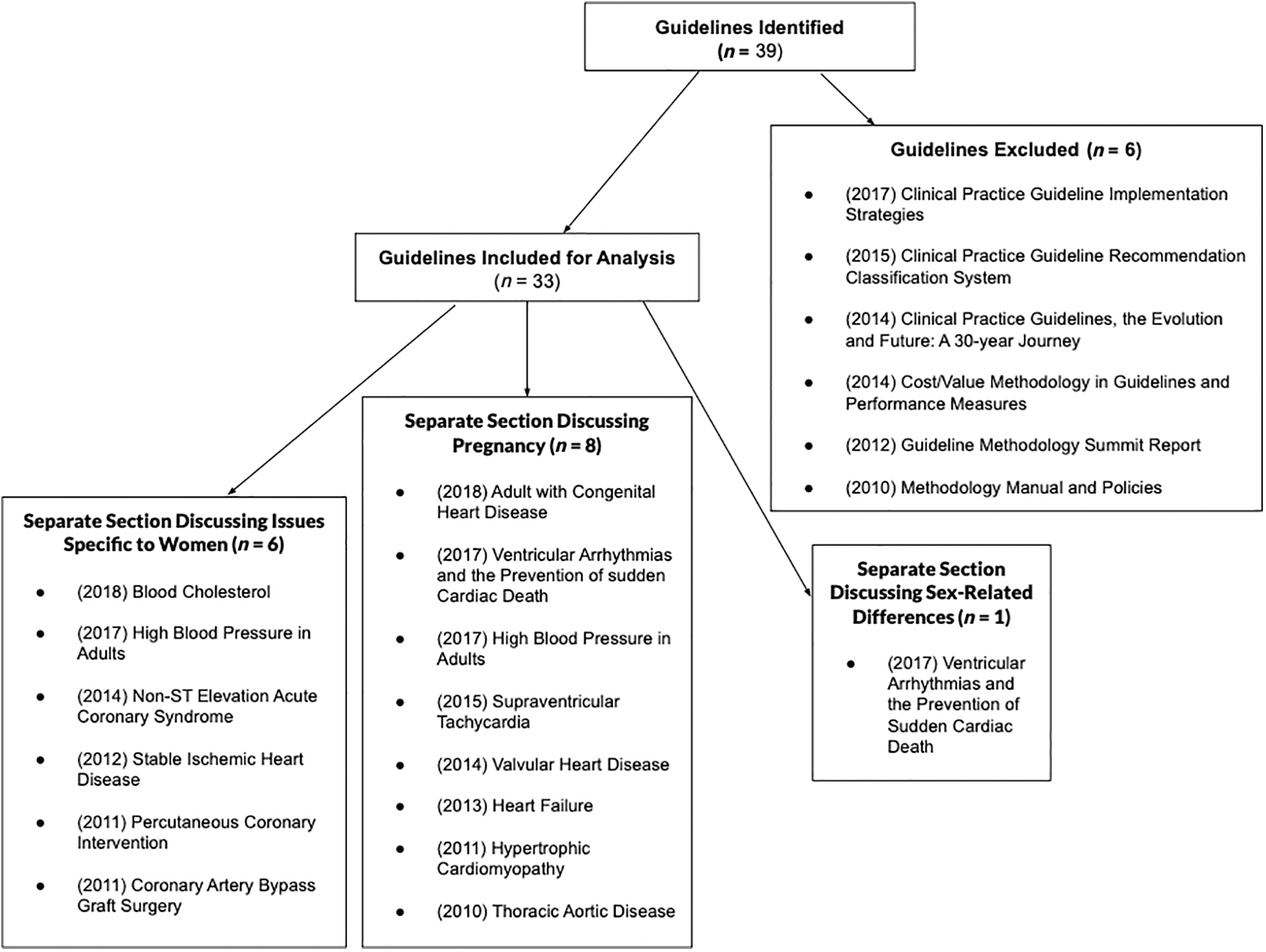
Inclusion and exclusion of clinical practice guidelines.
American College of Cardiology Guidelines from 2008 to 2018
Each guideline was assigned two reviewers. Each committee member was randomly assigned six to seven guidelines for review. After the first round of reviews, committee members were assigned an additional six to seven different guidelines for review, such that two different members within the SGHC Scholarship Committee independently reviewed each guideline. Before statistical analysis, the two reviewers for each guideline addressed any discrepancies in their review and came to consensus.
Data collection
We determined the total number of authors on the writing committee for each guideline and then determined the number of women authors on that committee. Appointments to the ACC CPG Committees are made annually for open committee seats by the ACC Nominating Committee. The committee selects the best candidates from nominated/self-nominated applications based on committee needs, demographics, and competencies. 46 Term lengths range from one to three years, and committee members are eligible to serve on a committee for six consecutive years. 47
To determine the gender of a given author, we performed an internet search on each author and categorized authors as women or men from the use of pronouns in any publications by and/or about a given author (he/his/his or she/her/hers) or phenotypically from a photograph. There were no issues determining the gender of each author. We then reviewed each guideline to look for the specific discussion of sex and/or gender differences as it pertained to the guideline's subject cardiac condition. When sex- and/or gender-specific content was present, we determined if the content was solely focused on pregnancy and/or lactation or if the content contained information pertaining to differences between men and women in terms of prevention, screening, clinical presentation, diagnosis, treatment, and outcomes of the subject cardiac condition. We also took note of whether the reasons for not including sex- and gender-specific content were incorporated into recommendations in the guidelines. Data were collected to indicate the presence or absence of sex and gender content. Two reviewers independently reviewed each guideline to minimize any inaccuracies due to human error and to avoid potential reviewer bias, although reviewer bias was not anticipated to be an issue given the inherent objective nature of our review criteria. Before statistical analysis, the two reviewers assigned to a given guideline discussed and addressed any discrepancies in their data review. See Table 2 for a complete list of content review for each guideline. In addition, one author (I.T.) reviewed all guidelines to identify a separate section within the guideline, which specifically addressed issues pertaining to women, pregnancy, and/or sex-related differences (Table 1).
Association Between Proportion of Women Authors and Presence of Sex and Gender Content. p-Value Determined Based on Mann–Whitney U tests
IQR, interquartile range.
Statistical analyses
Descriptive statistics was used to report the median proportion of women authors on guidelines, as well as the proportion of CPGs that contained any content on sex and gender, specific content on pregnancy, and specific content on lactation. Medians were used for comparisons due to non-normally distributed data. To determine whether the proportion of women authors was associated with the presence of sex and gender content, median (interquartile range [IQR]) proportion of women authors was compared between guidelines with and without sex and gender content. The Mann–Whitney U test and Kruskal–Wallis test were used to determine statistical significance. Finally, the median proportion of women authors in the first 5 years (2008–2013) of our review period was compared to that of the latter 5 years (2014–2019) and then stratified by presence of sex and gender content. Sensitivity analyses were performed excluding the 2011 Cardiovascular Disease Prevention in Women 19 article due to a concern that this particular guideline, which was written primarily for women, may bias the study results. Statistical significance was assessed at the 0.05 level. All statistical analyses were done using R statistical software.
Results
Thirty-three articles published between 2008 and 2018 met inclusion criteria and were reviewed for analysis (Table 1). For the 33 guidelines included in the first analysis, the median proportion of women authors was 22.2% (IQR 4.4–81.1) (Table 2 and Fig. 2a). Only two of the 33 (6%) guidelines had writing committees consisting of >50% women authors.
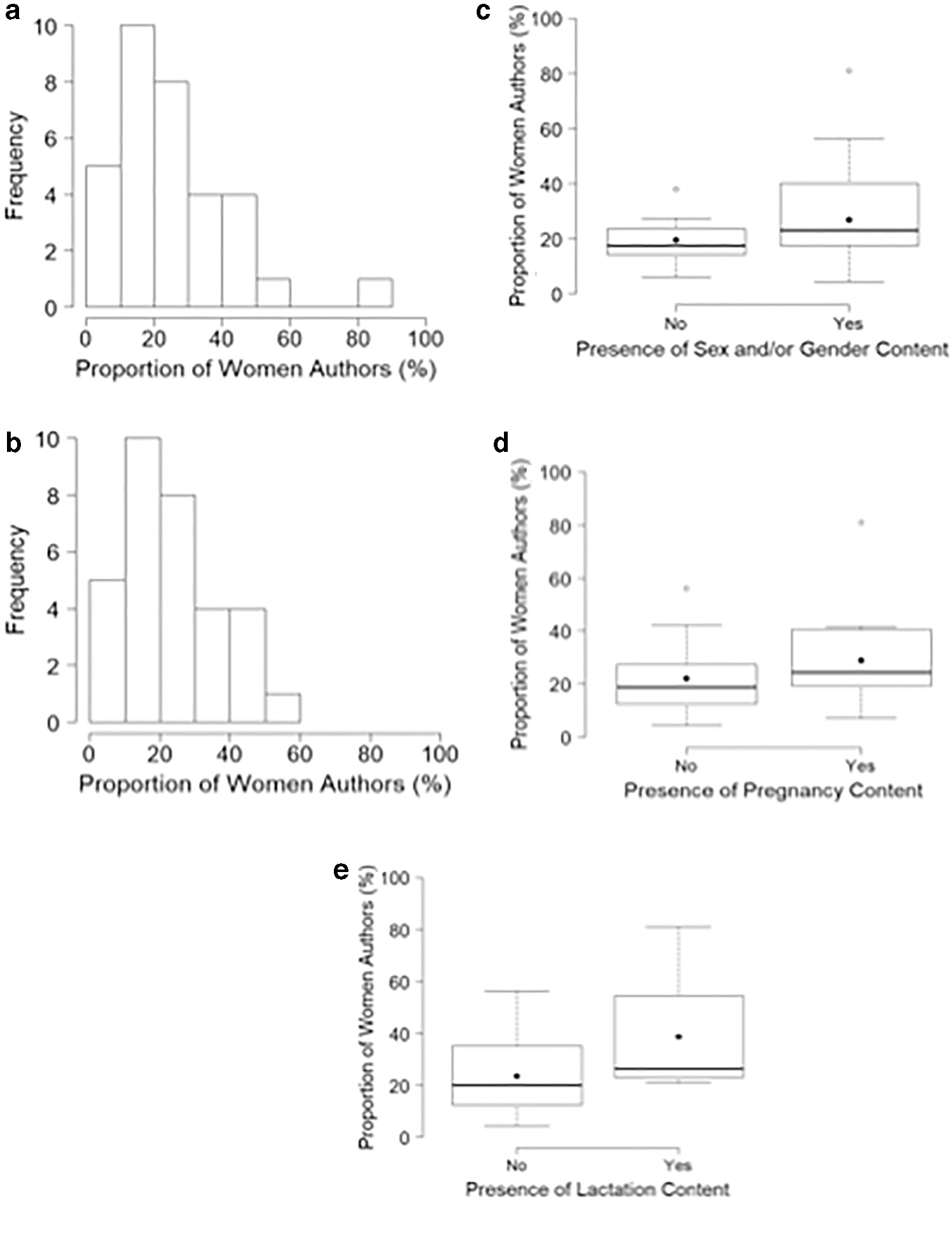
Of the 33 guidelines, 25 (75.8%) had the presence of any sex- and/or gender-based content in the guideline, 16 (48.0%) had content specifically related to pregnancy, and 4 (12.0%) had content specifically related to lactation. Eleven guidelines did not address sex and/or gender differences, but only two guidelines stated why. For example, in the 2011 guideline on extracranial carotid and vertebral artery disease, 20 the authors explained that data on women were an existing gap in evidence.
Next, we evaluated whether the presence of sex and gender content was associated with the proportion of women authors (Table 2 and Fig. 2c–e). Comparing between guidelines with and without general sex and gender content, between guidelines with and without pregnancy-related content, and between guidelines with and without lactation-related content, there were no statistically significant differences in the median proportion of women authors (Table 2 and Fig. 2c–e). Similarly, there were no statistically significant differences in the median proportion of women authors between guidelines that did and did not address sex and gender differences or between guidelines that did and did not explain why sex and gender differences were not addressed (Table 2). However, the absolute differences in median proportion of women authors were greatest between guidelines that did and did not have pregnancy-related content (24.4% vs. 18.8%, respectively), between those that did and did not have lactation-related content (26.4% vs. 20.0%, respectively), and those that did and did not explain why sex and gender differences were not addressed (30.4% vs. 23.1%, respectively) (Table 2).
Finally, we compared the proportion of women authors between two study periods: 2008–2013 and 2014–2018. There were 14 guidelines published in the 2008–2013 study period and 19 guidelines published in the 2014–2018 period (Table 1). Overall, the median proportion of women authors was 20.0% in the first study period compared with 23.4% in the second study period, but this increase was not statistically significant (p = 0.59) (Table 3). When data were stratified by presence of sex and gender content, the difference in the proportion of women authors on guidelines during the 2008–2013 versus the 2014–2018 study periods was not statistically significant (Table 4 and Fig. 3a). When data were stratified by presence of a discussion as to why sex and gender differences were not addressed, the difference in the proportion of women authors on guidelines during the 2008–2013 versus the 2014–2018 study periods was also not statistically significant (Table 4 and Fig. 3b).

Median (Interquartile Range) Proportion of Women Authors by Study Period
Median (Interquartile Range) Proportion of Women Authors in Each Study Period Stratified by Presence of Sex and Gender Content
As the 2011 guideline on Cardiovascular Disease Prevention in Women 19 had a disproportionate number of women authors compared to the remaining 32 guidelines (81.1% compared to a range of 4.4%–56.3%), a sensitivity analysis was performed excluding this guideline. Statistically, there was no difference in the outcome analysis. For the 32 guidelines included in the second analysis, the median proportion of women authors was 21.6% (4.4%–56.3%) (Fig. 2b) compared to 22.2% (4.4%–81.1%) in the initial analysis. Only one of the 32 (3%) guidelines had a writing committee consisting of >50% women authors. There were no statistically significant differences among median proportion of women authors with respect to sex- and/or gender-based, pregnancy-related, or lactation-related content among the guidelines. The proportion of women authors also did not differ statistically between guidelines that did or did not address sex- and/or gender-based differences. Finally, there were no statistically significant differences between median proportion of women authors when comparing the earlier and later study periods (2008–2013 vs. 2014–2018) nor were there statistically significant differences in median proportion of women authors when data were stratified by presence of sex and gender content or when data were stratified by presence of a discussion as to why sex and gender differences were not addressed (data not shown).
Among the ACC guidelines, there were notable variations in the amount of sex- and gender-based content in each guideline. While some guidelines only briefly mentioned sex and gender differences, other guidelines provided more in-depth sex- and gender-based content. For example, the 2018 Guideline on Blood Cholesterol 43 included an entire section on women as a specific population, whereas the 2013 guideline on ST-elevation myocardial infarction did not discuss sex differences in detail. 22 In addition, some guidelines only addressed issues related to pregnancy and did not address differences that may pertain to nonpregnant women, such as in the 2014 guideline on valvular heart disease. 32 Six guidelines included a separate section within the guideline discussing issues specific to women, 16,17,21,28,38,43 and eight guidelines included a separate section discussing issues specific to pregnancy (Table 1). 14,15,26,32,35,38,39,45 Only one guideline included a separate section discussing sex-related differences. 45 Moreover, some guidelines even suggested a separate guideline specific to women. 26,43 We performed an analysis comparing the median proportion of women authors of guidelines which included a separate section specific to women, pregnancy, or sex-related differences to those that did not include a separate section, and there was no statistically significant difference in the median proportion of women authors (data not shown).
Discussion
The increased inclusion of women as research participants has led to increased available information about the influence of sex and gender on medical disorders. Sex and gender, however, are not routinely taken into consideration in clinical practice and are not often addressed in CPGs. 9,12 As there are known differences between men and women in the epidemiology, presentation, rates of diagnosis, and management of heart disease, we reviewed the 33 ACC CPGs which were published from 2008 to 2018 and determined the presence or absence of sex- and gender-related content. We found that (1) the proportion of women authors was not associated with the presence of sex- and gender-specific content; (2) there was a slight increase in the proportion of women authors on ACC's CPG writing committees over time, which was not statistically significant; and (3) the inclusion of a discussion of the reasons for which sex and gender content was excluded did not increase over time.
Nielsen et al. 10 found a positive correlation between women authorship and the inclusion of sex and gender analysis. Similarly, we hypothesized that guidelines with a larger number of women authors would contain more sex- and gender-specific content but did not find such an association. In our analysis, there was a higher median proportion of women authors among ACC guidelines that included sex- and gender-related content and those which addressed reasons for which sex- and gender-related content was not included, but these differences were not statistically significant. In addition, we did not find a difference in the median proportion of women authors when comparing guidelines that contained a separate section within the guideline that addressed sex- and gender-related content and those that did not. Interestingly, only two guidelines had more than 50% women on the writing committees.
One reason that could explain the difference in our results compared to Nielsen's study is our small sample size. While there do appear to be some differences among median proportion of women authors, the difference is not statistically significant given the relatively small sample size and large variation in proportion of women authors within each group. Another reason that could explain the difference is that the field of cardiology was one of the first fields in medicine to examine disparities in diagnosis and treatment due to sex and gender. This awareness and subsequent increase in research leading to sex- and gender-specific diagnostic and therapeutic interventions in cardiology may have contributed to the addition of sex- and gender-specific recommendations to ACC's CPGs, regardless of the composition of the committees. As Nielsen et al. did not specifically review CPGs and included all specialties and as we only reviewed cardiology CPGs, this may account for the difference in our findings compared to Nielsen et al. 10
We commend the ACC as the majority of their guidelines (75.8%) did include some information about sex and gender. However, the breadth and depth of sex and gender content varied widely. Only 15 of the 33 guidelines included a more in-depth discussion on sex and gender, creating a specific section within the guideline to address sex- and gender-related content. For example, the guideline on management of non-ST elevation myocardial infarction (NSTEMI) 28 dedicates an entire section to recommendations for women in addition to having pertinent sex-specific data and recommendations throughout the guideline. This content includes sex-specific recommendations on the accurate dosing of anticoagulants based on weight and renal function to reduce the risk of bleeding among women, recommendations regarding which women may benefit from an early invasive strategy versus an ischemia-guided strategy, and a robust discussion of sex and gender disparities in treatment and outcomes. The authors also describe that women have higher rates of complications after NSTEMI and yet are more likely to be inappropriately discharged from emergency departments. In contrast, the 2017 Guideline for the Management of Heart Failure 40 does not provide a separate section or a more in-depth discussion on sex and gender despite known sex differences, such as consistently worse clinical outcomes in women. Although not of the scope of the current work, future in-depth qualitative analyses of ACC guidelines in conjunction with systematic reviews of the current literature on sex differences within specific topics may be one strategy to align better the known sex differences in management of cardiac conditions with the published guidelines.
Other authors have suggested methods to address sex and gender in CPGs, such as Tannenbaum et al., 6 who suggest including a sex/gender champion on guideline committees. We support Tannenbaum's approach to include a sex/gender champion on clinical guideline committees and suggest another option to include a specific section on sex- and gender-related content in every guideline, which 39% (13) of the ACC guidelines already include. When there are no sex- and gender-related differences, authors can state the lack of difference and cite the supporting evidence or report the lack of data in this section. By including such a section, readers will know that sex and gender differences were taken into consideration, analogous to the requirement to consider sex as a biologic variable in nationally funded grants.
We also found a low median percentage of women authors comprising the ACC CPG writing committees overall (22.2% with significant variability), with some CPGs with fewer than 5% women authors on their writing committees. After excluding one guideline that had a disproportionate number of women authors (81.1%), the median percentage of women authors of the remaining 32 guidelines decreased to 21.6%. Interestingly, when comparing guidelines from the first 5 years (2008–2013) to those of the last 5 years (2014–2018) of our study period, the median percentage of women authors did increase slightly, but this difference was not statistically significant, and the percentage of women authors on the ACC guideline writing committees still remained below 25%.
In a recent review of women representation in ACC/AHA Guideline Writing Committees, 12 Sarder et al. compared the number of women authors on CPGs before 2008 (13%) to the number of women authors on CPGs during 2008–2017 (23%), which is similar to our findings. Sardar et al. found that this increase in women authors reflected the increase in percentage of women practicing in cardiology subspecialities. 12 The authors summarize the importance of including women authors in cardiology guidelines: knowledge gaps may be highlighted, innovation may be sparked, and debates may be broadened as more diverse perspectives are included. Overall, it is critical for the physician workforce (including authors of CPGs) to mirror our patient population. Although not captured in our study, Sardar et al. reviewed ACC CPG women author credentials and found that 100% of women authors were affiliated with either academic institutions or the NIH and had an average of 20–25 years of experience. According to Mehta et al., the proportion of women adult cardiologists in the United States increased from 8.9% to 12.6% (p < 0.001) from 2006 to 2016. 48 Given that the proportion of female cardiologists has increased to some extent over time, we also hypothesized that women authors on cardiology guidelines would increase over the 10 years of our study period. While we found that the median proportion of women authors did increase over time, this increase was not statistically significant.
The cardiology community has highlighted women authorship as an issue 12 ; however, it is unknown whether other specialties are addressing gender and authorship in their writing committee guidelines. One comprehensive review of women authors in 454 CPGs demonstrated that there was a significant difference in the number of women authors among specialties. 11 Only three specialties were documented as having 50% or more of women authors (neurosurgery 50%, critical care 54.5%, and geriatrics 56.3%), with cardiology listed as 33.3%. 11
Limitations to our study include our small sample size and a lack of a qualitative analysis. While we did find some differences among the relationship of median proportion of women authors and sex and gender content, these differences were not statistically significant; this may be due to the small sample size and large variation within each group. Another limitation is that we did not perform a qualitative analysis of the sex and gender content in the ACC CPGs. While not originally a goal of this project, we realized the importance of performing a qualitative analysis during the analysis of our results and writing of this article. Future in-depth qualitative analyses will be helpful to outline the quality and quantity of sex- and gender-specific content in CPGs. An additional potential explanation for our findings is that sex- and gender-related differences were in fact included in certain guidelines but were removed during the peer review process, although it is not possible for us to determine if this occurred.
Conclusions
Sex and gender are critical factors affecting health care and are not routinely taken into consideration in clinical practice. In the future, researchers and authors should include sex and gender differences routinely in their studies and writing of CPGs. We propose including a specific section on sex- and gender-related content in every CPG, so that readers are aware that sex- and gender-related issues were considered. Our findings also point to continued gender disparities in authorship and suggest that changes need to be made with regard to the inclusion of women authors in CPG writing committees.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this article was received from the American Medical Women's Association.