
Abstract
Background:
Psychological well-being (PWB) is predictive of future health and mortality. Midlife is a pivotal time in women's lives and may impact future PWB. This study, based on a longitudinal cohort of women, sought to identify how personal and social resources and modifiable behaviors at midlife relate to women's PWB in later life, and to determine if psychological resilience in later life moderates the impact of health problems on PWB.
Materials and Methods:
We assessed the association of midlife factors with PWB ∼9 years later in 1693 women from the multiracial/ethnic Study of Women's Health Across the Nation (SWAN) cohort. PWB was a composite score with cognitive and affective components. Midlife factors included sociodemographics, health, menopause-related, and psychosocial factors collected over the course of midlife.
Results:
In a multivariable model, greater PWB at an older age was associated with the following at midlife: less financial strain, greater physical activity, not smoking, better physical functioning, and fewer sleep problems. More positive attitudes toward menopause and aging, less cynicism, greater optimism, less trait anxiety, greater spirituality, and greater resilience were also independently associated with better PWB. Chinese women reported lower PWB compared with whites. Later life resilience moderated the impact of sleep problems on PWB.
Conclusions:
Several modifiable factors at midlife are associated with better PWB in older women and highlight the importance of healthy behaviors such as physical activity and good sleep hygiene at midlife. Interventions to increase optimism, spirituality, and resilience are also worth exploring.
Introduction
Psychological or subjective well-being (PWB or SWB) has long been a major focus of studies of aging. Well-being has been conceptualized and defined in multiple ways, including SWB, PWB, positive affect, and life satisfaction. Two broad conceptualizations of well-being are hedonic and eudaimonic. Hedonic well-being refers to the pursuit of happiness and is generally characterized by high positive affect and the evaluation of one's life as satisfying. 1 Eudaimonic well-being typically refers to a more evaluative component and includes meaningful pursuits and personal growth as seen in the scales developed by Ryff. 2 PWB is considered the broadest and most all-inclusive term that covers SWB, cognitive reflections, and affect. 3 To assess this broad construct of PWB, studies often use multiple measures 4,5 or a composite score 6 that encompasses these various aspects of well-being.
Despite being defined and measured in multiple ways, PWB importantly has been shown to predict future health and mortality. 7 –10 For example, the longitudinal survey of Midlife Development in the United States (MIDUS) found that participants who were persistently high in PWB over 9–10 years had better subjective health, fewer symptoms, chronic conditions, and functional impairments compared with those who had persistently low PWB. 8 A study of men and women aged 60 years and older found that higher levels of life enjoyment predicted less impaired functioning 8 years later. 9 Positive well-being was also strongly related to less cardiovascular disease after 12 years of follow-up in an initially healthy group of men and women. 10
Given the importance of PWB or SWB for subsequent health and mortality, studies have examined determinants of well-being, although most of these are cross-sectional. 11 Education and income are strong predictors of well-being later in life, 12 with income being a bit stronger. Self-rated health, social integration, social support, a sense of control, and mastery have also been related to well-being. 11,13 In a cross-sectional study of women aged 65 years and older, Lukaschek et al. found that low income, physical inactivity, multimorbidity, depression, anxiety, and sleeping problems were associated with low SWB. 14 However, given the cross-sectional nature of the majority of this research, we know little about how earlier life characteristics impact well-being at older ages.
Dispositional factors such as psychological resilience and optimism may be related to PWB and may moderate decreases in physical function or increases in comorbidities associated with aging. Psychological resilience, a personal characteristic that enables one to thrive in the face of adversity and adapt to change, 15 has been shown to be protective in the face of worsening health or living circumstances in later life. 16,17 Longitudinal studies have also found that greater optimism 18,19 predicts better life satisfaction in later life.
Midlife can be a pivotal time in women's lives, with the menopausal transition representing a key physiological and psychosocial event. This transition, encompassing hormonal and biological changes, can provide a marker in the aging process, and may occur at a time of changes in family structure and social roles. All of these factors may influence women's health or lifestyle behaviors, which may have important implications for later PWB. In conceptualizing well-being during the menopausal transition, Brown et al. considered both hedonic well-being and eudaimonic well-being important. 20 Their systematic review of studies of positive well-being during the menopausal transition identified a range of factors related to well-being, including stress, life events, loneliness, exercise, smoking, work satisfaction, attitudes toward aging and menopause, and mastery.
Only one study, however, went beyond the transition. 21 The Melbourne Women's Midlife Health Project (MWMHP) reports longitudinal data on life satisfaction and well-being among 267 mostly white women who were followed for 9 years over the menopausal transition. They found that more positive attitudes toward aging and menopause, positive feelings for partner, fewer daily hassles, and not smoking were related to better later life satisfaction. 21 They also found that becoming married or partnered and increased work satisfaction were related to more positive well-being (defined as the difference between positive and negative affect), while experiencing a major life event and increased daily hassles were related to decreased well-being 9 years later. 22
The present analyses take advantage of data from the 20-year longitudinal multiethnic/racial Study of Women's Health Across the Nation (SWAN) to evaluate how factors collected over the course of midlife contribute to PWB measured ∼9 years later. Specifically, the objectives of the present study are as follows: (1) to examine the extent to which personal and social resources and modifiable behaviors at midlife contribute to women's PWB at later life, and the extent to which race or ethnicity is associated with PWB; and (2) to determine if concurrent psychological resilience moderates the impact of health problems (e.g., poor health, sleep problems) or negative events on PWB in older age.
Materials and Methods
Sample and procedures
SWAN is a multiracial/ethnic cohort study characterizing biological and psychosocial changes occurring during the menopausal transition. 23 From 1995 to 1997, each of seven clinical sites recruited non-Hispanic white women and women belonging to a predetermined racial/ethnic minority (African American women in Pittsburgh, Boston, Michigan, Chicago; Japanese women in Los Angeles; Hispanic women in Newark; Chinese women in Oakland, California). The protocol was approved by the institutional review boards at each site. All participants provided written informed consent.
Baseline eligibility included age 42–52 years; an intact uterus and at least one ovary; not pregnant, lactating, using oral contraceptives, or hormone therapy (HT); and having a menstrual cycle in the 3 months before screening. Among cohort-eligible women, 50.7% (n = 3303) entered the longitudinal study. 23 The SWAN cohort sample size was determined to have adequate power to detect menopause transition-related within-women changes in outcomes. Participants were assessed in-person at baseline and through follow-up visit 15 from 1996 to 2017 using a standardized protocol of detailed questions about medical, reproductive, and menstrual history; lifestyle and psychosocial factors; physical and psychological symptoms; and anthropometric measurements. Visits occurred approximately annually until after visit 10 when they were spaced further apart. All instruments were translated into Spanish, Japanese, and Cantonese.
PWB was measured for the first, and only, time at follow-up visit 15 and was obtained from 1911 women still participating in SWAN at that follow-up visit. Reasons for nonparticipation at visit 15 were as follows: withdrew from SWAN before visit 15 (n = 788), missed the visit (n = 275), and deceased (n = 149). Of the 2091 women still participating in SWAN, 180 did not complete the measures of well-being because they either had an abbreviated telephone interview or did not complete the full SWAN protocol (n = 106), or had missing data on one or more of the well-being scales (n = 37).
Researchers have generally considered midlife to encompass the ages of 40–60, but also consider other factors, making it a relative approximation. 24 For the purpose of these analyses, we consider the ages of 40–60 as midlife, but also take the menopause transition into account. In considering midlife predictors of PWB, we include SWAN data from baseline to visit 10 encompassing ages 42–60. Our primary outcome, PWB, which was measured at visit 15, occurred ∼9 years after visit 10 when women were ages 61–69. We exclude women from analyses who were older than 60 at or before visit 10 (n = 211), had not yet entered the menopause transition by visit 10 (n = 5), or were not yet postmenopausal by visit 15 (n = 2), for a final sample size of 1693. Supplementary Fig. S1 shows when SWAN visits occurred and the age of the sample at these visits.
Measures
Primary outcome
To include both the hedonic and eudaimonic aspects of PWB, we developed a composite measure of PWB consisting of four measures: the Satisfaction with Life scale, 25 the Positive and Negative Affect Scale (PANAS) positive affect scale 26 and the Ryff Purpose in Life and Personal Growth scales. 2 The Life Satisfaction scale contains 5 items (e.g., “I am satisfied with my life,” “So far, I have gotten the important things I want in life”) that are rated on a 7-point scale from strongly disagree to strongly agree. Items are summed to create a total score where high scores reflect greater life satisfaction. The PANAS positive affect scale, 26 which contains 10 adjectives (e.g., interested, excited, alert) asking how a person felt in the past 7 days, served as the affective measure. Responses are on a 6-point scale that range from very slightly or not at all to extremely. The Purpose in Life and Personal Growth scales each contain 7 items asking respondents to rate their agreement on a 6-point scale from strongly disagree to strongly agree with statements such as: “I have a sense of direction and purpose in life” and “For me, life has been a continuous process of learning, changing, and growth.”
Principal component analysis (PCA) was used to examine the factor structure of the four well-being measures. The PCA was run on standardized values of the total scores of each of the four well-being measures to account for differences in scales and variances. Examination of PCA results, including scree plots and eigenvalues, indicated one factor, with all items loading strongly on the factor (Cronbach's alpha = 0.77). The composite score was created by using factor loading results as weights for each of the scales and then summing the weighted values. The PWB score is thus also a standardized score, with a mean of zero and a standard deviation equal to one.
Predictors
Midlife predictors of later life PWB were selected to include sociodemographic, health-related, menopause-related, and psychosocial factors considered to influence SWB 13 and previously found to be associated with PWB during the menopause transition. 20 Predictors included (1) those that were obtained once during the midlife period and were not considered to be time-varying (race/ethnicity, educational attainment, duration of perimenopause, cynicism, optimism, trait anxiety, spirituality); (2) those that were obtained annually during midlife and were considered to be time-varying (difficulty paying for basics, marital status, self-assessed health, comorbidities, sleep problems, quality of life, use of HT, vasomotor symptoms (VMS), smoking, physical activity, body mass index (BMI), anxiety, depressive symptoms, stress, and social support); and (3) those that were concurrent with PWB at visit 15 (age at visit 15, resilience).
Because we only have one measure of PWB in later life, time-varying midlife predictors were summarized for modeling. To do this, we considered baseline through visit 10 to be the midlife period and obtained cumulative values of predictors from all available visits during this time. Area under the curve (AUC) analysis was used for continuous predictors. We calculated AUC for each time-varying continuous predictor using Reimann sums. 27 The proportion of visits from baseline through visit 10 with reporting of a specific characteristic (e.g., the proportion of visits the participant reported being married/partnered vs. not) was used to summarize dichotomous time-varying predictors. For predictors that were unlikely to change over time (e.g., education), we used values from SWAN baseline or the visit at which the predictor was assessed since these were not assessed at every visit. Predictors were organized into five domains: sociodemographic, health-related, menopause-related, health behaviors, and psychosocial factors. Details of the measures used are provided below.
Sociodemographic variables were race/ethnicity, age at visit 15, educational attainment (<high school, high school or some college, college/more than college), the proportion of visits with difficulty paying for basics (somewhat/very hard to pay for basics vs. not at all hard), and the proportion of visits married or partnered. Ethnicity was self-defined at baseline by participants in response to the open-ended question: “How would you describe your primary racial or ethnic group?” Responses were categorized as white, black, Chinese, Hispanic, or Japanese.
Health-related factors included the proportion of visits with self-assessed health rated fair or poor; number of medical conditions ever reported during midlife (none, 1, or 2 or more of the following: diabetes, hypertension, high cholesterol, arthritis/osteoarthritis, under/overactive thyroid, heart attack, angina, or stroke); and the proportion of visits with sleep problems (any of the following: difficulty falling asleep, staying asleep, and/or early morning awakening reported ≥3 times/week in past 2 weeks). We also examined three domains from the SF-36, 28 which assesses the impact of health in various life areas: physical functioning, role limitations due to physical health, and role limitations due to emotional health. For all three domains, we used the previously used cut-point of scoring in the lowest 25% to indicate poor functioning 29 and computed the proportion of visits with poor functioning in each domain. We also controlled for psychiatric medication use at visit 15. Participants completed a detailed medication review, and those reporting having taken antidepressant, anxiolytic, or antipsychotic medications were classified as psychiatric medication users.
Menopause-related variables included duration of perimenopause (calculated as the estimated time a woman began early perimenopause, defined as bleeding in the previous 3 months and changes in menstrual regularity in the past year, to one year after the final menstrual period), ever use of HT, attitudes toward menopause and aging from Visit 9, 30 and the proportion of visits with frequent VMS, defined as experiencing hot flashes or night sweats, at least 6 days in the previous 2 weeks. Duration of perimenopause was used instead of menopause status because 97% of women were postmenopausal by visit 15 and longer duration of perimenopause has been shown to be an important variable related to depression. 31
Health behaviors included physical activity (AUC) 32 and BMI (weight [kg]/height [m2] [AUC]), and the proportion of visits reporting cigarette smoking. The physical activity measure in SWAN, referred to as the Kaiser Physical Activity Survey (KPA) is adapted from the short physical activity survey developed by Baecke. 33 We used the total score that includes the sports, active living, and household/childcare domains.
Psychosocial factors included a one-time measure at baseline of cynicism from the Cook-Medley Cynicism scale 34 ; optimism as measured by the short version Life Orientation Test 35 at visit 1; trait anxiety by the Spielberger State-Trait Anxiety Inventory at visit 4, 36 and spirituality by the Daily Spiritual Experience Scale 37 at visit 4. Other psychosocial measures were the cumulative measures of the proportion of visits with high anxiety (sum of 4 items with score ≥4), the proportion of visits with depressive symptoms (Center for Epidemiologic Studies Depression [CES-D] ≥16 CES-D scale), 38 proportion of visits with 2+ stressful life events, and perceived stress (AUC of summed score of 4 items), 39 and emotional and instrumental social support (AUC). 40 Psychological resilience was measured at visit 15 with the 10-item Connor-Davidson Resilience Scale. 15
Statistical analyses
Preliminary analyses included descriptive plots and statistics (means, standard deviations, ranges, frequencies), as well as an examination of the correlation among predictors. Continuous variables were assessed for normality and transformations applied as necessary.
Multiple linear regression was used to assess the relationship of the PWB composite score with midlife health status, health behaviors, psychological and social function, and menopause-related and socioeconomic characteristics. Nontime-varying variables were ethnicity, education, daily spiritual experiences, trait anxiety, optimism, hostility, and attitudes toward menopause, as these variables were either measured at one visit or are thought not to change over time. All other variables were summarized from visits baseline to 10 as described in the methods.
All linear regression models included age, ethnicity, and clinical site. Remaining variables were then assessed separately within their domains (sociodemographic, health-related, menopause-related, health behaviors, and psychosocial) for collinearity and significance of relationship with the PWB score. Variables that were significant at p < 0.05 within each domain were included in the final multivariable model and manual backward elimination was performed until all variables in the model (except forced—site, age, ethnicity, psychiatric medications at visit 15) were significant at p < 0.05. In addition, we tested the interactions between psychological resilience and stressful life events, perceived stress, self-reported health, number of comorbidities, and sleep problems.
SAS system version 9.3 (SAS Institute, Inc., Cary, NC) was used for all analyses.
Results
Sample characteristics
Characteristics of the analytic sample at the SWAN baseline are shown in Table 1. The mean age of the sample at the beginning of SWAN was 45.8 years, about 69% of women were partnered, almost half (47.9%) had completed college, and 58.6% were premenopausal and 41.4% early perimenopausal.
Baseline Characteristics of the Analytic Sample Expressed as Percentage of Sample Unless Otherwise Noted (n = 1693)
BMI, body mass index; CES-D, Center for Epidemiologic Studies Depression; VMS, vasomotor symptoms.
Bivariate associations between predictors and PWB score
Table 2 shows the bivariate associations between the predictors and PWB. As can be seen in this table, most predictors were significantly associated with PWB in the expected direction. Better PWB was associated with being partnered; more positive attitudes toward menopause and aging; and greater physical activity, optimism, resilience, spirituality, and social support. Lower PWB was associated with less education; difficulty paying for basics; sleep problems; self-reported fair/poor health; poor role physical, role emotional, and physical function; frequent VMS; current smoking; higher BMI; greater cynicism; both trait and state anxiety; depressive symptom; 2+ stressful events; and greater perceived stress. Compared with women with no comorbidities, having only one comorbidity was not significantly related to PWB, but having two or more comorbidities was. Blacks did not differ significantly from whites, although Hispanic, Chinese, and Japanese women had significantly lower PWB compared with whites. The only variables not associated with PWB were age, duration of perimenopause, and ever use of HT.
Bivariate Associations Between Predictors and Psychological Well-Being
Adjusted model of PWB
Before analyzing an adjusted model, we analyzed together the predictors listed above within each domain to check for collinearity and to identify which predictors within the domain were significantly associated with PWB. The following variables were significant within the domain models and were included in the multivariable modeling process: sociodemographic factors: education and difficulty paying for basics (financial strain); health-related: self-assessed health, sleep problems, role emotional, and poor physical function; menopause-related: attitudes toward menopause; health behaviors: physical activity, smoking; psychosocial: trait anxiety, optimism, cynicism, depressive symptoms, stressful life events, perceived stress, spirituality, and resilience.
In the adjusted model (Table 3), greater PWB at an older age was associated with the following characteristics at midlife: greater physical activity, more positive attitudes toward menopause and aging, greater optimism, and greater spirituality, and greater resilience at visit 15. Difficulty paying for basics, poor physical function, sleep problems, smoking, cynicism, and trait anxiety at midlife were all associated with lower PWB. We also found racial/ethnic differences with Chinese women reporting lower PWB compared with whites.
Adjusted Model of Psychological Well-Being
Bold indicates significance.
Also adjusted for study site.
AUC, area under the curve.
Of those variables tested for an interaction with resilience (self-reported health, number of comorbidities, stressful life events, sleep, and physical function), the only variable that had a significant interaction with resilience was sleep (β = 0.02, p = 0.01). Reporting sleep problems was negatively related to PWB when resilience was low, but was unrelated to PWB when resilience was high. This interaction is depicted in Figure 1where the Connor-Davidson score is broken into four levels for illustrative purposes.
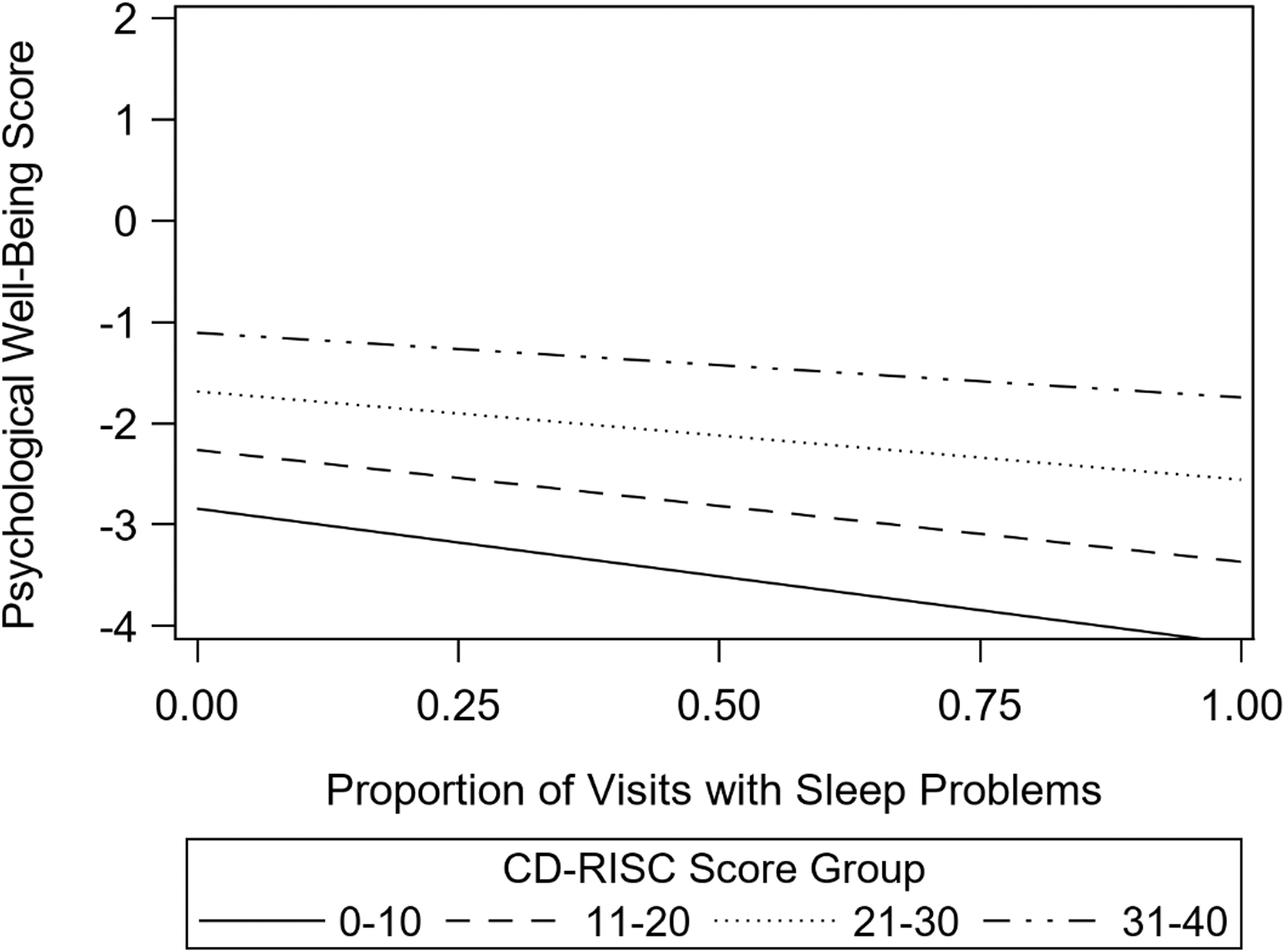
Relationship between psychological well-being and sleep problems across levels of psychological resilience. CD-RISC, Connor-Davidson Resilience Scale.
Discussion
Our study identified a range of factors assessed over the course of midlife that were related to better PWB at later life. Most notably, modifiable factors such as higher levels of physical activity, not smoking, and fewer sleep problems were each independently related to better PWB at an older age. The health benefits of physical activity have been well documented 41 and studies have shown a positive association between physical activity and SWB in older adults. 14 However, studies have also reported declines in physical activity with age. 42 MIDUS has shown that over an 18- to 20-year period of middle and later life, 50% of respondents showed a steady decline in physical activity. 43 Nevertheless, in general, these declines in physical activity are not inevitable and physical activity can be increased during middle and later life. 44 A regimen to increase physical activity at midlife and beyond is feasible and important for later well-being.
Sleep health is also increasingly recognized as critically important for health and well-being, 45 –47 yet numerous studies have shown that sleep problems increase with age with 40%–60% of postmenopausal women reporting poor sleep. 48 Our results highlight the importance of sleep during midlife for long-term well-being and suggest that mitigation of sleep problems in midlife may have benefits for PWB in later life. An increasing body of evidence points to effective behavioral modifications that help improve sleep. 49,50 Taken together, these results provide further evidence that middle age may represent an important time point for improving health behaviors for future PWB.
We also found several dispositional characteristics related to better PWB. Greater optimism, spirituality, lower trait anxiety, and cynicism at midlife were all independently related to better PWB at an older age. Although other studies have also shown that these characteristics are related to better well-being, 18,19 it is worth pointing out that these characteristics were all independently associated with better PWB at an older age. Although these characteristics are generally viewed as stable over time, there have been some attempts to increase optimism 19 and spirituality 51 and such interventions are worth pursuing. It is also possible that PWB earlier in life led to greater optimism. Although longitudinal studies have also found that greater optimism 18,19 predicts better life satisfaction in later life, one cannot rule out the possibility that PWB is a precursor to optimism.
Consistent with other studies, 4 poor physical function over midlife was negatively related to PWB. Although social support was significantly related to PWB in the bivariate analyses, it was not significant in the final multivariable model building, possibly due to its correlation with resilience (positive) and cynicism (negative). The presence of depressive symptoms was also significant in the bivariate analysis and the multivariable model building, but dropped out of the final model due to its correlations with poor physical function and sleep problems. These results suggest that resilience, physical function, and sleep problems may be especially important and modifiable factors related to PWB.
In terms of racial/ethnic disparities, blacks did not report significantly lower PWB compared with whites in either bivariate or multivariable analyses. A deeper look at our composite measure of PWB revealed that blacks scored significantly lower than whites on the Life Satisfaction measure, but not the Ryff or PANAS measures. We note that studies finding racial differences in SWB tend to focus on life satisfaction, 52,53 thus suggesting that racial differences may vary by specific measure. Consistent with our findings, a study from the Women's Health Initiative did not find significant differences between whites and non-whites older than the age of 80 on the Ryff Personal Growth or Purpose in Life measures. 54 We also found that Chinese women reported significantly lower PWB compared with white women, even after controlling for a range of variables. Although we are unable to find other studies that specifically compare Chinese women with white women on PWB. Cross-cultural research suggests that well-being is likely to have different meanings across cultures, 55,56 but it is beyond the scope of this article to determine if the ethnic differences in SWAN are reflections of “real” differences in PWB or if they reflect cultural differences in response to these items.
We hypothesized that psychological resilience would moderate the relationship between health problems (poor self-assessed health, comorbidities, and sleep problems) and stressful life events and PWB. Results showed that resilience only moderated the relationship between sleep problems and PWB such that sleep problems at midlife had a greater negative impact on PWB among those women with low resilience. It is possible that resilience did not reduce the effect of stressful life events as this measure takes into account a person's perceptions of stressfulness and perhaps the same event is less likely to be rated as stressful among women with higher levels of resiliency. It is also possible that resilience did not moderate the relationships between comorbidities or physical function and PWB as the Connor-Davidson scale measures psychological resilience and may have less influence on physical measures. Nevertheless, results suggest that resilience may help reduce the negative impact of sleep problems on PWB.
We should also point out that resilience was measured only at visit 15, concurrently with PWB, and not at midlife, although there is some evidence that resilience as measured by the Connor- Davidson Resilience Scale is relatively stable. 57 Taken together, our findings suggest that resilience may play an important role in PWB as women age. Although the research on interventions to increase resilience is sparse, there is some evidence that resilience can be increased among older adults 58,59 and such interventions are worth investigating for middle-aged and older women.
The study has several limitations. Although results are based on a multiracial/ethnic cohort, some of these groups were too small to stratify results by race/ethnicity. Second, the analyses only include women who were still active in SWAN at visit 15. SWAN, like other cohort studies, has loss to follow-up and those women who dropped out before V15 were likely worse off in terms of physical and/or emotional health than those still participating. However, this bias is unlikely to impact the identification of factors related to better PWB. One should also interpret the results related to dispositional characteristics with caution, as there is some overlap between these concepts and PWB. Finally, we did not have a baseline measure of PWB and were thus unable to examine change in PWB from midlife to older age.
Important strengths of this study include the following: (1) the availability of multiple repeated standard measures of diverse psychosocial and health-related correlates of PWB and menopausal status; (2) the long follow-up period that allows for the evaluation of modifiable risk factors across the menopausal transition and midlife; and (3) a diverse sample with respect to race, ethnicity, and geography. This study adds to previous literature by highlighting the importance of healthy behaviors during midlife for better PWB at older ages. In addition, we found that Chinese women report significantly lower PWB compared with white women, even after controlling for a range of variables. However, it is unclear whether this is due to cultural biases in reporting well-being or actual well-being.
This study provides information for clinicians and women about midlife factors that are important for PWB in older age and are modifiable, including sleep behaviors and physical activity. Such factors can be addressed both in midlife and beyond to help women achieve successful aging. Results further suggest that interventions to increase optimism, spirituality, and resilience are worth exploring.
Footnotes
Acknowledgments
We thank the study staff at each site and all the women who participated in SWAN.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Study of Women's Health Across the Nation (SWAN) has grant support from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging (NIA), the National Institute of Nursing Research (NINR), and the NIH Office of Research on Women's Health (ORWH) (Grants U01NR004061; U01AG012505, U01AG012535, U01AG012531, U01AG012539, U01AG012546, U01AG012553, U01AG012554, and U01AG012495). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the NIA, NINR, ORWH, or the NIH.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.