
Abstract
Background:
The average age of the homeless population is and will continue to rise. Although women comprise a significant and growing percentage of this vulnerable population, their age- and sex-specific health characteristics are poorly understood.
Materials and Methods:
This integrative review appraises published research addressing the physical and behavioral health characteristics of aging homeless women (≥50 years) in the United States (2000–2019). The authors searched six electronic databases to identify eligible studies. Studies were screened for methodological quality by using the Johns Hopkins Nursing Evidence-Based Practice model. The review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Results:
Ten primary studies met the review eligibility criteria. All were level III (non-experimental); nine appraised as “good” quality (level B), and one as “lower” quality (level C). Aging homeless women demonstrate elevated rates of physical health conditions, related to suboptimal nutrition, lower than expected preventive health screening uptake, and geriatric concerns. Disproportionate rates of mental health conditions are compounded by substance use and interpersonal trauma. Familial and social dynamics and socioeconomic disadvantage contribute to social health concerns. Spiritual health is a critically important yet underexplored protective factor.
Conclusions:
Studies are limited, though collective findings suggest that aging homeless women endure a disproportionate physical, behavioral, and social health burden compared with aging non-homeless women and aging homeless men. Implications for research on early aging, preventative health strategies, and homelessness among women, and clinical practice in the context of geriatric and women's health are described.
Introduction
The average age of the homeless population is increasing and will continue to rise. 1 –8 Over the past three decades, the median age of a homeless person in the United States has risen from the late 20s to about 50 years of age. 9,10 Older adults in the United States are at higher risk for homelessness than at any point in recent history, and by 2050, homelessness is projected to double nationally among people aged 65 and older. 11 Aging people are especially vulnerable to the negative health consequences of homelessness. 12 Due to early physiological aging, 13,14 homeless people as young as 50 years of age experience health conditions at rates on par with non-homeless older people chronologically 20 years older. 14 It is projected that the aging of the homeless population will result in an estimated $5 billion annually in health care and shelter costs. 7
Although increasing research has focused on the aging homeless populations, representation of women in most studies ranges from 4% 12 to <25%. 15,16 This is problematic, as more women are becoming homeless for the first time in mid- to late life. 6,17 –19 During midlife and older age, 20 women are often socially and economically vulnerable, relating to relationship breakdown, 17 abusive relationships, illness, and/or employment issues. 21 However, little is known about the unique age- and sex-specific health characteristics and needs of aging homeless women. By synthesizing studies focusing on physical and behavioral health characteristics of aging homeless women, unique health and health care needs can be identified, and population-specific research and clinical priorities established.
This integrative review evaluated the question: What are the physical and behavioral health characteristics of homeless women aged 50 and older in the United States? Findings from this review identify the state and quality of the science on this topic, implications of existing research findings, and areas requiring further research.
Materials and Methods
Article eligibility criteria
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. 22 Eligible studies included those focused on actively homeless cisgender females with a mean/median sample age ≥50 years; were conducted in the United States; were published in English in the year 2000 or later; and assessed physical and/or behavioral health characteristics. Diverse methodological approaches were eligible. Studies including non-homeless females or homeless males were eligible when used as a comparator population, including separate analyses of aging homeless women's health. Ineligible studies included those sampling at-risk for or formerly homeless, incarcerated or otherwise institutionalized populations; and/or explored topics not directly pertaining to physical or behavioral health characteristics (e.g., health care utilization). Non-empirical and non-peer reviewed studies (e.g., commentaries, protocols) were ineligible.
Conceptual definitions
For the literature search, physical health refers to the presence or absence of physiologic conditions, injury, or disabilities of the body that are separate from mental health conditions. Behavioral health focuses on emotional and psychological well-being, including mental health and substance use disorders. 23 The U.S. Department of Housing and Urban Development (HUD) definition of homelessness was used: “individuals who lack resources and support networks to obtain permanent housing.” 24
Information sources and search strategy
Table 1 reports results of a search strategy that was created and executed by a medical librarian (LLP) in six databases: (1) Medline (via Ovid); (2) Embase; (3) Ovid Nursing Database; (4) Cochrane Library (via Ovid); (5) Cumulative Index to Nursing and Allied Health Literature (CINAHL) (via EBSCOhost); and (6) Web of Science. The search used controlled vocabulary and free text synonyms for the concepts: homeless, women, women's health; subject headings were used to exclude research focused on pediatric populations or populations outside the United States.
Medline (Ovid) Search Strategy
Search Command Key.
= denotes wildcard character.
/ = denotes Medical Subject Heading.
Exp = denotes exploded Medical Subject Heading.
ti,ab. = denotes keyword search in title and abstract.
Search outcome
The database searches yielded 6184 records from each database's inception date through December 17, 2019; citation-index searching 25 yielded one additional record (n = 6185). After removing duplicates, 3177 records remained; articles were collated and uploaded into Covidence®. 26
Article review
Figure 1 reports the PRISMA flow diagram, which details the review process. A comprehensive data search (Table 1) accounted for the substantial number of records (n = 3177) initially included in title and abstract screening. Two reviewers with expertise in women's health and vulnerable populations (K.A.D., S.E.L.) independently screened each article's title and abstract against eligibility criteria and found that 3089 records did not meet eligibility criteria. Of the 88 remaining articles eligible for full-text screening, 78 did not meet eligibility criteria for reasons detailed in Figure 1.
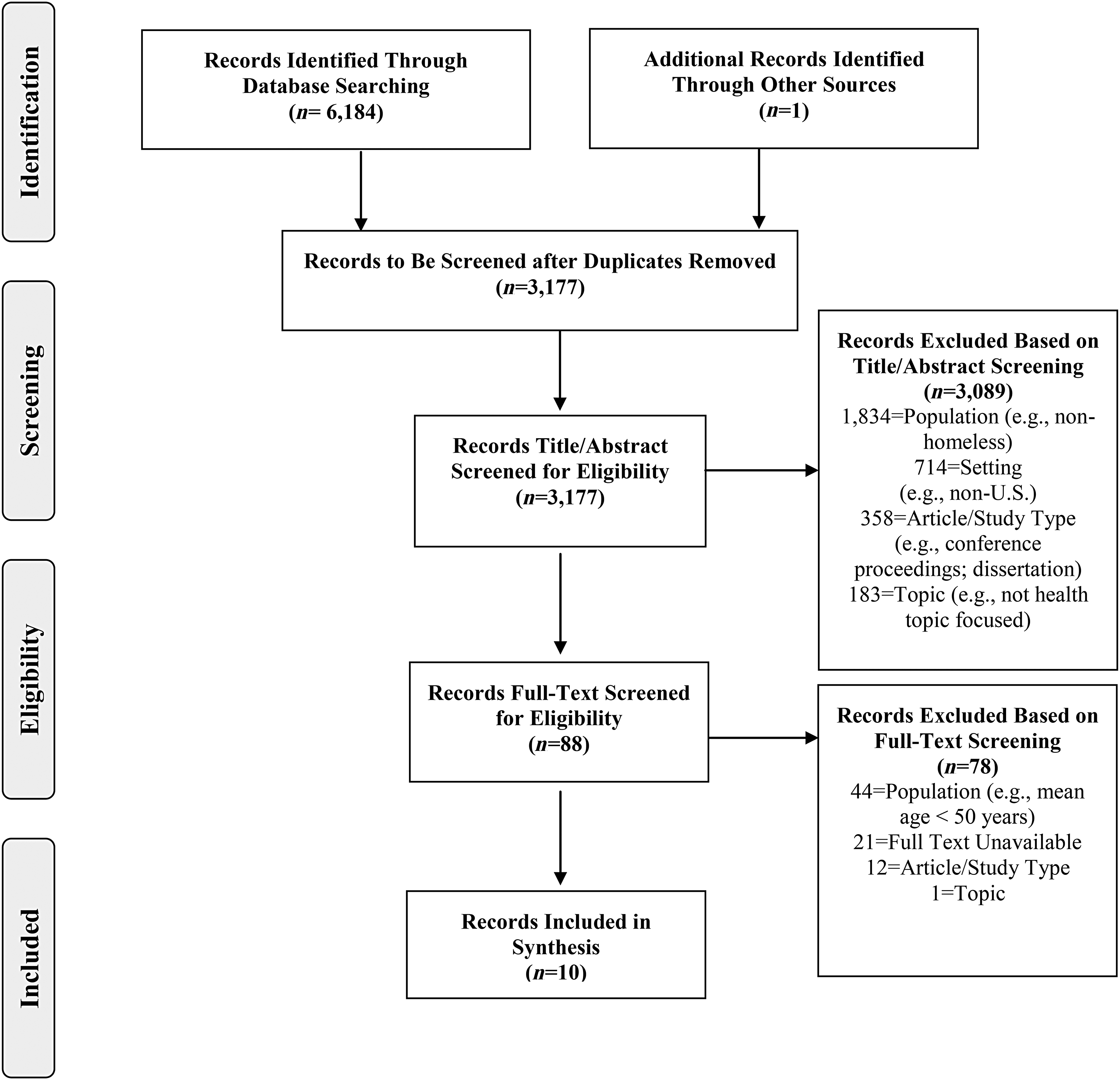
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Assessment of evidence quality
All articles that met eligibility criteria were independently appraised by two reviewers (K.A.D., S.E.L.) using the Johns Hopkins Nursing Evidence-Based Practice (JHNEBP) Research Evidence Appraisal Tool. 27 First, the level of evidence (I, II, III) was determined. Level I indicates a randomized controlled trial or experimental study, level II a quasi-experimental study, and level III a non-experimental study. Next, the quality of each article was determined (A, B, C): level A indicates high quality, level B good quality, and level C lower quality evidence. 28
Data extraction and synthesis
Key study and sample characteristics were then extracted from each study in preparation for synthesis (Tables 2 and 3).
Study Characteristics
BMI, body mass index; PSH, permanent supportive housing; PTSD, post-traumatic stress disorder; VA, veterans affairs.
Study Sample Characteristics
Range, mean age ± SD reported, as available.
IQR, interquartile range; SD, standard deviation.
Results
Study characteristics and quality rating
Eligible studies were published between 2002 and 2019, representing all five major U.S. regions: West, Southwest, Southeast, Midwest, and Northeast (Table 2). Sample sizes ranged from 5 to 223 homeless women ≥50 years old, with the majority of participants being African American/Black and Caucasian/White (Table 3). Six were quantitative studies, and four were qualitative studies. All 10 studies were categorized as level III (non-experimental), with 9 (90%) appraised as “good” (B) quality, and 1 (10%) of “lower” (C) quality (Table 2).
Synthesis of key study findings
After careful review of the 10 articles, an inductive thematic synthesis approach 29 was used to generate descriptive themes to categorize the articles. Initial themes included: (1) physical health and (2) behavioral health. After further discussion, the authors identified two additional themes that emerged from the articles: (3) social health, which refers to one's relationships with other individuals, one's community, and/or society, which are influenced by norms, policies, and systems, 30,31 and (4) spiritual health, which refers to one's sense of connection or relationships with an ultimate being or superior existence, with oneself, others, and/or nature. 32,33
Physical health
Findings pertaining to the theme of physical health of aging homeless women were categorized into two domains: (1) general health, (2) chronic physical conditions, and four sub-domains: (a) risk factors for chronic physical conditions; (b) suboptimal nutrition; (c) cancer and cancer screening; (d) geriatric conditions.
General health
General physical health was a critical feature of overall health that was emphasized across articles. General physical health was described as comparatively low among aging homeless women, who experienced lower self-reported physical health scores in comparison with other populations, including non-homeless aging women. 34,35 Aging homeless women were found to be less healthy than aging homeless men, indicated by a greater number of medical diagnoses. 36 Having “poor” or “fair” self-rated health was a significant predictor of homelessness among aging women veterans, 35 and nearly 70% of aging homeless African American women self-rated their health as “poor” or “fair,” 34 reflective of overall poorly self-rated general health.
Chronic physical conditions
Chronic physical conditions of various types were prevalent among aging homeless women. Specifically, across the seven studies that addressed physical health issues, 75% 37 to 100% 18 of aging homeless women had at least one documented chronic physical condition diagnosis. Higher rates of chronic physical condition diagnoses among aging homeless women than non-homeless aging people were noted, 34 and aging homeless women were more likely to have chronic physical conditions than aging homeless men. 36 Only one study detailed chronic physical condition prevalence by condition type, reported by aging homeless African American women, including: hypertension (60.8%); arthritis (50.5%); respiratory illness (44.3%); “ulcers” (32%); “heart trouble” (28.9%); anemia (28.9%); diabetes (12.4%); liver issues (10.3%); and HIV/AIDS (3.1%). In this study, the number of chronic conditions appeared to increase with length of time homelessness. 34 Aging homeless women endorsed the presence of physical pain as another chronic condition. 38 Although various types of chronic physical conditions were documented as prevalent across studies, details regarding self-perceived management and impact of these conditions were lacking.
Risk factors for chronic physical conditions
Increased risk for chronic physical conditions among aging homeless women was evident. This heighted the risk related primarily to elevated cholesterol and overweight/obesity, which were the primary documented risk factors for chronic physical conditions among aging homeless women highlighted in the included studies. One study found that 44% of 52 aging homeless women had elevated non-fasting total cholesterol levels, and 33% had elevated triglyceride levels. 39 In this same study, nearly one-third of the sample (31%) was overweight (15.4%) or obese (15.4%), suggesting increased risk for cardiovascular disease and diabetes. 39 Although many were overweight/obese, the vast majority conversely had a very low body mass index, with mid-arm muscle mass area measurements indicating low body fat stores and potential muscle wasting. 39 Although the presence of elevated cholesterol and overweight/obesity was documented, there was little emphasis on assessment, management, and impact of other forms or features of chronic physical condition risk in the included studies.
Suboptimal nutrition
For aging homeless women sampled in the included studies, nutritional status was non-optimized, though there was an expressed desire for education and healthier dietary opportunities. Among these women, average daily caloric intake fell below federal daily recommendations (mean = 1460 calories daily), and dietary intake was lower than recommended levels for nearly all nutrients. Data obtained from 24 hours dietary recall ranged from 220 to 3992 calories, and the average reported duration of going without food was 1.5 days. 39 Further, women conveyed concerns about the quality and nutritional value of shelter meals. 39 Barriers to obtaining nutritious foods were noted, and aging homeless women expressed their desire for education regarding healthy eating on a budget, 38 demonstrating an opportunity for optimizing low-cost nutritional options among aging homeless women.
Cancer and cancer screening
The impact of cancer and the value of cancer screening for aging homeless women was evident, though information across articles regarding cancer diagnoses and screening rates was limited. One study reported cancer diagnosis rates, revealing that 9% of 100 aging homeless African American women self-reported a cancer diagnosis. 34 In a retrospective evaluation of breast cancer screening rates and related outcomes among 26 aging homeless women with documented mammogram results, more than half of the women's mammogram results were unknown (n = 14), 10 were normal, 1 was abnormal, and 1 signified a breast cancer diagnosis. 37 The rate of aging homeless women who were up-to-date with breast cancer screening was lower in comparison to the national average (59% homeless vs. 72.2% non-homeless). Aging homeless women explicitly expressed a need for cancer screening, 38 suggesting opportunities for structured clinical approaches to improve cancer detection in this high-risk population.
Geriatric conditions
Geriatric conditions were prevalent among aging homeless women. In the included articles, exploration of geriatric conditions focused primarily on functional status and falls, with expressed need for greater evaluation of other age-associated conditions. In one sample of aging homeless women, although 80% of 20 participants reported ability to walk independently and 65% did not use an assistive walking device, 70% reported having fallen within the past year, and 35% reported having fallen within the past 30 days. 38 Data regarding frailty scores, bone mineral density, or fracture incidence specific to aging homeless women were not explicitly reported in any study included in this review. Although no studies reported rates or impact of memory impairment, aging homeless women expressed a need for memory testing. 38 Functional status and falls have been demonstrated as crucial geriatric concerns among aging homeless women, whereas evaluation of other age-associated conditions that are pertinent to the healthy aging of this population (e.g., cognitive health) requires further attention.
Behavioral health
Findings pertaining to the theme of behavioral health of aging homeless women were categorized into two domains: (1) mental health conditions, (2) substance use; and one sub-domain: (a) trauma experiences (adverse childhood events, adult abuse, sexual coercion).
Mental health conditions
Mental health issues were described in 8 of the 10 included studies, 17 –19,34 –37,40 highlighting the importance of this domain in the overall health of aging homeless women. One study reported the prevalence of mental illness history in more than half (56.8%) of the study sample of aging homeless women. 37 In another study, nearly one-third of the study sample of 223 aging homeless women attributed mental health difficulties as a major cause of homelessness. 19 When compared with aging homeless men, older homeless women were two and one-half times more likely to have any chronic mental health condition, and they were diagnosed with more mental health conditions. 36 Moreover, aging homeless women veterans were more likely to screen positive for an anxiety disorder and/or post-traumatic stress disorder, and had lower self-reported mental health scores than non-homeless women veterans, as measured by mental health items on the Short Form-12 (SF-12) survey. 35 Across studies, the pervasive impact of various forms of mental health conditions was apparent and highlighted as a critical feature in the comprehensive understanding of the overall health of aging homeless women.
Substance use
Substance use—in its various forms—was a noteworthy topic of focus across the majority of articles, underscoring the impact of this domain on the health of aging homeless women. Specifically, to differing degrees, 8 of the 10 studies described issues related to various types of substance use. 17 –19,35,37 –40 In studies that reported alcohol use separate from other substances, rates were relatively low, ranging from 2.2% of 44 participants 37 to 18% of 52 participants. 39 Aging homeless women veterans were more likely than their non-homeless veteran counterparts to use tobacco 35 ; the only study to report a rate showed that just more than one-third of 44 participants had a tobacco use history. 37 In one study, alcohol and marijuana were the primary substances used by aging homeless women, and substance use was influenced by familial substance use, triggered by stressful situations, and used as a coping mechanism to escape from life situations; moreover, most participants expressed an interest in discontinuing substance use. 40 Mental health and substance use co-occurrence was more common among aging homeless women veterans than non-homeless women veterans, 35 with one study revealing a 30% co-occurrence rate. 18 Substance use, particularly when considered in combination with mental health conditions, is a vital consideration necessary to understanding the health and experiences of many aging homeless women.
Trauma experiences
The prevalence and impact of trauma experiences were explored and described in 6 of the 10 included studies, 17 –19,35,38,40 illustrating the insidious and lasting effects of diverse forms of trauma across the lifespan of many aging homeless women. It was clear that most women experienced some form of trauma at one or multiple points throughout their lives, 18 often in the form of interpersonal violence. In numerous situations, abuse and/or neglect were the factors that women believed meant the difference between remaining precariously housed and becoming homeless. The experience of trauma—which is often repeated and prolonged—in many ways shapes and informs current and future life experiences and overall health of aging homeless women.
Adverse childhood events
For many aging homeless women, the experience of trauma began in early life, with several having endured multiple forms of childhood abuse. Many aging homeless women have survived multiple childhood traumas, including childhood sexual abuse. 17 In one study, all aging homeless women veterans reported childhood abuse that ranged from verbal abuse, to physical violence, to prolonged sexual molestation, including with immediate and distant family relatives. Within this study sample, denial in the family surrounding the abuse was a common theme. For many of these women, their childhoods were unstable, having experienced the death of a parent or sibling, foster care involvement, or being moved from relative to relative throughout childhood. Several described childhood abuse or family upheaval as “normal,” 40 suggesting the ways in which the experience of childhood or early abuse may impact future health and life experiences.
Adult abuse
Abuse during adulthood represented a major issue related to the trauma experiences of many aging homeless women. Within one study, a majority (60%) of the 10 aging homeless women detailed a history of physical abuse within an adult relationship. 18 In addition, many aging homeless women described the threat of physical violence within the shelter. 18 Further, many felt vulnerable to physical and sexual abuse and, thus, are reluctant to utilize settings such as shelters. 19 As a result of real and perceived threats of violence, many aging homeless women remained hidden to service providers, which may impact health opportunities.
Sexual coercion
Sexual coercion, or sexual abuse, was another documented experience related to trauma experiences of many aging homeless women. Although discussed only minimally, sexual abuse, including sexual coercion, undoubtedly affects the lives of aging homeless women, including histories of “prostitution” endured by aging homeless women. 17 One study conveyed perspectives regarding sexual practices, indicating challenges in negotiating safer sex—specifically, condom use—for fear of “losing” a partner. 38 Two studies detailed the prevalence and impact of military sexual trauma, both reporting a majority of the sample having experienced sexual trauma while in the military, ranging from harassment to blatant sexual exploitation. 35,40 Experiencing military sexual trauma was significantly associated with being homeless, and aging homeless women veterans were more likely than their housed counterparts to have endured military sexual trauma. 35 No studies provided information regarding sexually transmitted infection rates, despite the demonstrated frequency of adverse sexual experiences, which may influence the accuracy of understanding of the sexual health risk of aging homeless women.
Social health
Findings pertaining to the theme of social health of aging homeless women were categorized into two domains: (1) familial and social dynamics (2) socioeconomic disadvantage.
Aging homeless women constitute a distinctly marginalized population 19 that experiences stigma at the intersection of sexism, ageism, and homelessness. 17 Certain social features uniquely contribute to the increasing number of aging homeless women, 19 related to familial and social dynamics and socioeconomic disadvantage.
Familial and social dynamics
Familial and social networks were of equally critical importance, operating both positively and negatively for aging homeless women. Many aging homeless women reported familial and social support, and a period before homelessness marked by prolonged reliance on external resources. 40 The role of the “nurturer” or “caregiver” was present across studies, which was found to be the central identity that helped aging homeless women to create a “valued sense of self.” 17 The support of friends and relatives aided many low-income, marginally housed women in avoiding homelessness for a time. 18 Once homeless, social connections with other homeless women operated as a support system. As two studies suggested, these social networks served as a source of mutual education, and information sharing regarding where to obtain meals, find shelter, and which places to avoid. 38,40
Conversely, many aging homeless women described the practice of associational distancing from other women, particularly within the shelter—separating themselves from the notion of being both “older” and “homeless.” 17 Two studies showed how aging homeless women experienced the dysfunctional aspects of familial and social relationships, detailing histories of disputes 19 and dysfunction within family units. 40 The majority of aging homeless women in their respective samples were single, separated, divorced, or widowed. 17,19,34,38,40 In one study, 90% of 100 women had children. 34 In another study, aging homeless women described how having children made the “biggest impact” on life, despite complicated relationships with these children. 17 Two separate studies shared how the women's tendency to nurture family and romantic partners caused trouble or enabled a level of relational dysfunction that ultimately led to their homelessness. 18,40 Although more aging homeless women than men had more relatives in their social networks who provided support, they also had more relatives with whom they experienced conflict. 36 Family fracturing, upheaval, and estrangement 17 from children, grandchildren, siblings, and other family members was common. Relationship problems, or disputes, were cited as a primary reason for homelessness. 18 Arguments with friends or family members, spousal abuse, family violence, and lack of social support accounted for up to 73.5% (164/223) of the major cited reasons for homelessness. 19 Social and familial networks, in many instances, served as a protective factor, but in others promoted remaining in marginal housing situations, thereby compromising housing security and health for aging homeless women.
Socioeconomic disadvantage
Socioeconomic disadvantage was a key topic of consideration in several of the included studies. The limitation of socioeconomic opportunities and its intersection with aging and health played a critical role for many women in both becoming and remaining homeless. Many women were single and living on fixed incomes, with 71% living at or below the poverty level and not well connected with benefits services. 19 Thirty-five percent of the 223 aging women in this study reported insufficient income as a major reason for homelessness. 19 In comparison to aging homeless men, aging homeless women were less likely to have achieved a high school education, and relatedly, had lower incomes. 36 Further, among aging women veterans, being unemployed was one of the strongest predictors of homelessness. 35 These persistent gender disparities translate into heightened socioeconomic vulnerability among women. 18 Although older homeless women relayed a desire to obtain employment, many experienced challenges in seeking and maintaining employment, citing physical health and age-related difficulties (e.g., balance/walking) as barriers. 38 Aging homeless women were often tasked with navigating complex socioeconomic circumstances, which may pervasively undermine both housing and health.
Spiritual health
Spiritual health was described as a key protective feature among aging homeless women. Findings pertaining to the topic of spiritual health were discussed in 3 of the 10 included studies, though this was not a central focus of any of the included articles. “[H]aving strength” and belief in a “higher power” was described as having critical importance to aging homeless women. 38 Many aging homeless women had less trust and faith in people, and more in the Lord, 17 and many aging homeless women emphasized the importance of spiritual beliefs, “looking up,” and believing “He's always with you.” 18 Altogether, these findings suggest the importance of spiritual beliefs as a source of strength for aging homeless women, which may be an underexplored protective factor that may facilitate resilience and support health in this population.
Discussion
The number of aging homeless women is steadily increasing. Synthesized evidence from this integrative review suggests that aging homeless women tend to fare worse than similarly aged non-homeless women. Aging homeless women experience a heavy burden of physical health conditions, complicated by elevated risk for progression associated with suboptimal nutrition, lower than expected cancer screening participation, and age-associated issues. In comparison to aging homeless men and non-homeless aging women, aging homeless women show drastically higher rates of mental health conditions, often complicated by the presence of substance use disorders. Early and often-sustained physical and emotional trauma, compounded by impaired social support, impacts the overall health of aging homeless women.
As women age in the United States, the number of low-income women increases, owing to many factors, including employment and health issues. Indeed, women are most at-risk for homelessness in their mid-50s, and there has been a dramatic increase in the number of older homeless women seeking shelter at night. 17 However, research throughout the past decade has primarily included and focused on women who are younger than 50 years of age and homeless. Many of these studies have demonstrated a noteworthy host of health concerns that are present during the midlife phase, which may be foretelling of the health of the growing population of aging women who are at-risk for homelessness and older homeless women. Physical health concerns among later midlife homeless women include an extremely high seroprevalence of herpes simplex virus 241 and trichomonas vaginalis, 42 and high rates of bodily pain contributing to activity limitations; behavioral health concerns, including high rates of stimulant use 43,44 and engagement in condomless sex 45 ; mental health concerns, including high rates of psychiatric conditions; and social health concerns, including disconcerting rates of emotional, physical, and sexual violence. 46 With the passage of time and the aging of the homeless population, the samples investigated in these studies have now aged into their 50s. However, as demonstrated in this integrative review, sparse follow-up research has been conducted among aging homeless women (age 50 years and older) to evaluate and address the aforementioned concerns or explore geriatric-specific physical or behavioral issues.
Indeed, results of this review reveal that chronic physical condition rates among aging homeless women are concerningly high, yet few data are available on specific physical condition diagnoses and preventive efforts tailored to the sex- and age-specific needs of this population. Although many contemporary studies focus on aging, there is a dearth of disaggregated sex-specific analyses regarding the impact of health conditions and the social determinants of health on older populations. 47 This deficit of sex-specific research may lead to service gaps for women and bias provider perceptions, 48 diagnosis, and treatment patterns, which can ultimately impact treatment outcomes, morbidity, and mortality. Greater focus is needed on the sex-specific manifestations of geriatric conditions in aging homeless women, such as frailty, cognitive impairments, and other functional impairments that progress in older age. Further, although mental health conditions are a prominent feature among aging homeless women, little is known regarding the prevalence, impact, and management of specific mental health conditions. More investigation is needed into the features and treatment of mental health conditions, such as depression and anxiety, with attention to the presence of co-occurring substance use disorders. Many of the studies documented noteworthy histories of multiple forms of trauma and its intersection with socioeconomic disadvantage; however, none represented a longitudinal analysis of the presence and/or impact of the trauma on the lived experiences of aging homeless women. Lastly, an understanding of how the social determinants of health influence physical and behavioral health outcomes of aging homeless women is imperative to leveraging protective factors and identifying effective health promotion strategies.
Implications for future research
Homelessness and housing research
Annually, the HUD point-in-time count estimates the number of homeless people living across the United States, which is believed to underestimate 49 the true magnitude of homelessness, particularly among women. Many low-income midlife and older women may be marginally housed and not self-define as “homeless.” Marginally housed people are a traditionally difficult-to-study population, 49 as it is challenging to count people who are provisionally sheltered, 50 or invisible from public spaces and typical homeless service sites. Although studies inside and outside of the United States generally find more homeless men than women, 51 this may reflect gender differences in the numbers of people most visibly homeless, inaccurately accounting for those who are doubled-up, couch surfing, staying in hotels, and staying in unsafe domestic situations. 52 It is, therefore, necessary to consider and count low-income marginally housed women at high risk for homelessness in future research.
Aging research, early aging and geriatirc conditions
Although the incidence of homelessness among aging adults is expected to continue rising, homeless policies and practices still largely focus on younger populations. 53 Owing to several factors, the onset of geriatric conditions 2 such as dementia occurs much earlier for homeless people. However, little is understood regarding the mechanisms by which this phenomenon occurs. Relatedly, preventive opportunities that could promote extended longevity and quality of life are not well understood. Future aging research should focus on historically underrepresented sub-groups of the aging homeless population, focusing on how to best delay the onset and provide better clinical management of geriatric conditions, including dementia, depression, and frailty. Further, future longitudinal analyses aging homeless women should focus on high-risk physical, behavioral, and social health issues, emphasizing the presence and impact of the trauma.
Mortality research
Though homeless people are on average three to four times more likely to die than non-homeless people, 54 no studies included in this integrative review addressed the risk for excess death among aging homeless women. In fact, although homelessness is considered an independent risk factor for death attributable to specific causes, 55 no U.S.-based studies have focused exclusively on mortality among homeless women, but rather they have focused on excess death seen in younger homeless populations. Existing research has demonstrated that leading causes of death among aging homeless women aged 65–84 years are: (1) cancer, (2) heart disease, and (3) diabetes, 56 which may be preventable and/or reversible if conditions are identified early and women are engaged in care. To equitably promote healthy aging and reduce the increased risk for mortality experienced by homeless women, preventive health opportunities should effectively target specific conditions or causes of death, 55 early in the aging trajectory. In so doing, the illness burden experienced by aging homeless women with potential disproportionate mortality risk may be addressed. Among aging homeless women, research into the rates and causes of death among homeless women is needed, with a focus on aging homeless women.
Implications for clinical practice
Women's health practice
Homeless women are at increased risk of injury and illness, though they are less likely to obtain needed health care services, including primary and preventative care services. 56 –61 As a result, pre-existing problems that were once more manageable with early intervention are likely to worsen. 62 Despite a heavy burden of cancer risk factors, 59 preventive screening uptake for women's health cancers remains suboptimal. Given below-average cancer screening rates and above-average cancer risk factors, 63 homeless women are often diagnosed with breast cancer at significantly later stages than non-homeless women. 64 Implementation of low-barrier, multidisciplinary point-of-care 65 interventions should be tailored to the needs of aging homeless women.
Geriatric practice and need for trauma-informed care
Aging homeless women disproportionately experience trauma, including high rates of physical and emotional abuse, high-risk sexual behaviors, along with mental health concerns and substance use disorders. Clinical care must be sensitive to age while focusing on trauma symptom recognition and integrating knowledge about trauma into assessments and plans. Guided by the framework of a trauma-informed approach, 66 employing a shared decision-making approach, 67 and leveraging clinical decision support tools, 68 clinicians should be equipped to offer substance use screening with aging homeless populations, and follow positive screens with brief interventions and referrals to treatment. 69
Limitations of the eligible studies
Despite the important contributions of the 10 level III studies identified in this review, there were a number of significant limitations, underscoring the need for future empirical studies. None of the studies utilized an experimental design. Methods of data collection largely relied on participant self-report, with some studies utilizing retrospective chart reviews. Self-reported data are often subject to social desirability bias and recall bias. 70 Further, studies that utilized provider/staff report (n = 2) 19,37 did not provide details regarding the sources from where data were obtained, the instruments used for data extraction, or the proportion of participant self-report versus provider report. In addition, some findings were limited by small sample sizes in quantitative and qualitative studies alike, which can affect generalizability and transferability.
Conclusions
Aging homeless women endure a disproportionate physical, behavioral, and social health burden compared with aging non-homeless women and aging homeless men. The paucity of published research in this area brings to light the need for large contemporary cohort evaluations of the age- and sex-specific health risk factors and characteristics of aging homeless women. Future research, clinical initiatives, and policy efforts must work in unison to develop opportunities for healthy aging, protect against the disproportionate impact of novel health threats, and extend quality of life among this socially vulnerable population.
Footnotes
Author Disclosure Statement
No competing financial interests exist for K.A.D., L.L.P., J.F., and S.J.B.. T.P.B. receives royalties from UpToDate for authorship of a topic review on homeless health care. S.E.L. has no competing financial interests for this article. Unrelated to this work, S.E.L. is a nonpaid board member of the nonprofit organization Healing Our Community Collaborative, Inc., Boston, MA, and has received one-time speaker fees from the Association of Nurses in AIDS Care in 2017 and 2019.
Funding Information
No funding was received for this article.