
Abstract
Background:
Intimate partner violence (IPV) is common, yet physicians do not routinely screen patients for IPV. There are no clear recommendations for best educational practices for physician trainees that improve screening rates.
Materials and Methods:
We implemented an IPV curriculum combining didactics and communication skills training for internal medicine residents. Didactics included definitions, risk factors, screening recommendations, and documentation; communication skills training included developing unique screening and response phrases; and two simulated patient exercises. The primary outcome was screening documentation rates as measured through pre- and postcurriculum chart review. Secondary outcomes included knowledge, comfort, and attitudes measured through pre- and postcurriculum administration of an adapted Physician Readiness to Manage Intimate partner violence Survey (PREMIS). Postcurriculum semistructured interviews provided further details regarding behaviors and attitudes.
Results:
Forty residents completed the curriculum. 29/40 (73%) completed both pre- and postsurveys. Fifteen participated in semistructured interviews. Residents demonstrated increased screening documentation postcurriculum (p < 0.05). Residents showed improvement in 80% of objective knowledge questions, and in all perceived knowledge and comfort-based questions (p < 0.01). Statistically significant improvement was noted in many attitudinal domains, including reported screening rates (p < 0.05). In the semistructured interviews, participants reported experiencing both practice-based improvements and ongoing screening barriers. Practice-based improvements included increased screening comfort and frequency, and strengthening of the doctor–patient relationship. Ongoing screening barriers included time, resistance to practice change, competing medical needs, and personal discomfort.
Conclusions:
A multifaceted IPV curriculum for residents significantly improved documentation rates, knowledge, comfort, and attitudes. Residents reported increased comfort with screening and strengthened patient relationships but acknowledged ongoing barriers to screening.
Introduction
Intimate Partner Violence (IPV) is an insidious and highly destructive public health problem. IPV, defined as physical or sexual violence, stalking behavior, and psychological aggression by an intimate partner, affects one-third of U.S. women in their lifetime. 1 Persons who experience IPV suffer higher rates of pregnancy complications, chronic health conditions, and mental health morbidity compared with those who do not. 2,3 Medical and mental health services for patients with an IPV history cost an estimated 10.4 billion dollars yearly. 4 Given IPV's significant morbidity and mortality, the United States Preventative Services Task Force (USPSTF) recommends screening all reproductive-age women for lifetime IPV exposure and providing appropriate resources. 5 When implemented effectively, screening identifies those experiencing IPV, and correlates with high rates of intervention use and relationship departures. 6,7 In light of the social isolation and increased stressors associated with the COVID-19 pandemic, violence screening is perhaps more important than ever. 8
Despite guideline recommendations and medical providers' acknowledgment of IPV as a clinically relevant issue, 9 providers do not routinely discuss violence with patients. 10 In a nationally representative sample, only 7% of women reported that they were ever asked about violence by a health care professional. 11 Physicians identify multiple barriers to IPV screening, including personal discomfort, lack of knowledge, and limited resource awareness. 12 Similar to practicing physicians, medical trainees report discomfort with violence screening and do not universally screen female patients for IPV. 13 Despite unease in the topic area, trainees deem violence education both important and relevant to their future practice. 14 Physicians of all levels desire IPV educational interventions with the potential to improve care for women experiencing violence.
Unfortunately, there is no guidance regarding educational strategies most effective in IPV training. 15 Trainees receive IPV instruction largely in didactic form, but desire practical applications including role play and group discussions of complex patient cases. 16,17 Prior work in trainee IPV education suggests that didactics-based curricula increase knowledge, and when combined with practical education, increase comfort and attitudes. 18 –23 However, there is little evidence that IPV educational interventions lead to behavior change or improved patient outcomes among medical trainees. 15
We developed an IPV curriculum for internal medicine (IM) residents combining both knowledge-based didactics and practical communication skills training. Our aims were to assess pre- and postcurricular changes in IPV (1) knowledge, comfort, and attitudes based on adapted survey measures; (2) screening documentation rates based on a chart review; and (3) perceptions and attitudes based on postcurriculum interviews. Our hypothesis was that a curriculum that developed practical skills in screening and response would lead to increased IPV screening documentation in the primary care setting. We also hypothesized that residents would show improved knowledge, comfort, and attitudes regarding screening and managing IPV in the primary care setting postcurriculum.
Materials and Methods
Study design
We employed both qualitative and quantitative methods to assess curriculum effectiveness. The quantitative portion was a pre–post study design consisting of a knowledge test, survey, and chart review of patient encounters. Semistructured interviews postcurriculum provided qualitative data on resident perceptions and attitudes. The study was approved by the University of Pittsburgh and Veterans Affairs (VA) Pittsburgh Health System Quality Improvement committees.
Setting and participants
The educational intervention occurred January through October 2019. Our participants were first-year residents in a required ambulatory medicine rotation within our university-associated academic IM residency program. Residents provided verbal consent for both the qualitative and quantitative portions of the study. Residents had the opportunity to opt out of research participation, however, all residents agreed to participate.
Curricular design
Our curriculum design was guided by prior IPV curricula at our institution, local expert recommendations, and literature review. 18 –23 Groups of three to six residents met in 3-hour sessions with a faculty member (J.K.) with experience in IPV and communication training. The educational session was divided into three parts: didactics, communication skills workshop, and simulated patient (SP) exercises (Table 1). The 1-hour didactic session included a general IPV overview, screening guidelines with supportive evidence, communication skills strategies as recommended by women who have experienced IPV, 24 and documentation. 25 Immediately following the didactics, residents participated in a 1-hour communication skills workshop in which they prepared responses to prompts and received feedback on word choice. Residents had the opportunity to develop their own unique verbiage, which is in line with adult learning principles (i.e., learner centered). 26 Finally, participants completed a 1-hour session with two cases for immediate skill application. Residents practiced IPV history taking and response with trained SP actors employed by our medical school. Cases were either developed specifically for this curriculum or were already in use at our institution. The faculty member guided the learners through the exercise using the “Primary Teaching Method” for coaching and feedback. 27 At the session's conclusion, each participant received a take-home packet, including a key IPV concepts fact sheet, communication skills guide, and local resource reference.
Curriculum Overview
IPV, intimate partner violence; USPSTF, United States Preventative Services Task Force.
Quantitative outcomes
We evaluated change in resident IPV knowledge, comfort, and attitudes by administering an adapted version (with author consent) of the Physician Readiness to Manage Intimate Partner Violence Survey (PREMIS), a previously validated scale intended to measure physician preparedness to effectively care for patients experiencing IPV. 28 We altered the knowledge and opinion questions to better reflect our curriculum didactic material (J.K., R.B., and M.A.M.). Residents completed the survey immediately before the curriculum and immediately after the 4-week ambulatory block. Objective knowledge was measured through seven multiple-choice and three true–false questions; residents' perceived (self-assessed) knowledge was measured through nine questions using a seven-point Likert scale (1, no knowledge to 7, know very much). Resident comfort in performing IPV-related skills in the clinical setting was measured through five questions with a seven-point Likert scale (1, not prepared to 7, quite well prepared). Attitudes on physician responsibility in IPV management, preparedness, and the patient's role were evaluated by 23 questions with a seven-point Likert scale (1, strongly disagree to 7, strongly agree). The survey included a demographic assessment of age, gender, medical school graduation year, and previous IPV training hours.
We assessed behavior change through chart review of screening documentation. We reviewed charts for all residents who completed the curriculum between January and June 2019, 4 months pre- and posteducational intervention. Residents from July to October 2019 were excluded, given they did not have any preintervention chart data. Our primary academic and VA sites were included in the analysis. Residents are evenly divided between the two clinic locations. All charts represented reproductive-age women (i.e., those deemed eligible by USPSTF guidelines 5 ) presenting for a new or annual visit to a resident physician who completed the curriculum. We reviewed new or annual visits in concordance with our recommendations for when to screen in the didactic session. We did not specifically review focused or sick visits as we encouraged residents to discuss violence in an unhurried manner (a known preference among patients who experience IPV) 24 and in the context of a patient's social history. We felt that this is best done during a wellness visit. Any mention of a discussion of IPV, domestic violence, or relationship safety within the current visit or acknowledgment of a past discussion was counted as documentation. The primary note reviewer (J.K.) was blinded to resident name, patient name, and whether note was completed pre- or postintervention. Each note was provided with a unique identifier code with a corresponding key for later decoding purposes (J.K. blinded to this process). Twenty notes were selected at random for coreview by an independent blinded reviewer (M.M.) with 100% concordance.
Qualitative outcomes
We further assessed resident comfort, attitudes, and reported behavior postcurriculum through semistructured interviews. Qualitative interviews gather rich detail regarding participant experience and opinions not captured by survey. 29 All curriculum participants were invited to complete an in-person or phone interview 4 weeks postcurriculum with a trained qualitative interviewer. Participants received a small financial incentive ($5 Amazon gift card) for their participation. The interview guide was developed with assistance of IPV and qualitative research experts (Supplementary Data S1). Interviews lasted ∼20 minutes, and addressed resident comfort with screening both pre- and postcurriculum, perceived barriers to screening, proposed action plans for responding to a positive screen, and overall curriculum reflections. We used probes where applicable to further elicit provider responses. Interviews were audiotaped and transcribed verbatim. Data analysis was performed iteratively using a content analysis approach. 29 Two authors (J.K., M.M.) independently coded all transcripts and met to adjudicate differences. Coding was examined for patterns in participant responses. The resulting content analysis was developed by the primary author (J.K.) and then shared with all authors for final agreement. We used ATLAS.ti version 8 (ATLAS.ti, Chicago, IL) to code all transcripts.
Statistical analysis
Descriptive statistics were computed to characterize the study participants. Frequencies and percentages were used for categorical measures; means and standard deviations (or medians in the case of skewed distributions) were employed for continuous variables. Changes in knowledge from pre- to postcurriculum were assessed using McNemar tests given the paired nature of the test questions. Changes in perceived knowledge, comfort, and opinion were analyzed using the Wilcoxon signed-rank tests; sign tests were alternatively employed when distributional assumptions of the Wilcoxon signed-rank test were not met. Chart review data were analyzed using Fisher's exact test. All statistical analyses were performed using STATA 15 (StataCorp, College Station, TX).
Results
Study participants
Forty first-year residents drawn from two residency classes (of 40 eligible residents) participated in the curriculum between January and October 2019. An average residency class in our program consists of ∼50 residents (excluding transitional and preliminary residents). The residents were 37% male and 60% female. All residents completed the presurvey (100%). Seventy-three percent completed the postsurvey (29/40), of which 31% were male and 69% were female. The median number of prior IPV training hours was two. The majority of residents (73%) graduated from medical school within the last calendar year. One hundred seventy-four total new or annual visit charts were reviewed for mention of IPV screening from both clinical sites (primary academic and VA). All participants were invited to participate in qualitative interviews. Fifteen residents agreed to participate and were interviewed; we completed 13 one-on-one interviews and 1 group interview of 2 participants. We did not assess demographic data for interview participants.
Our analysis included four major content areas: knowledge, comfort, attitudes, and behavior. Each will be discussed in turn with both quantitative and qualitative data included.
Change in knowledge
In our quantitative analysis, we assessed knowledge change in two domains: objective and perceived. There was statistically significant knowledge improvement in 4 of 10 questions (Table 2), and nonsignificant improvement in 4 additional questions. The two remaining questions revealed no change in pre- versus postcurriculum scores.
Residents Demonstrated Statistically Significant Improvement in Objective Knowledge in Four Key Topic Areas
p Values based on the McNemar test. Significant results (p < 0.05) in bold.
Perceived knowledge significantly improved in all domains posteducational intervention (Fig. 1). Notable areas of self-assessed knowledge improvement included legal reporting requirement awareness, strategies for medical record documentation, understanding of why a patient may not disclose an IPV history, resident role in detection and management, appropriate verbal response to a positive screen, and awareness of the natural history and stages in a relationship with IPV (all p < 0.01).
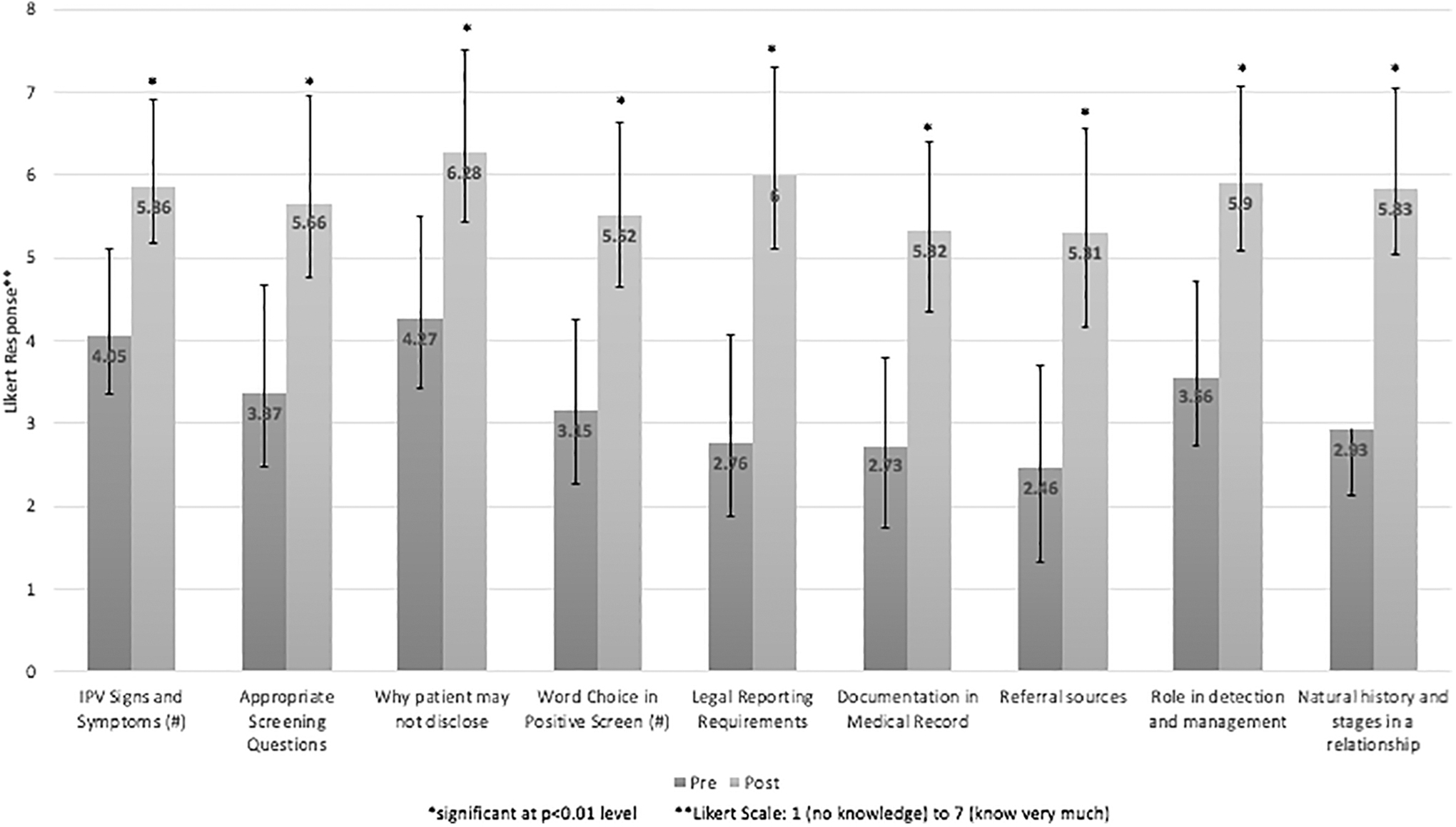
Residents demonstrated significant increase in perceived IPV knowledge postcurriculum. Numbers on bars represent mean Likert response both pre- (n = 40) and post- (n = 29) curriculum. Bar lines represent standard deviations. p Value based on the Wilcoxon signed-rank test. Sign test (#) employed when assumptions of the Wilcoxon signed-rank test not met. IPV, intimate partner violence.
Change in comfort
In our quantitative analysis, residents demonstrated significantly increased comfort regarding IPV communication skills postcurriculum (Fig. 2). Specific areas of increased comfort included asking appropriate questions, responding to positive screens, identifying violence red flags, medical record documentation, and making appropriate referrals (all p < 0.01).
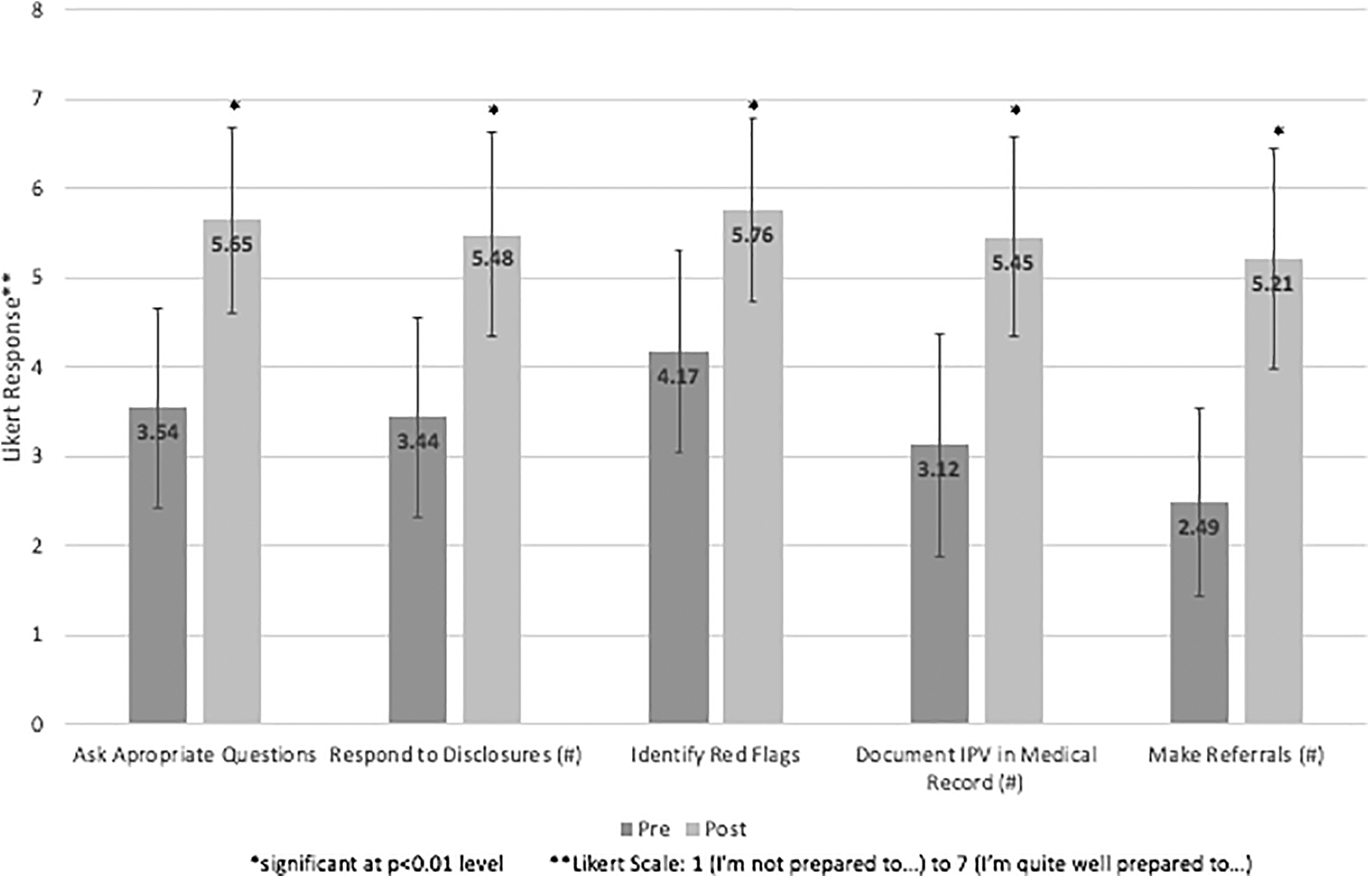
Residents demonstrated significant increase in comfort with IPV communication skills postcurriculum. Numbers on bars represent mean Likert response both pre- (n = 40) and post- (n = 29) curriculum. Bar lines represent standard deviations. p Value based on the Wilcoxon signed-rank test. Sign test (#) employed when assumptions of the Wilcoxon signed-rank test not met.
In the qualitative interviews, many residents expressed their increased comfort discussing violence with patients. They referred to comfort as a continuum, reflecting on their movement from complete discomfort, to feeling able to discuss and manage IPV with patients:
I'm comfortable asking the question rather than just speculate and wait until I get more clear signs…I think it's because I'm more comfortable asking the question—Interview 5
[The curriculum] helped me primarily be prepared to screen for [IPV]…My comfort level with training for it is very high now. My comfort level with actually managing it and responding to it probably started at zero and now it's maybe five out of ten—Interview 11
I think that I have the tools in my toolbox that I could use to screen. I think I have a better understanding of who I could ask, and who I could go to, and who could help find resources—Interview 9
Change in attitudes
In the quantitative analysis, residents demonstrated positive attitude changes regarding IPV (Table 3). Residents showed greater agreement that health care providers are responsible for asking all female patients about violence, that patients experiencing violence have the right to make their own decisions regarding possible interventions, and greater understanding of why individuals with an IPV history “do not always comply with (health care provider) recommendations.” 28 There was a nonsignificant increase in resident agreement that they had adequate time to ask about IPV and respond to patient's concerns about violence. However, residents strongly disagreed both pre- and postcurriculum that health care providers do not have time to assist patients experiencing IPV, or that they were too busy to participate in a team model to care for these patients.
Residents Demonstrated Improved Attitudes Regarding Their Role in Management of Intimate Partner Violence
Both precurriculum (n = 40) and postcurriculum (n = 29) results are included. Likert scale of 1 (strongly disagree) to 7 (strongly agree). *Denotes a statistically significant result with p < 0.05 based on the Wilcoxon signed-rank test or sign test (#) when assumptions of the Wilcoxon signed-rank test were not met.
In our qualitative analysis, residents reported that discussing violence strengthened the doctor–patient relationship. Regardless of whether the patient acknowledged experiencing IPV or accepted resources, residents felt that discussing violence and offering support was an important part of the physician's role. Residents felt they could be a trusted source of support for patients experiencing violence, both now and in the future, by establishing themselves as someone willing to discuss and manage difficult issues:
I felt I'm being an outlet to a patient who might be suffering from IPV. It also felt like I'm providing a safe space for them, maybe a solution…[by] making sure that's not the case. I feel like I'm opening doors to a patient who might feel [things are] closing down around them…we're another door for them to either reach safety or be the turning point for them to be in a safe relationship or safe environment—Interview 5
It shows that the doctor cares about these issues that might not seem medical at the surface but can really affect a person's life—Interview 12
Change in behavior
In the quantitative analysis, residents reported increased screening frequency postcurriculum. There was a statistically significant increase in reported IPV screening rates; residents moved from relative disagreement toward agreement that they ask all female patients about abuse and compliance with USPSTF screening guidelines (Table 3).
When asked about screening behaviors in the semistructured interviews (qualitative analysis), many residents acknowledged increased screening rates. They reported beginning to ask all female patients about violence at both new and annual visits:
I have become more deliberate about it…it's something at least on my new patient exam I have included…screening is something that I have started doing with all of my female patients—Interview 1
Residents also discussed beginning to ask about violence when red flag features were present:
I did have some experiences this month where I felt like it was an issue…and so I used some of the techniques we talked about. I would ask more directly if they feel like they have experienced physical, emotional violence from their partner—Interview 14
In addition to self-reported screening practices, we assessed objective changes in documentation rates postcurriculum (quantitative analysis). We reviewed 174 total charts of reproductive-age women presenting for a new or annual visit both pre- and postcurriculum from September 2018 to September 2019. First-year residents who completed the curriculum July 2019 to October 2019 were excluded from chart review analysis as we were unable to obtain preintervention data due to their early residency status. At our main academic site precurriculum, 1 visit out of 100 charts had a documented screen representing 1% of all visits (Table 4). Postcurriculum, 5 of 67 charts (7.5%) had a documented IPV screen, which was statistically significant increase (p = 0.039). Data from our VA site are detailed in Table 4.
Residents Demonstrated Increased Screening Documentation Postcurriculum at the Primary Academic Medicine Site, But Not at the Veterans Affairs Site
Charts of reproductive-age women (in accordance with USPSTF guidelines) presenting for a new or annual visit to a resident who completed the curriculum were reviewed. “Pre” refers to 4 months precurriculum to the resident's curriculum date. “Post” refers to the 4 months following the curricular intervention. * p < 0.05 based on Fisher's exact test.
VA, Veterans Affairs.
While residents reported increased screening and demonstrated small but significant documentation increases, they acknowledged multiple barriers that may have limited screening implementation in the semistructured interviews (qualitative analysis). The most common reasons for not screening included inadequate time in clinic appointments, lack of incorporation into their usual routine, primacy of other patient issues, and personal discomfort. In regard to time, residents reported that delayed or omitted screening was primarily due to inefficiency and patient tardiness. This was not unique to IPV but included other elements of the social history as well. One resident stated,
It's kind of hard to incorporate a lot of history when I'm seeing patients because they're scheduled for an hour session, but they come thirty minutes late or I have other patients that I've been seeing and then running behind so that makes it hard—Interview 2
They also acknowledged not remembering to screen for IPV because it was not already part of their usual routine in outpatient visits, and they had yet to make a change in their practice:
Part of it is that even the sort of brief period of time that I've had over the past year to kind of build up a practice and how I approach a new patient…it's hard to change the structure in a meaningful way—Interview 9
Residents felt that screening may be enhanced by small in-clinic changes, such as incorporation into electronic medical record. One resident had already independently included a screening prompt into her template for new patient visits:
I tried in the annual exam [of] said new patients. And then I found that…I just didn't remember to always screen…I have…a note template that I just use to prep myself and I have a women's health screening section. I just put IPV screen in there as a reminder to myself, which helped—Interview 4
Residents cited other patient concerns as trumping routine screening and social issues. While they acknowledged the importance of IPV screening, they felt that there were many competing medical issues that necessarily took precedence:
Screening itself sometimes gets overlooked…by other medical issues. [It has] nothing to do with the patient or whether it's a topic I'm comfortable with or not because I'm very comfortable with it, and I feel it's something very important to talk about. But unfortunately, it's just due to the matter of dealing with other medical issues that I'm focused on, because they're more pressing at the moment rather than the overall picture—Interview 5
Finally, despite reporting increased comfort after completing the curriculum, residents continued to acknowledge unease in asking about IPV. They continued to report feeling “awkward” and unsure about phrasing, and so sometimes avoided addressing violence with patients. They did however feel that with practice and time these skills would improve:
It's kind of awkward for me to ask some of these kinds of questions so I just need to get more practice at that part—Interview 2
Discussion
We found that an IPV curriculum combining knowledge-based didactics and practical communication skills training improved resident knowledge (both objective and perceived), comfort, attitudes, and screening rates.
Residents demonstrated statistically significant improvement in both objective and perceived knowledge. Residents demonstrated improved scores in 8 of 10 knowledge questions, 4 of which were statistically significant. These four topic areas represented knowledge essential in harm reduction with the capacity to save lives. Knowledge gains represented sustained learning as the post-test was completed 4 weeks after the educational intervention. In addition, trainees reported significant improvement in perceived knowledge increasing their likelihood of appropriately addressing IPV going forward.
This is further suggested by the fact that resident comfort and attitudes regarding IPV were significantly improved postcurriculum. Residents demonstrated greater confidence in their ability to screen patients for IPV, respond to positive disclosures, document appropriately in the medical record, and make referrals. They felt that IPV screening was an important part of the physician's role, strengthened the doctor–patient relationship, and would be an ongoing part of their practice. While residents did acknowledge some ongoing discomfort as a screening barrier, they were hopeful that further practice would beget greater comfort, opening the door for further educational opportunities to solidify principles and best practices.
Screening rates were significantly improved by resident self-report and documentation. Residents reported greater compliance with USPSTF screening guidelines and higher violence discussion rates with patients. IPV screening documentation rates at our primary academic site were significantly increased, although our numbers were small. There was a nonsignificant trend toward increased screening at our VA site, which was limited by small female patient census. There are multiple possible reasons why residents may report increased screening but fail to document. Our curriculum extensively discusses the pros and cons of documentation, and strongly recommends that residents not document the discussion if the patient objects or if there are safety concerns. Confidential and non-electronic medical record-based IPV documentation was reviewed. If a resident did not document screening, we are unable to assess whether screening was not completed, screening was completed but not documented, or whether a positive screen was not documented in readily available notes due to safety concerns.
Our study has several notable strengths. To our knowledge, our study is the first to demonstrate improved IPV documentation rates among IM residents. Prior studies among trainees have shown improved documentation rates among pediatrics residents through a multipronged approach (didactic sessions, screening clinical reminders, and on-site counselors) 30 or improved screening through subjective patient report. 21 While many prior curricular interventions address knowledge acquisition, our study demonstrates improvement in multiple outcome domains. Our study also employs a highly structured educational intervention easily adaptable to a variety of learner levels. Finally, our study supports previously identified screening barrier themes such as time, personal discomfort, and the competing demands of other patient medical issues. 12,31
Our study has several limitations. First, the use of unvalidated questions limits our knowledge assessment and may suggest higher baseline knowledge than truly exists. Second, our study does not include a clinical intervention. Prior successful studies among practicing physicians have involved both educational and clinical components to encourage ongoing uptake and screening beyond a single-day curricular intervention. 15 Third, documentation is at best a surrogate marker of actual screening. Our analysis was not able to capture patients screened without subsequent documentation, and actual screening rates pre- and postcurriculum may have been higher. Fourth, our curriculum prominently features SP work, which may be unattainable or financially impossible for other programs interested in implementing this curriculum. Fifth, all curricular sessions were led by a single facilitator, which may limit the curriculum's transfer to other settings. However, our use of a single instructor offered consistency across all sessions, and we believe the content could be successfully delivered by other educators. Sixth, it is notable that residents were two-third female and one-third male. The gender distribution of the residency program is approximately equal between men and women. Since the curriculum was required, the participant gender distribution reflects random schedule assignment and not variable curriculum uptake based on gender. Finally, we acknowledge that the small female population seen by residents at our VA site limits our ability to assess those participants' transferred skill as measured by documentation rates.
Our study suggests many opportunities for future work. Combining our educational intervention with a clinical intervention may facilitate repeated resident topic exposure and greater support for ongoing practice change. Inclusion of IPV screening in resident note templates and faculty-prompted reminders may lead to improved resident documentation rates. To address perceived and actual time burden, staff prescreening and consistent inclusion in previsit questionnaires across sites may allow residents to triage more extensive violence discussions to those deemed of highest need. As our increase in documentation rates was notably small, more systematic changes within the clinic environment to support violence discussions and patient support may be more crucial than change at the individual provider level. Our residents also desired further practice to continue to develop confidence and skill. This can be supported through spaced lectures, skills-based practice opportunities, focused work with an IPV specialist or domestic violence shelter, or deliberate practice.
Conclusions
IPV is a critically important health determinant in our patients, yet often missed by health care providers. An IPV curriculum combining knowledge-based didactics and practical communication skills training improved knowledge (both objective and perceived), comfort, attitudes, and screening rates.
Footnotes
Acknowledgments
We thank the authors of the PREMIS scale for their agreement with adaptation of the survey for our educational and research purposes. We also thank the staff of Qual EASE at the University of Pittsburgh, particularly Flor de Abril Cameron, for interview support and transcription services for the qualitative portion of the project. We also thank the University of Pittsburgh Medical Center Internal Medicine Residency program, the Division of General Internal Medicine, the VA Pittsburgh Health System Simulation Center, and the University of Pittsburgh School of Medicine Standardized Patient program for their participation and support.
Authorship Confirmation Statement
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in the Journal of Women's Health. J.K., M.A.M., M.H., R.B., and S.R. conceived and designed the study. J.K. and M.M. participated in data acquisition. J.K., M.H., and S.R. analyzed and interpreted the data. J.K. drafted the article with significant revisions for important intellectual content by M.A.M., M.H., R.B., and S.R. All authors reviewed the final article before publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was funded locally by the Thomas H. Nimick, Jr. Competitive Research Fund, and the University of Pittsburgh Division of General Internal Medicine Fellow Award. Financial compensation for simulated patient actors was generously provided by the VA Pittsburgh Health System.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.