
Abstract
Objective:
To assess whether evidence-based information on progestin-only pills (POPs) and over-the-counter (OTC) oral contraceptives (OCs) increases support among clinicians for bringing a POP or combined oral contraceptive (COC) OTC and to identify concerns clinicians may have about OTC access to OCs.
Materials and Methods:
In 2018 a survey of 778 clinicians assessed support for bringing a POP and COC OTC before and after receiving evidence-based information, which was pretested through in-depth interviews. Clinicians were randomized into two groups, stratified by clinician type. One group received information about OTC access to OCs generally, and the second group received OTC information plus information about POPs. Levels of support between arms were compared using robust Poisson models.
Results:
Before receiving information, 31% of clinicians supported moving a POP OTC. After receiving information, 39% of clinicians who only received OTC information supported moving a POP OTC compared to 61% who received OTC and POP information (relative risk = 1.53, 95% confidence interval: 1.34 to 1.75). Support for bringing a COC OTC increased marginally for those who received OTC and POP information, while support among those who received only OTC information increased by 12 percentage points (to 50%). Among clinicians opposed to moving a POP OTC after receiving information, top concerns included safety (26%), effectiveness (19%), potential for incorrect use (19%), and loss of preventive screenings (15%).
Conclusion:
Evidence-based information, particularly around POPs, has the potential to change clinician attitudes and address misconceptions about POPs and OTC access.
Introduction
Oral contraceptives (OCs) are the most common, nonpermanent method of birth control in the United States 1 ; however, research indicates that the prescription requirement for hormonal contraceptive pills may be a barrier to use due to gaps in insurance coverage, 2 cost barriers, 3 and challenges accessing a provider. 3 Making OCs available over-the-counter (OTC) could expand contraceptive access for individuals who face barriers in accessing a prescription OC and could potentially lead to higher rates of OC initiation 4,5 and continuation 6 and lower rates of unintended pregnancy. 7,8
A progestin-only pill (POP) is likely to be the first formulation approved for OTC use in the United States due to a lower prevalence of contraindications compared to combined oral contraceptives (COCs) 9 and the Food and Drug Administration's (FDA) prior approval of an OTC progestin-only emergency contraception. Although current use of POPs in the United States is low, 10 there is interest in using an OTC POP; in a 2015 nationally representative survey, 39% of U.S. adult women at risk of unintended pregnancy and 29% of young women aged 15–17 said that they were likely to use an OTC POP after reading a description of the product. 11
Health care providers are key stakeholders in an effective rollout of an OTC OC because they are trusted by the general public. Although there is wide support among prominent professional medical associations for making an OC available OTC, including from the American Academy of Family Physicians, 12 the American College of Obstetricians and Gynecologists, 13 and the American Medical Association, 14 previous research has suggested that clinicians in practice hold mixed opinions on the issue. A 2009 survey of 482 physicians, advanced practice clinicians, and registered nurses found that 28% supported bringing an OC OTC. 15 In 2012, a survey of 638 obstetrician-gynecologists (OB/GYN) and family medicine residents assessed opinions about OTC access of POPs and COCs. Almost half (48%) of surveyed residents supported moving a POP OTC, while 29% supported an OTC COC. 16 Those opposed to an OTC COC cited safety as their primary concern (93%). Among the 52% opposed to bringing a POP OTC, 70% named safety as their primary concern, despite the strong safety profile of POPs. This may indicate a high prevalence of misconceptions about POPs or a lack of knowledge about this particular formulation of OC.
As the current primary prescribers of OCs and influential voices in the scientific community, understanding clinicians' opinions of bringing a POP and COC OTC and addressing concerns that may underlie these opinions are essential. We therefore conducted a survey to understand clinicians' opinions of bringing a POP and COC OTC and to assess the impact of evidence-based information on support for bringing a POP and COC OTC by randomizing the information that clinicians viewed. We hypothesized that providing evidence-based information on the data supporting moving an OC OTC and specifically about a POP would increase support for moving a POP OTC. We also aimed to assess opinions about POPs as a method of contraception.
Materials and Methods
We surveyed U.S. health care clinicians on their opinions, attitudes, and knowledge of POPs and of bringing a POP and COC OTC. Primary care physicians, OB/GYNs, nurse-midwives, nurse practitioners, and physician assistants who prescribed contraception to women of reproductive age at the time of the survey and saw at least one patient per week in office or clinic visits at the time of the survey were eligible to participate in the study. Specialties of those identifying as primary care physicians could not be obtained for the full sample, but materials provided by Epocrates indicated primarily internal medicine and family medicine specialties among primary care physicians. The survey was fielded with clinicians enrolled in Epocrates's market research database, HCPView, a database including over 1.4 million health care professionals. Clinicians included in the panel opt in to participate in research and receive incentives for participation.
Clinicians who were invited to take part in the survey received the study topic—“healthcare providers' perspectives regarding progestin-only oral contraceptives and moving a progestin-only contraceptive over the counter”—before consenting to participate. The clinicians who consented to participate in the survey and met inclusion criteria were randomly assigned to one of two groups using the survey software; the first group received information about OTC access to OCs generally (the “OTC information” group), and the second group received this same OTC information plus information about POPs specifically (the “OTC and POP information” group). Randomization was balanced by clinician type; a 1:1 randomization was conducted within strata of clinicians. Clinicians first answered questions about the profile of contraceptive clients they saw and their support for moving an OC OTC. If they did not voice support, they were asked to provide reasoning as to why they did not support moving a COC and/or POP OTC, unprompted by prespecified options. Clinicians then saw the evidence-based information according to the arm to which they were randomized (Table 1). One message was shown per page.
Evidence-Based Information Given to Clinicians During Survey
The table mimics the text viewed by clinicians in the survey, including the references cited.
COC, combined oral contraceptive; FDA, Food and Drug Administration; LARCs, long-acting reversible contraceptives; OC, oral contraceptive; OTC, over-the-counter; POP, progestin-only pill.
After seeing evidence-based information, clinicians were asked to compare COCs to POPs. For this question, clinicians could choose from the following options: “when used as directed, combined oral contraceptives and progestin-only pills have the same effectiveness at preventing pregnancy,” “combined oral contraceptives are more effective at preventing pregnancy than progestin-only pills,” or “progestin-only pills are more effective at preventing pregnancy than combined oral contraceptives.” Clinicians were then asked “In light of the messages you read on over-the-counter access to oral contraceptives, do you support bringing any of the following oral contraceptive products over the counter?” If they were not supportive of moving a COC or POP OTC, clinicians were asked to identify their concerns with moving an OC OTC from a list of options (safety, loss of income for providers, impact on provider–patient relationship, less effective pill formulation, concern that women will no longer come in for preventative screenings, loss of counseling on other contraceptive options, potential for incorrect use of method, cost to patient, unfamiliar pill formulation for users, side effects of product, or other). If they chose more than one concern, they were asked to identify their top concern. All clinicians were asked an open-ended question at the end of the survey about what additional information they would like to have about moving an OC OTC. The survey also covered a number of sociodemographic, workplace, and clinician characteristics.
Clinicians were asked about their support for moving a POP and COC OTC by answering the following question “Do you support bringing any of the following oral contraceptive products over the counter?” Clinicians could select multiple options from the following list of answers: “yes, a combined oral contraceptive,” “yes, a progestin-only oral contraceptive,” “no, I don't support bringing either of these products over the counter,” or “unsure.” Clinicians who answered they were “unsure” if they supported bringing a pill OTC were considered not supportive; however, clinicians who selected unsure were not asked to identify concerns with moving the OC OTC.
Information displayed in the survey was developed using academic literature (references cited in Table 1) and tested through in-depth interviews with 11 clinicians recruited through the Association of Reproductive Health Professionals listserv before fielding of the survey. Through these interviews, we aimed to understand clinicians' top concerns about moving an OC, particularly a POP, OTC, and test information developed to respond to clinicians' concerns identified by previous research. The information included in the survey was adapted based on feedback from these formative interviews for inclusion in the survey instrument.
With a sample of 778 clinicians, 389 in each of the control and intervention arms, we estimated that we had 80% power to assess a difference of 10 percentage points in support for an OTC POP with a 95% confidence interval (CI) ±5%.
We tested whether clinicians in the OTC and POP information group had different levels of support toward bringing a POP or COC OTC than the group who received only OTC information. We ran two robust Poisson models to allow for the estimation of relative risks (RRs). 17 –20 In the first model we controlled for baseline support to increase precision of the estimate. 21 We also performed a secondary analysis controlling for the following clinician characteristics, which were identified a priori 22 as potentially affecting support of a OTC OC as documented in prior literature 15,16 or due to the research team's hypotheses: clinician type (primary care physician, OB/GYN, nurse-midwife, nurse practitioner, physician assistant), gender, number of years in practice, practice type (academic facility, public hospital, or private practice/private hospital), practice location (urban vs. not urban), region of country (Northeast, Midwest, South, West), percent of contraceptive patients prescribed long-acting reversible contraceptives (LARCs; categorical variable defined at quartiles), percent of contraceptive patients prescribed OCs (categorical variable defined at quartiles), and percent of patients with Medicare and private insurance (both categorical variables defined at quartiles). We present a RR, or relative change in probability, of supporting moving a given pill type OTC. We also calculated the difference in the proportion of clinicians supporting moving a given pill type OTC among the group of clinicians that received both OTC and POP information compared to the group receiving just OTC information using model estimates and the mean of the observed covariates.
At baseline, we ran Chi-square tests to test for differences in support for bringing a POP, COC, or either a POP or COC OTC by clinician characteristics. We descriptively analyzed reasons given for not supporting bringing a POP and a COC OTC separately among those who were not supportive both before and after information was presented. Open-ended questions were coded by one member of the study team. A codebook was developed iteratively throughout the coding process. Thirteen percent of responses were double coded by another researcher, and any discrepancies were discussed until consensus was reached. Overall frequencies of codes are presented. After information was presented, we compared the top reasons selected for not supporting moving a POP or COC OTC by randomization group. These concerns, as well as opinions about POPs, were compared descriptively and through Chi-square tests.
Analyses were conducted using Stata 15 SE (Stata Corp., College Station, TX) and R (R Core Team, Vienna, Austria). This study was approved by Allendale Investigational Review Board.
Results
The survey was fielded from August 15 to 23, 2018. Approximately 18,560 clinicians were contacted to participate (response rate ∼5%), and of those that agreed to participate, 84% were eligible to participate. A total of 779 clinicians completed the survey. One survey was excluded from the analysis as the clinician identified as being mostly retired. Our final sample included 778 clinicians.
Just under half (42%) of the sample identified as primary care physicians, 24% identified as OB/GYNs, 13% as nurse practitioners, 12% as physician assistants, and 9% as nurse-midwives (Table 2). Over half of the sample identified as female (56%), and most clinicians were between the ages of 36–65. There was a distribution of experience in practice among the sample. Most commonly, clinicians reported that their patients had private insurance followed by Medicaid or other public insurance. On average, clinicians reported that <10% of their patients were uninsured. The majority of clinicians reported prescribing OCs most often, followed by LARCs and other contraceptive methods. The sample had representation from all regions of the country, with the most respondents coming from the South (38%) followed by the West (23%). Three hundred eighty eight clinicians were randomized into the OTC information group, and 390 were randomized into the OTC and POP information group. The two randomized groups had good balance on most characteristics with the biggest differences by percentages observed by practice location, and region.
Characteristics of Clinicians, by Study Arm (over-the-Counter Information Only or over-the-Counter and Progestin-Only Pill Information), N = 778
Not exclusive options.
OB/GYN, obstetrician-gynecologist.
Before receiving information, support for bringing a COC OTC was higher than for a POP across the full sample (38% vs. 31%) (Table 3). Twenty-two percent of the sample supported moving both a POP and COC OTC, while 9% of the total sample supported moving a POP OTC and not a COC OTC while 16% supported moving a COC OTC while not supporting moving a POP OTC. Those more likely to support OTC access of a COC or POP tended to be clinicians who: were nurse-midwives, younger (ages 27–45), worked in an academic setting or in a public hospital, saw more patients with Medicaid, prescribed LARCs to a larger proportion of their contraceptive patients, and prescribed OCs to a fewer proportion of their contraceptive patients. Support for OTC POPs in particular was strong among nurse-midwives (63%), compared to 19% of physician assistants, 22% of nurse practitioners, 27% of primary care physicians, and 36% of OB/GYNs, as well as among older clinicians (65+) and female clinicians. Unlike other clinician types, OB/GYNs had similar levels of support for both formulations.
Support for an over-the-Counter Progestin-Only Pill, over-the-Counter Combined Oral Contraceptive, or Either an over-the-Counter Progestin-Only Pill or over-the-Counter Combined Oral Contraceptive Before Information, by Clinician Characteristics, N = 788
p-Values represent results from chi-square tests comparing support for the outcome given in the column. For nonexclusive categories, chi-square tests were performed on each category separately.
n = 765.
Other insurance not included because 86% of respondents reported no patients with other insurance types.
Not exclusive options.
Before receiving information, clinicians who did not support bringing either a POP and/or COC OTC reported a variety of reasons for their opposition to OTC access. Among clinicians who did not support bringing a POP OTC at baseline (n = 412), top listed concerns were: safety (46%), potential for incorrect use of method (19%), less effective pill formulation (17%), side effects (15%), and loss of preventative screening (8%; results not shown). Among clinicians who did not support bringing a COC OTC at baseline (n = 354), 81% said that they were concerned about safety, 14% were concerned about potential for incorrect use of the method, 12% were concerned about potential negative side effects, and 8% were worried about loss of preventative screening.
Information provided increased support for OTC access of both POPs and COCs, although increases in support varied depending on whether the clinician received OTC information alone or both OTC and POP information (Fig. 1). Support for bringing a POP OTC increased by 29 percentage points in the group that received both OTC and POP information, from 32% at baseline to 61% after information was presented. Among the group that received only OTC information, support for bringing a POP OTC increased by 9 percentage points, from 30% to 39%. Support for bringing a COC OTC increased by 2 percentage points among the group that received OTC and POP information, from 38% to 40%, while support for bringing a COC OTC among those who only saw OTC information increased by 12 percentage points, from 38% to 50%.
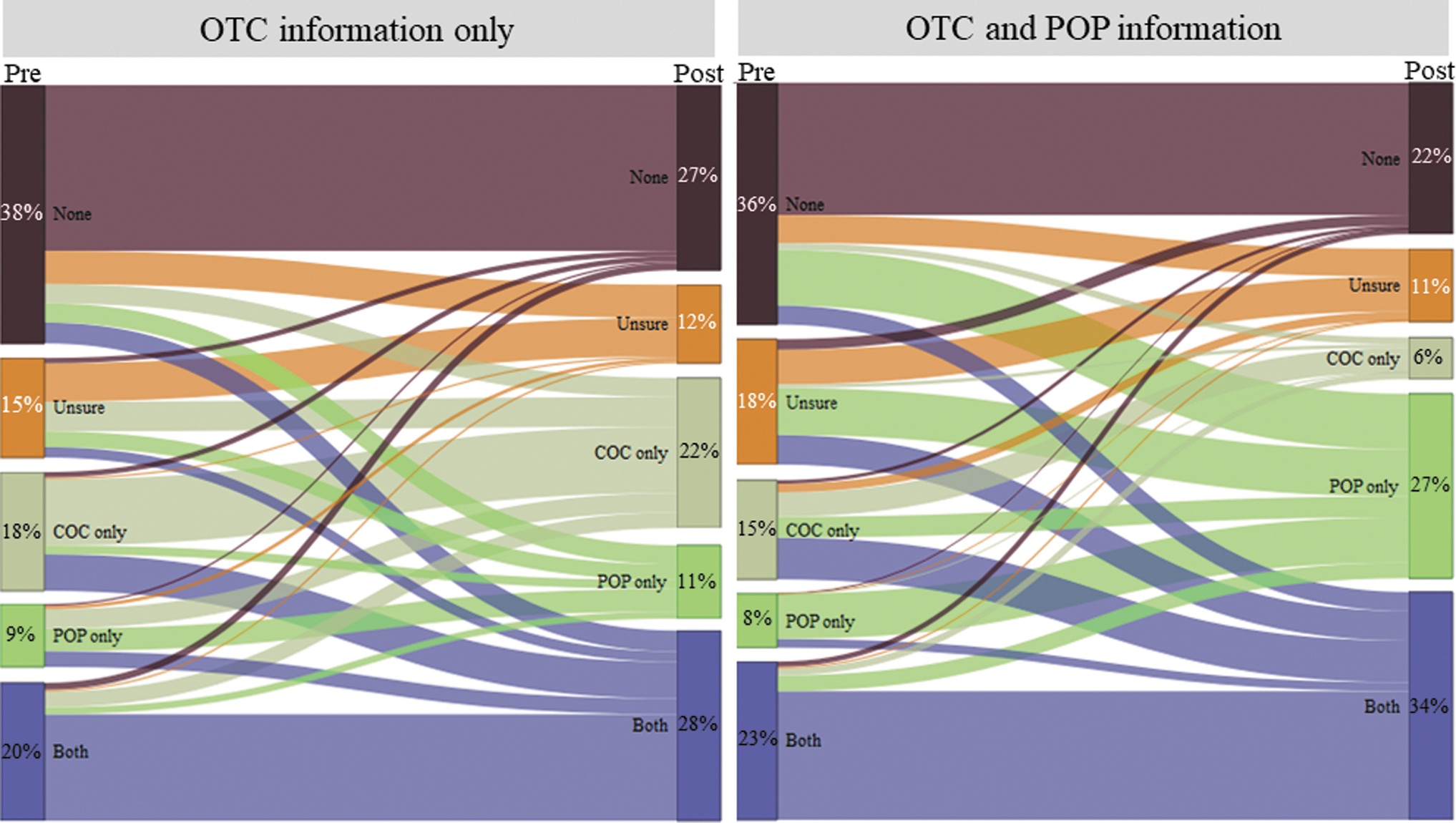
Support for an OTC POP and OTC COC before and after evidence-based information. Percentages reflect the percentage of clinicians in each arm that did not support any pill moving OTC (none), were unsure, supported only a COC (COC only), supported only a progestin-only contraceptive (POP only), or both a COC and a progestin-only oral contraceptive (both). The size of the lines represents the proportion of clinicians. COC, combined oral contraceptive; OTC, over-the-counter; POP, progestin-only pill.
In the first model examining support for bringing a POP OTC controlling for baseline support, the group that received OTC and POP information was 53% more likely (RR = 1.53, 95% CI: 1.34 to 1.75) to support bringing a POP OTC after receiving information, compared to the group receiving only OTC information, translating to a difference of 0.21 in the proportion of clinicians supporting moving a POP OTC in the OTC and POP information group compared to the OTC only information group (95% CI: 0.15 to 0.28). In the first model examining support for bringing a COC OTC, the group that received OTC information alone were more likely to support bringing a COC OTC after receiving information compared to the group receiving OTC and POP information (RR = 0.79, 95% CI: 0.70 to 0.90). In our first model examining support for bringing either a POP or COC OTC, the group that received OTC and POP information was 11% more likely to support moving either a POP or COC OTC compared to those who only received OTC information alone (RR = 1.11, 95% CI: 1.02 to 1.21), translating to a difference of 0.07 in the proportion of clinicians supporting moving either a POP or COC OTC in the OTC and POP information group compared to the OTC only information group (95% CI: 0.01 to 0.12). However, lower estimates of the effect approached zero. Across all three outcomes, models that included covariates identified a priori changed estimates only slightly; however, the RR comparing probability of support for either a POP or COC OTC between study arms was no longer significant (Table 4).
Unadjusted and Adjusted Relative Risk and Difference in Support Between Clinicians Who Received over-the-Counter and Progestin-Only Pill Information Versus Clinicians Who Received Only over-the-Counter Information (N = 778)
RRs represent the relative probability that the group who received the OTC and POP information supports the given outcome (either a POP or COC, a POP, or a COC) compared to the group who received only OTC information. The difference reported represents the estimated difference between the proportion of clinicians that support the given pill type moving OTC in the group that received OTC and POP information and the group that received only POP information (E[Y2] − E[Y1]) where 2 represents having received both OTC and POP information and 1 representing only having received OTC information.
Adjusted for clinician type (primary care physician, OB/GYN, nurse-midwife, nurse practitioner, physician assistant), gender, number of years in practice, practice type (academic facility, public hospital, private practice, or private hospital), practice location (urban vs. not urban), region of country (Northeast, Midwest, South, West), percent of contraceptive patients prescribed LARCs (categorical variable defined at quartiles), percent of contraceptive patients prescribed OCs (categorical variable defined at quartiles), and percent of patients with Medicaid and private insurance (both categorical variables defined at quartiles).
RR, relative risk.
Respondents who indicated that they did not support moving a POP (n = 303) and/or COC OTC (n = 341) after viewing the information were asked to pick their top concern (Fig. 2). Clinicians most commonly cited safety, which was chosen by 55% of those not supporting an OTC COC and 26% of those not supporting a POP OTC. Among clinicians opposed to an OTC POP after viewing information (n = 303), top concerns after safety were less effective method (19%) and the potential for incorrect use of the method (19%). This was followed by loss of preventative screening (15%) and loss of counseling on other contraceptive options (8%). Among clinicians opposed to an OTC COC after viewing information (n = 341), the most cited top concerns after safety were potential loss of preventative screening (15%), potential for incorrect use (10%), potential side effects (8%), and loss of counseling on other contraceptive options (6%).
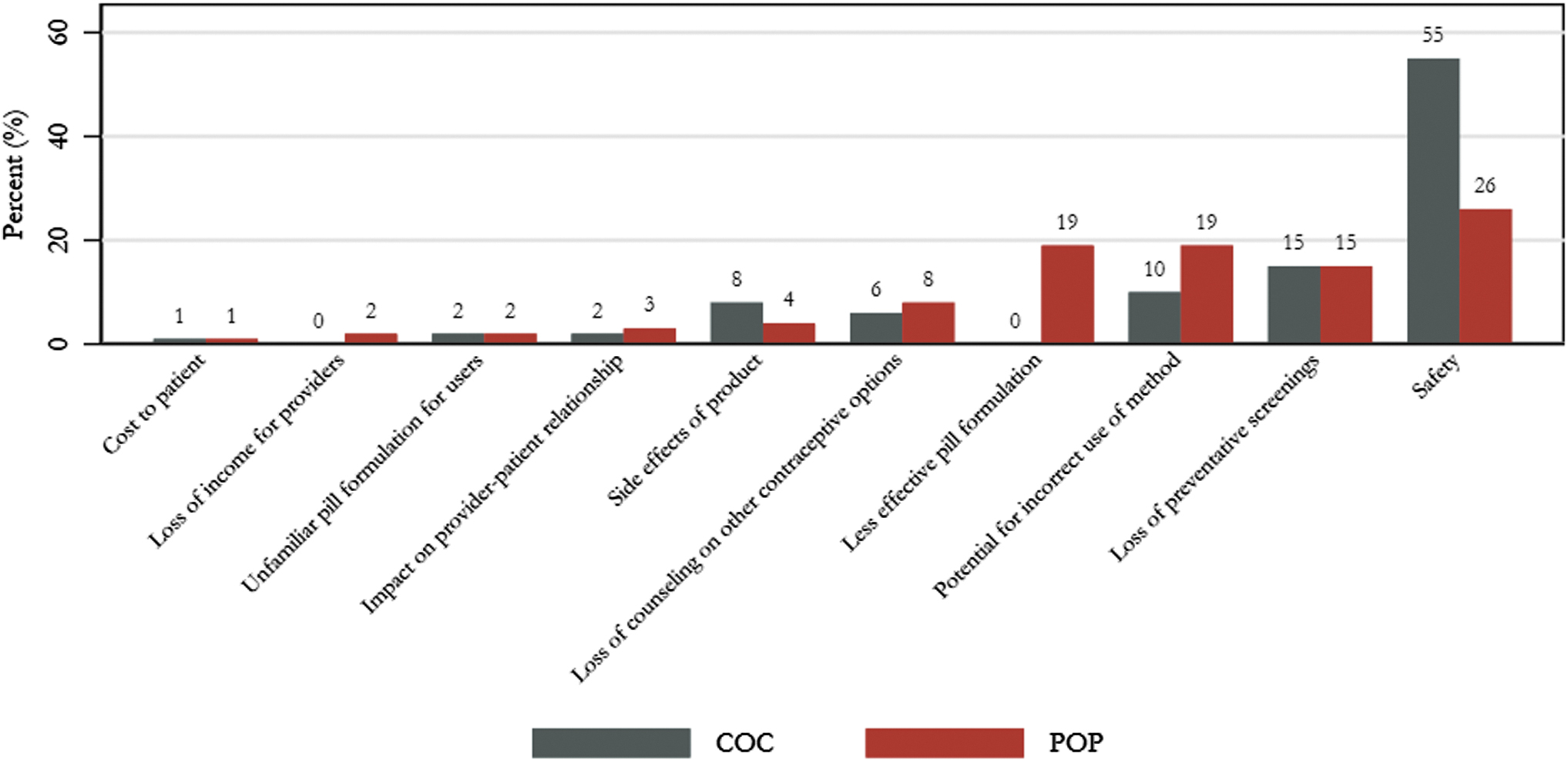
Top concerns about moving a COC and/or POP OTC. Percentages reflect the percentage of clinicians reporting the item who do not support moving a POP or COC OTC, respectively, after viewing information.
There were minimal differences in the prevalence of top concerns about moving a COC OTC by study arm. Descriptively, prevalence of the top concerns about moving a POP OTC differed by arm; however, these differences were not statistically significant. Those who received both OTC and POP information were less concerned that a POP would be a less effective method (14% in this group selected this reason as their top concern compared to 22% in the OTC information only arm); however, those who received OTC and POP information were more concerned that women would no longer come in for preventive screening (22%) than those who received OTC information (11%), a concern not unique to POPs. Both arms were equally concerned about safety (26% in the OTC information group and 28% in OTC and POP information group) and potential for incorrect use (20% in OTC information group and 16% in OTC and POP information group).
Clinicians' opinions on how COCs compared with POPs differed by arm (Table 5). When asked “How would you compare combined oral contraceptives to progestin-only pills?,” 60% of those who received OTC and POP information answered that when used as directed, COCs and POPs have the same effectiveness, compared to 47% of those who received OTC information alone (p < 0.001). After reading the information, there was a general appetite among clinicians for more information on the safety (n = 111), potential cost (n = 69), label (n = 64), data to support moving a pill OTC (N = 64), and potential restrictions for an OTC OC (n = 44).
Knowledge Related to Progestin-Only Pills After Information, by Study Arm (over-the-Counter Information Only or over-the-Counter and Progestin-Only Pill Information), N = 778
Chi-square tests performed, comparing distribution of responses by study arm.
Discussion
This study examined the impact of evidence-based information on clinician support for bringing an OC OTC. Among a diverse set of clinicians, support for bringing either a POP or a COC OTC increased among both study arms after viewing information. However, the group of clinicians randomized to receive only information about OTC OCs saw less of an increase in their support for an OTC POP than the group that received both OTC and POP information. Those receiving only OTC information saw an increase of approximately 9–12 percentage points for both pill types, and support for a COC was higher than support for a POP. Among those that received both OTC and POP information, there was a large increase of 29 percentage points in support for bringing a POP OTC, while support for bringing a COC OTC increased only slightly.
Clinicians' primary concern after viewing information for both pill types moving OTC was safety; however, this concern was more pronounced for COCs while other concerns, particularly around effectiveness and potential for incorrect use, were prevalent among those that opposed bringing a POP OTC. We did observe, however, differences in answers related to perceptions of POP efficacy between the two study arms. The results of this study suggest that assumptions about the effectiveness of POPs can be addressed by information highlighting the available evidence (or lack thereof in the case of the evidence underpinning assumptions of lower POP efficacy 23,24 ) and strong safety profile of POPs. Given the extremely limited set of contraindications to using a POP and evidence supporting moving this type of pill OTC, alternative strategies or additional follow-up may be required to address remaining concerns held by those whose opinions did not change after viewing information.
Support for bringing both a POP and COC OTC increased among clinicians who viewed only information on OTC access generally; however, the increase in support for a POP was ∼50% higher in those who saw POP information in addition to the OTC information. We saw less movement in support for moving a COC OTC among clinicians who viewed the POP specific information. Further research could explore the impact of information that includes broad information on OTC access and specific information about both POPs and COCs to understand how highlighting data specific to each type of OC impacts clinician attitudes about OTC access. It may be that without specific information, general information about OCs privileges COCs since this is the predominant formulation in the United States 10,25 and clinicians have to rely on their own knowledge and preconceptions in the absence of specific information about each type of OC.
This study also highlighted interesting differences in the baseline opinions among different types of clinicians about moving an OC OTC. Nurse-midwives were particularly more likely to support bringing an OC OTC than other types of clinicians surveyed before the presentation of information, potentially due to nurse-midwives role in serving underserved populations. 26 Clinicians that worked at academic hospitals or clinics, clinicians who worked at public hospitals, and those treating a higher proportion of Medicaid patients were more likely to support bringing a pill OTC at baseline. One reason for this difference may be that clinicians working in public hospitals or academic facilities may be exposed to a more diverse patient population that may be less likely to have insurance and for whom they could see the benefit of an OTC OC. Clinicians who prescribed LARCs to a large proportion of their contraceptive patients were also more likely to support bringing an OC OTC than clinicians who prescribe mostly OCs; such a difference may be driven by clinicians who mostly prescribe OCs and who are concerned about the potential impact OTC OCs would have on their practice. Female clinicians were also more likely to support an OTC POP than their male colleagues, a finding supported by Howard et al. 16 Future research could further explore differences in OTC support by clinician characteristics and how that might inform future messaging around moving an OC OTC.
There are a number of limitations to this study. First, we cannot assess the representativeness of the sample in this study. However, the sample does capture a more diverse sample than previous studies on clinician opinions of moving an OC OTC. 15,16 In addition, this study only assessed immediate changes in support of bringing OCs OTC. We cannot assess whether the information presented had any change on support over a longer period of time. Questions about effectiveness of POPs were assessed only after randomization, so we cannot confirm whether differences observed were the product of information presented or were due to preexisting differences between groups; however, given the balance on a number of clinician characteristics and the fact that overall support for OTC OCs was similar between groups, the latter may be less likely. Finally, we cannot assess which specific pieces of information were most effective at influencing clinician support given that the information was tested as a whole.
Conclusion
When provided with evidence-based information about bringing OCs OTC, the majority of clinicians supported bringing either a POP or COC OTC. Support for moving a POP OTC increased substantially among clinicians who received information about POPs. This study highlights the importance of educating clinicians on available evidence on OCs, and on POPs in particular, as well as educating them on the evidence supporting OTC access for all OCs.
Footnotes
Authors' Contributions
All authors certify that they have contributed substantially to the article. A.W.: project administration, data analysis, visualization, writing-original draft. C.Z.: data collection, formal analysis, writing—review and editing. N.L.: data analysis, writing—review and editing. D.G.: conceptualization, methodology, writing—review and editing. K.G.: conceptualization, methodology, funding acquisition, supervision, writing—review and editing.
Author Disclosure Statement
Ibis Reproductive Health has a formal partnership with HRA Pharma to work together on the research needed for an application to the U.S. FDA to make a birth control pill available OTC. Ibis does not receive financial support from HRA Pharma and has no financial interest in an OTC product. Ibis has taken a public stand on the need for insurance coverage of OTC contraceptives, including an OTC OC. The authors have no further conflicts of interest to disclose.
Funding Information
This study was supported by The David and Lucile Packard Foundation (grant No. 2015-63012). The funders had no involvement with the study design; collection, analysis, and interpretation of the data; writing of the article; or the decision to submit the article for publication.