
Abstract
Background:
This study examines the relationship among food insufficiency, adequacy of prenatal care, and barriers to prenatal care.
Materials and Methods:
Using data from the Pregnancy Risk Assessment Monitoring System (PRAMS), 2009–2016, negative binomial and logistic regression models were used to assess the association among food insufficiency during pregnancy, late onset of prenatal care, the number of prental care visits, as well as barriers to prenatal care.
Results:
Findings indicate that food insufficiency is associated with not initiating prenatal care during the first trimester and having fewer overall visits. In addition, food insufficiency is associated with more overall barriers to prenatal care, and this association operates through several specific barriers, including not having enough money, lacking transportation to get to the clinic or doctor's office, not being able to get time off work, not having a Medicaid card, having too many other things going on, and having no one to take care of children.
Conclusion:
Considering the adverse consequences of both food insufficiency and a lack of sufficient prenatal care for maternal and child health, study findings suggest a need to develop targeted interventions that expand access and remove barriers to prenatal care among food-insufficient women.
Introduction
As of 2018, an estimated 37 million individuals were living in food-insecure households in the United States (i.e., households that were unable to acquire nutritionally adequate food). 1 Because of the wide range of physical and psychological health problems that stem from food insecurity, it is widely considered to be a significant public health issue. 2
In the United States, rates of food insecurity are higher among certain segments of the population, including households headed by African American and Hispanic individuals, unmarried persons, younger individuals, those with less education, and households below the poverty line. 1 –3 Moreover, the risk of food insecurity can be heightened among pregnant women for several reasons including (1) increased household expendutures on pregnancy-related costs, (2) elevated nutrient demands and greater food expenditures, (3) more difficult and time-consuming efforts involved in food preparation, and (4) the potential need for women to curtail employment, especially during later pregnancy, thereby generating economic hardship. 4
While food insecurity raises substantial health risks for all those who experience it, the health consequences of food insecurity may be particularly elevated when experienced during pregnancy. Indeed, nutritional needs are elevated throughout pregnancy, and prior research has found experiencing food insecurity during pregnancy to be associated with negative birth outcomes, such as low birth weight, 5 preterm birth, 6 and certain birth defects, 7 as well as maternal health issues, including gestational diabetes, 8 gestational weight gain, 9 and depression. 10 Given the health risks associated with food insecurity during pregnancy, it is important to develop interventions that can alleviate food insecurity among pregnant women.
One potentially fruitful avenue is through screening for food insecurity during prenatal care and using prenatal care as an opportunity to provide resources to food-insecure women. One recent study found that participation in group prenatal care can improve food security by improving budget managing skills, diet, and self-efficacy in obtaining healthy foods. 11 However, while prenatal care may offer an opportunity to reduce food insecurity, prenatal care is not accessed in a consistent or timely manner by all pregnant women, and a lack of adequate prenatal care may increase the risk of unintended high-risk pregnancies and adverse birth outcomes. 12,13 Notably, over half of women who expereinced delayed or no prenatal care during their preganancy report having wanted to establish earlier prenatal care. 14 Certain women are at higher risk for experiencing late prenatal or inadequate number of prenatal care visits, including those who are younger, non-white, have lower education levels, women with higher numbers of previous births, and those who are on Medicaid. 15
Furthermore, some at-risk populations face a host of barriers to prenatal care, including lacking proper medical coverage, financial challenges, lacking transportion, not having available time, difficulties finding child care, or an inability to get time off work. 14,16 –21 To be sure, receiving insufficient prenatal care is associated with a host of adverse health outcomes for infants, including preterm birth, lower birth weight, and increased risk of infant mortality, 12,16,22,23 whereas the early and consistent utilization of prenatal care is associated with improved birth otucomes 24 and better maternal health. 25 Prior work has found these barriers to be more prevelant in light of ceratin risk factors, such as experiencing recent stressful life events, being younger, being a racial/ethnic minority, being unmarried, having lower education, having more prior births, and lower levels of household income. 26 –29 Despite existing disparities in prenatal care access, little is known about whether women experiencing food insecurity during pregnancy face challenges with early initiation and continuous utilization of prenatal care, as well as whether food insecurity is assoicated with unique barriers to prenatal care. Notwithstanding this void in the literature, one study from Bangledesh found that household food insecurity was associated with both under- and non-underutilization of maternal health care services (including before and after childbirth). 30 Thus, it remains plausible that food-insecure pregnant women may also face a greater number of barriers to prenatal care.
The purpose the current study is to extend knowledge regarding access and barriers to prenatal care faced by food-insufficient women during pregnancy. The findings from this study can aid in the identification of barriers to prenatal care and can point to intervention opportunities, which in turn can lead to expanded prenatal care access among this vulnerable population.
13
Specifically, we address three key questions: Is food insufficiency associated with late prenatal care onset and fewer prenatal care visits during pregnancy? Are food-insufficient women exposed to more barriers to prenatal care? Is food insufficiency associated with specific barriers to prenatal care?
Materials and Methods
Data
This study uses data from the Pregnancy Risk Assessment Monitoring System (PRAMS). PRAMS is an ongoing population surveillance system of live births in the United States conducted by the Centers for Disease Control and Prevention (CDC) and state health departments. The PRAMS survey uses birth certificates to obtain an annual stratified sample of ∼1,000 to 3,000 women who recently delivered a live birth in participating states. Questionnaires collect retrospective data from recent mothers and survey responses are linked with birth certificate data. Recent mothers are mailed a survey ∼3–6 months following birth. Up to five contact attempts are made by mail surveys, and states follow up with nonresponders by phone call within a week of the last mailed survey. 31 The use of PRAMS data for the current study were approved by the CDC. The list of states and years that include questions on food insufficiency, barriers to prenatal care, and relevant covariates are presented in Appendix A1.
Dependent variable
Dependent variables include the timing of prenatal care initation and number of prenatal care visits that a woman reported receiving during her most recent pregnancy. Start of prenatal is a binary measure of whether a respondent began prenatal care during the first trimester. Coding the measure in the direct of risk, we classify women who reported starting prenatal care during the first trimester with a value of 0 and those who did not with a value of 1. Prenatal care visits is a binary indicator that measures whether a recent mother reported having fewer than nine prenatal care visits during her recent pregnancy (0 = 9 or more visits; 1 = less than 9 visits). These thresholds are based on those used in established measures of the adequacy of prenatal care, such as the Kessner Index, 32 as well as measurement used in prior research using PRAMS data. 33
Next, barriers to prenatal care were reported following a question in the PRAMS survey asking “Did any of these things keep you from getting prenatal care at all or as early as you wanted?” Specifically, we focus on whether women reported any of eight experiences, which capture a variety of challenges to prenatal care listed in Appendix A2. Affirmative responses were assigned a value of 1 and responses of no were assigned a value of 0. Reponses were summed into a prenatal care barriers index, which ranges from 0 to 8 (Cronbach's Alpha = 0.732).
Independent variable
Food insufficiency is measured using a survey item that asks respondents “during the 12 months before your new baby was born, did you ever eat less than you felt you should because there was not enough money to buy food?” (1 = yes; 0 = no). The wording of the food insufficiency item in the PRAMS survey is based on a single-item question from the multi-item United States Department of Agriculture food security survey module, 1 and has been employed by recent research using PRAMS data. 34 –36
Control variables
Control variables are included to measure several demographic and socioeconomic characteristics that may confound the estimates. Demographic measures include maternal age (17 or younger [reference], 18–24, 25–29, 30–34, 35 or older), and maternal race/ethnicity (white [reference], Hispanic, black, other race/ethnicity). A binary item is included to measure whether the mother was a college graduate (1 = 16 or more years of education, 0 = less than 16 years). Marital status is measured using a single item that captures if a respondent reports she is currently married (1 = yes, 0 = no). We also measure characteristics of the current and past pregnancies, including number of prior births (0 [reference], 1, 2, 3+) and whether the current pregnancy was planned (1 = yes, 0 = no). We include measures of economic status, including whether a mother received Medicaid benefits in the month before the most recent pregnancy beginning (1 = yes, 0 = no) and the total household income levels before taxes in the 12 months before a respondent's new baby was born (<$10,000 [reference], $10,000–14,999, $15,000–19,999, $20,000–24,999, $25,000–34,999, $35,000–$49,999, $50,000 or greater). To account for the number of persons who rely on income in a household, we include a variable that adjusts for the number of dependents (including the responsdent) in a household. Finally, models include binary indicators for state of residence and year of birth to account for variation in barriers to prenatal care across place and time.
Analytic approach
We begin by regressing food insufficiency on the measures of not starting prenatal care in the first trimester and having less than nine prenatal care visits among the full sample (n = 31,606). Given the binary nature of both these measures, logistic regression is used. Next, we assess the association between food insufficiency and barriers to prenatal care. We first examine the total number of barriers in the full sample, and use negative binomial regression given the outcome variable is positively skewed with large number of zero values. We then examine whether food insufficiency is related to the eight specific barriers to prenatal care among the subset of women who either received no prenatal care or did not receive prenatal care as early as they wanted (n = 5,173). The specific barriers to prenatal care are examined using a series of eight separate logistic regression models that uses responses to each of the specific barriers to prenatal care as dependent variables, while controlling for covariates. All statistical analyses are conducted using Stata V.16.1. Models were adjusted for survey weights and strata information to account for the complex design of the PRAMS survey. Missing data were addressed using multiple imputation with chained equations, resulting in the utilization of 20 multiply imputed datasets. Results from analyses using listwise deletion produced substantively similar findings. Appendix A3 reports the percent of missing data by variable.
Results
Summary statistics stratified by food insufficiency are reported in Table 1. Approximately 9.7% of the sample reported food insufficiency in the 12 months before birth. Women who experienced food insufficiency were significantly more likely to report not having prenatal care in the first trimester (26.1% vs. 14.0%, p < 0.001) and have fewer than nine prenatal care visits throughout pregnancy (25.0% vs. 17.8%, p < 0.001). In addition, food-insufficient women were less likely to report having no barriers to prenatal care (75.1% vs. 90.0%, p < 0.001), but more likely to report having one (6.9% vs. 4.1%, p < 0.001), two (6.6% vs. 3.3%, p < 0.001), three (5.0% vs. 1.3%, p < 0.001), or four or more barriers (6.5% vs. 1.3%, p < 0.001). The prevalence of specific barriers to prenatal care stratified by food insufficiency is reported in Figure 1. Food-insufficient women reported a higher prevalence of several barriers to prenatal care, including not having enough money, lacking transportation, not being able to get time off work, not having a Medicaid card, being too busy, and not having childcare.
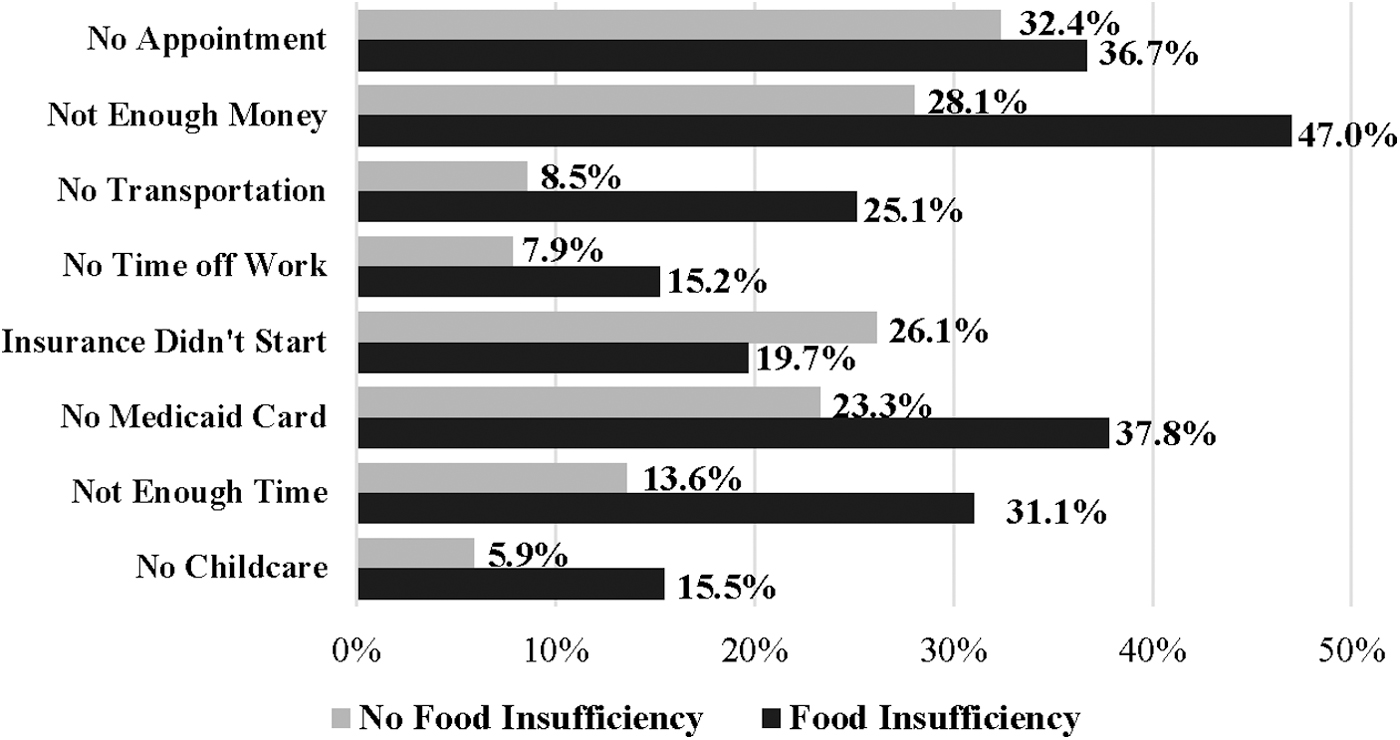
Prevalence of barriers to prenatal care stratified by food insufficiency (n = 5,173).
Weighted Summary Statistics Stratified by Food Insufficiency
Table 2 presents the results from the logistic regression of food insufficiency predicting late start and the number of prenatal care visits. The bivariate results in Model 1 show that food-insufficient women were ∼2.1 times more likely to not begin prenatal care during the first trimester (odds ratio [OR] = 2.141, 95% confidence interval [CI] = 1.846–2.482). Model 2 includes the set of control variables, with the results showing that after covariate adjustment, food insufficiency is associated with ∼1.3 times the odds of not beginning prenatal care during the first trimester (OR = 1.290, CI = 1.104–1.508). The bivariate results in Model 3 demonstrate that food insufficiency is associated with a 1.5 times increase in the odds of having fewer than nine prenatal care visits (OR = 1.566, CI = 1.340–1.830). After adjusting for covariates, results in Model 4 show that food insufficiency retains a positive and marginally significant association with reporting fewer than nine prenatal care visits (OR = 1.161, CI = 0.984–1.370).
Results of Logistic Regression of Food Insufficiency on Prenatal Care (n = 31,606)
p < 0.001, ** p < 0.01, * p < 0.05.
CI, confidence interval; OR, odds ratio.
Table 3 presents the results of the negative binomial regression of the number of prenatal care barriers regressed on food insufficiency. The bivariate results shown in Model 1 demonstrate that food insufficiency is associated with an approximately three-times greater rate of barriers to prenatal care (incidence rate ratio [IRR] = 3.188, 95% CI = 2.721–3.734). After including the control variables in Model 2, food-insufficient women are expected to endure barriers to prenatal care at an ∼1.9 times greater rate (IRR = 2.138, CI = 1.820–2.251). Results were consistent in ancillary analyses that used a single-item factor in leui of the additive scale.
Results of Negative Binomial Regression of Food Insufficiency on Number of Prenatal Care Barriers (n = 31,606)
p < 0.001, ** p < 0.01, * p < 0.05, † p < 0.10.
IRR, incidence rate ratio.
Finally, we examine whether food insufficiency is associated with the odds of experiencing specific barriers to prenatal care, net of covariates, among the subsample of women who reported not starting prenatal care as early as they wanted or not engaging in prenatal care. The ORs from the eight separate logistic regression models are presented visually in Figure 2. Food insufficiency is associated with significant increases in the odds of several specific barriers to prenatal care, including not having an appointment (1.38, 95% CI = 1.041–1.826), not having enough money (OR = 1.824, CI = 1.386–2.402), lacking of transportation to get to the clinic or doctor's office (OR = 2.697, CI = 1.877–3.874), not being able to get time off work (OR = 1.831, CI = 1.241–2.699), not having a Medicaid card (OR = 1.502, CI = 1.126–2.004), having too many other things going on (OR = 2.160, CI = 1.593–2.927), and having no one to take care of children (OR = 2.377, CI = 1.494–3.779). Ancillary analyses showed the relationship between food insufficiency and all the dependent variables did not significantly vary by the maternal race/ethnicity.
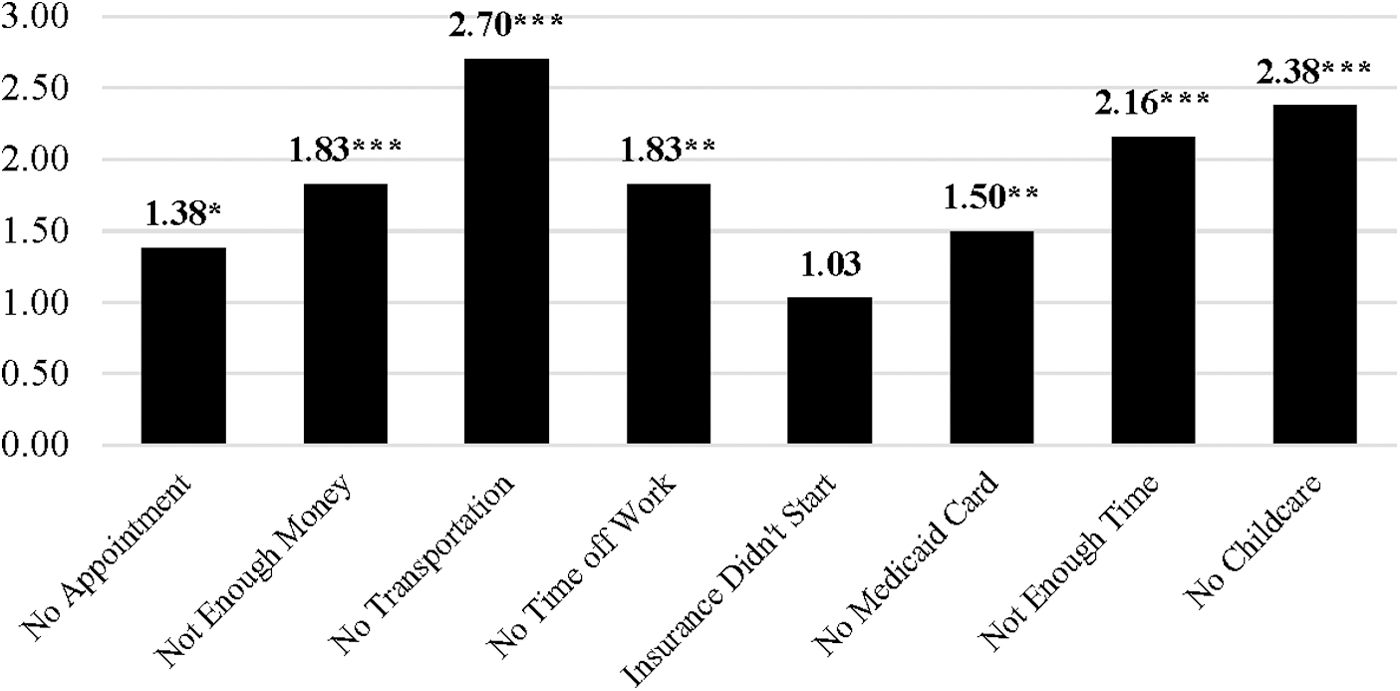
Results of logistic regression of food insufficiency on individual prenatal care barriers (n = 5,173). Models control for maternal age, maternal race/ethnicity, college graduate, currently marked, number of prior births, pregnancy planned, income levels, number of dependents, Medicaid recipient, state of residence, year of birth. ***p < 0.001, **p < 0.01, *p < 0.05.
Discussion
This study aimed to extend research on disparities in prenatal care by investigating whether food insufficiency is related to the utilization of prenatal care, as well as which specific barriers to prenatal care were experienced by food-insufficient women. This study revealed three key findings. First, women who experienced food insufficiency during pregnancy were less likely to begin prenatal care during the first trimester and having few prenatal care visits. Second, food insufficiency was associated with experiencing a greater number of barriers to prenatal care. Finally, food insufficiency was also associated with independent increases in the odds of experiencing certain barriers to prenatal care, including not having an appointment, not having enough money, lacking of transportation to get to the clinic or doctor's office, not being able to get time off work, not having a Medicaid card, having too many other things going on, and having no one to take care of children.
Several of these barriers can be understood within the context of low socioeconomic status, including not having enough money and not having a Medicaid card. Indeed, economic issues are a key barrier to accessing health care services, 17,37 as well as a primary driver of food insufficiency. 1 –3 Importantly, these findings also suggest that not having timely access to public health insurance programs such as Medicaid also serves as a barrier to prenatal care among food-insufficient women. This is important considering previous research has found that Medicaid participation reduces both food insufficiency and underutilizing medical resources. 38,39 Thus, the expansion of programs, such as Medicaid, to cover a greater number of women who experience food insufficiency during pregnancy may be a beneficial policy to enhance prenatal care participation among this population. 38 Similarly, alleviating economic challenges, possibly by enhancing benefits through programs, such as the Supplemental Nutrition Assistance Program (SNAP), may be a useful approach for reducing food insufficiency and associated economic hardship among pregnant women. 40,41 In addition, other policy changes such as expanding medical care access through the Affordable Care Act or granting universal access to care for pregnant women would likely offer benefits in increasing prenatal care access among food-insufficient women. 42 Likewise, the implementation of programs such as a basic income guauratee can be helpful in alleviating both food insufficiency and socioeconomic barriers to prenatal care. 43,44
Relatedly, not being able to get time off work was also a barrier associated with food insufficiency. While we cannot extricate the exact mechanisms behind this, it is possible this is also an issue related to socioeconomic status, given that many low-income workers do not have paid leave or are employed in positions with less flexible schedules. 45 While we do not have information on the type of employment women had during their pregnancy, it is likely that many food-insufficient women were employed in lower-wage positions and, as a result, these women may have faced challenges taking time off work as doing so could both risk women's employment as well as reduce earnings.
Findings revealed that lacking transportation to get to the clinic or doctor's office was an important barrier associated with food insufficiency. Prior research has found that a lack of transportation is a risk factor for food insufficiency, 46,47 and among food-insufficient populations, lacking reliable transportation is a key barrier in receiving health care services. 48 Indeed, Arena and Salerno highlight how a lack of reliable transportation poses a challenge for food-insufficient individuals that creates barriers in both accessing food, as well as other essential services, such as health care: “residents without a car or with limited funds for gas, insurance, and repairs often have trouble accessing important services and programs, including grocery stores, schools, food pantries, health clinics, and job training.” 49 A potentially beneficial intervention, therefore, may be providing vouchers for public transportation, taxis or ride-sharing services to improve access to prenatal care among food-insufficient women who lack reliable transportation. 50
Another important barrier was not having anyone to care for children. Because of economic challenges, food-insufficient women likely face fewer options in where to obtain childcare, and may have to rely more heavily on support from family or friends. Relatedly, food insufficiency was also associated with women reporting being too busy for prenatal care. Although there is limited research on how food insufficiency impacts time allocation, existing research does suggest that food-insufficient households spend more time on food preparation. 51 In addition, food insufficiency may be associated with greater time traveling to food pantries or finding affordable foods, 52,53 which is further amplified given that pregnancy is a period of decreased mobility.
Given that challenges with time and transportation to access prenatal care, these findings point to the need to expand access to prenatal care in a more flexible manner. One possibility is through the expansion of virtual prenatal care that leverages telemedicine to make care more flexible and patient centered. 54 The flexibility of such an approach would be particularly useful as fixed time slots for prenatal care visits are often challenging considering varying work schedules, difficulties securing reliable transportation, and arranging childcare, 55 all of which are challenges faced by food-insuffiicent women in the current study. Another beneficial approach may be through expanding group prenatal care options to food-insuffiicent women. Prior work has found that involvement in group prenatal care can improve food insufficiency, 11 and such an approach can offer collateral benefits of building social support networks, which can be protective against food insufficiency. 56 –60
Limitations
There are limitations with the current study that can be expanded upon in future research. First, the measure of food insufficiency is a binary item based on a single question. It would be useful for future research to assess the questions posed in this study using a multi-item scale to examine variation across levels of food insufficiency. 1 Second, the PRAMS survey asked about barriers to prenatal care among those who reported issues accessing prenatal care during their pregnancy. Thus, we could not examine barriers to prenatal care among women who experienced timely prenatal care, but may have still experienced barriers with receiving care. Moreover, we could not assess whether food-insufficent women experienced worse prenatal care because they faced more barriers. Third, while we examined a range of eight separate barriers to prenatal care, we were limited by the questions provided in the PRAMS survey. It is possible that food insufficiency leads to other unique barriers that were not captured in these data. It would be useful for future qualitative research to investigate barriers to prenatal care among food-insufficient women to learn about the specific challenges faced and whether there are additional barriers that were not captured in the current study. Fourth, the current data did not include measures on health-seeking behaviors, which may be relevant for understanding prenatal care utilization. Finally, the measure in the PRAMS study asked about barriers to not receiving prenatal care, and those who did not receive prenatal care as early as they wanted. It is possible that these two outcomes (i.e., no prenatal care and late initation) are differentially impacted by food insufficiency and various barriers to prenatal care. Consistent with other national statistics, however, there were few cases of women who reported no prenatal care visits in the PRAMS data. 15 Accordingly, we could not separately assess this group. However, future research that differentiates how food insufficiency and various barriers to prenatal care impact late onset versus not receiving any prenatal care would be valuable.
Conclusion
The findings from this study highlight that food-insufficient women face several barriers in obtaining prenatal care. This is a particularly important issue as prenatal care may be a key intervention to connect food-insufficient women to valuable resources that can improve access to nutritious foods, which may in turn improve maternal and infant health. Nonetheless, by identifying the barriers that inhibit food-insufficient women from obtaining prenatal care, the findings of the current study are useful for informing policy efforts aimed at overcoming these barriers and expanding prenatal care access for food-insufficient women.
Footnotes
Acknowledgments
The authors wish to acknowledge the CDC PRAMS Working Group: Tammie Yelldell, MPH (AL), Kathy Perham-Hester, MS, MPH (AK), Letitia de Graft-Johnson, DrPH, MHSA (AR), Ashley Juhl, MSPH (CO), Jennifer Morin, MPH (CT), George Yocher, MS (DE), Tara Hylton, MPH (FL), Florence A. Kanu, PhD, MPH (GA), Matt Shim, PhD, MPH (HI), Julie Doetsch, MA (IL), Jennifer Pham (IA), Tracey D. Jewell, MPH (KY), Rosaria Trichilo, MPH (LA), Tom Patenaude, MPH (ME), Laurie Kettinger, MS (MD), Hafsatou Diop, MD, MPH (MA), Peterson Haak (MI), Mira Grice Sheff, PhD, MS (MN), Brenda Hughes, MPPA (MS), Venkata Garikapaty, PhD (MO), Emily Healy, MS (MT), Jessica Seberger (NE), David J. Laflamme, PhD, MPH (NH), Sharon Smith Cooley, MPH (NJ), Sarah Schrock, MPH (NM), Anne Radigan (NY), Pricila Mullachery, MPH (New York City), Kathleen Jones-Vessey, MS (NC), Grace Njau, MPH (ND), Ayesha Lampkins, MPH, CHES (OK), Cate Wilcox, MPH (OR), Sara Thuma, MPH (PA), Karine Tolentino Monteiro, MPH (RI), Kristin Simpson, MSW, MPA (SC), Ransom Wyse, MPH, CPH (TN), Tanya Guthrie, PhD (TX), Nicole Stone, MPH (UT), Peggy Brozicevic (VT), Kenesha Smith, MSPH (VA), Linda Lohdefinck (WA), Melissa Baker, MA (WV), Fiona Weeks, MSPH (WI), Lorie Chesnut, PhD (WY), CDC PRAMS Team, Women's Health and Fertility Branch, and Division of Reproductive Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Appendix
Percent of Missing by Variable
| Variable | Percent missing |
|---|---|
| Food insufficient | 1.3% |
| No prenatal care first trimester | 0% |
| <9 prenatal care visits | 2.5% |
| Number of barriers | 2.3% |
| Maternal age | 0% |
| Maternal race/ethnicity | 0.3% |
| College graduate | 1.0% |
| Prior births | 0.2% |
| Pregnancy planned | 1.3% |
| Household income | 5.7% |
| Number of dependents | 0% |
| Medicaid | 0.2% |