
Abstract
Background:
Quality of life in adenomyosis (AD) patients has been poorly investigated. Previous data suggest that AD has negative impact on the quality of life in these women.
Materials and Methods:
From September 2018 to December 2019, all consecutive female premenopausal patients aged ≥18 years diagnosed with AD by transvaginal ultrasound (TVU) were invited to participate in a comparative cross-sectional study. The Short Form-36-item (SF-36) health questionnaire and the Hospital Anxiety and Depression Scale (HADS) were administered. Work productivity and activity impairment were assessed using the Work Productivity and Activity Impairment Questionnaire: General Health version (WPAI:GH). Data obtained from these patients were compared with women with normal-appearing myometrium in the TVU recruited during routine gynecological visits. The study was approved by the Clinical Research Ethics Committee of the Hospital Clinic (reference HCB/2018/0919).
Results:
One hundred three patients with AD and 214 without AD were analyzed. Patients with AD compared to those without AD showed significantly lower scores in all domains of the SF-36 questionnaire and mean (SD) higher scores in the HADS questionnaire for anxiety (10.06 [3.04] vs. 6.92 [2.98], p < 0.001) and depression (6.39 [3.89] vs. 2.74 [2.01], p < 0.002). Significant differences (p < 0.001) were also found for the percentages of absenteeism (12.2% vs. 1.1%), presenteeism (31.1% vs. 11.4%), overall work productivity loss (38.2% vs. 12.4%), and activity impairment (55.7% vs. 9.9%). The presence of AD was associated with higher yearly estimated indirect costs of €5161.32 (€7928.0 vs. €2460.8, p < 0.001).
Conclusions:
AD negatively affects women's health-related quality of life, psychological health, and work productivity, with impairment at work and daily activities, and higher risk for anxiety and depression.
Introduction
Adenomyosis (AD) is a chronic benign gynecological disease characterized by the presence of endometrial glands and stroma in the thickness of the myometrium, together with hyperplasia and hypertrophy of smooth muscle fibers. 1 The etiology is unknown; however, the predisposing factors include multiparity and a history of previous uterine surgeries. AD affects between 20% and 35% of women of reproductive age 2 and its symptoms include abnormal uterine bleeding, pelvic pain (dysmenorrhea, chronic pelvic pain, dyspareunia, dyschezia, and dysuria) and infertility. 3 These symptoms are not specific to AD or may be ignored by some patients and clinicians, which may explain why AD is often underdiagnosed or diagnosed only after a significant delay.
In the past years, cases of AD were usually diagnosed after histopathological examination of hysterectomy specimens. At present, however, other diagnostic methods such as transvaginal ultrasound (TVU) and magnetic resonance imaging have shown to be precise and noninvasive for the detection of AD. 4
AD symptoms and the lag in the diagnosis could affect the physical, mental, and social well-being of women, resulting in a decrease in health-related quality of life (HRQoL), impairment in work productivity, and increased states of anxiety and depression. However, these issues have been poorly investigated, and the few studies published have suggested a negative impact of the disease on HRQoL. 5 –7 Moreover, to our knowledge, no previous study has assessed the impact of the disease on mental health and impairment in work productivity. This information may be useful for developing an integrated approach to AD patients, improving work productivity, and reducing the indirect costs generated by this disease.
Therefore, the aim of this study was to assess the impact of AD on different aspects of women's psychological health, HRQoL, and work productivity, as well as to estimate its effects in terms of a potential increase in indirect costs.
Materials and Methods
Study design
From September 2018 to December 2019, a single-center comparative cross-sectional study was conducted at the Department of Gynecology of a tertiary teaching hospital of the Universidad de Barcelona, in Barcelona, Spain. The primary objective of the study was to assess the impact of AD on different aspects of the women's health, including HRQoL, anxiety, and depression, as well as on work productivity. The secondary objective was to determine how impairment of work productivity could potentially affect AD-related indirect costs.
The study was approved by the Clinical Research Ethics Committee of the Hospital Clinic (reference HCB/2018/0919, date of approval September 19, 2018). Written informed consent was obtained from all participants.
Patients
All consecutive premenopausal aged 18 years or older diagnosed with AD by TVU referred to the Department of Gynecology for treatment during the 15-month study period were included, provided that they gave written consent and completed the study questionnaires. For each case, we identified approximately two randomly selected premenopausal women aged ≥18 years without AD as confirmed by a normal-appearing myometrium in TVU. Healthy patients were recruited during routine gynecological visits for contraception or cervical cancer screening, and gave written consent to complete the study questionnaires. The exclusion criteria for women with and without AD were as follows: presence of rheumatologic or autoimmune diseases, pelvic or lumbosacral pain caused by conditions other than AD, known psychiatric disorders, history of substance abuse, use of gonadotrophin-releasing hormone analogs in the past 6 months, use of hormonal treatment in the past 3 months, infertility, endometriosis and other uterine conditions (fibroids, polyps, and endometrial hyperplasia), neoplasms, and history of hysterectomy and/or bilateral adnexectomy.
Study procedures
All patients underwent two–three dimensional TVU using an endovaginal probe (type RIC5-9, Voluson V730 Expert; GE Healthcare, Milwaukee, WI). The procedures were performed by two expert sonographers (C.R. and M.R.), following the Morphological Uterus Sonographic Assessment consensus statement. 8 AD was diagnosed when at least two sonographic criteria were clearly met. 9
The study questionnaires included Spanish validated versions of the Short Form 36-item (SF-36) questionnaire, 10 the Hospital Anxiety and Depression Scale (HADS) 11 and the Work Productivity and Activity Impairment Questionnaire: General Health version (WPAI:GH). 12 The SF-36 is a self-administered 36-item instrument that measures patients' perceptions of their general health status during the past month, and measures eight domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health, and has two summary scores (physical component summary [PCS] and mental component summary [MCS]). Higher scores indicate better HRQoL.
The HADS is composed of two subscales, anxiety, and depression, with a four point (0–3) response category. Possible scores range from 0 to 21 for anxiety and 0–21 for depression, with higher scores denoting poorer psychological conditions. Scores between 0 and 7 represent “no case”; 8 to 10 indicate “possible case”; and 11 to 21 suggest a “probable case of anxiety/depression”. The WPAI:GH consists of six items measuring four domains: (1) absenteeism (percentage of work time missed due to health problems in the past week, calculated as: [hours missed due to health problems/(hours missed due to health problems + hours worked)] × 100); (2) presenteeism (percentage of impairment experienced at work due to health problems in the past week, calculated as: [degree health affected productivity while working/10] × 100); (3) overall work productivity loss (absenteeism plus presenteeism, calculated as: [absenteeism + (hours worked × presenteeism)] × 100); and (4) daily activity impairment (percentage of impairment in daily activities due to health problems in the past week, calculated as: [degree health affected daily activities/10] × 100). Only respondents with full- or part-time employment provided data for absenteeism, presenteeism, and overall loss of work productivity and all the respondents provided data for daily activity impairment. The domain scores are expressed as percentages, with higher percentages indicating greater loss of work productivity and impairment in activity. Similar to other studies, 13 because of the cyclic fluctuations of AD-associated symptoms, a 4-week rather than the original 7-day assessment period was used, even though it has not been validated for evaluating these effects in the past month.
To estimate total annual indirect costs, we used data from the Ministry of Labor, Migration and Social Security (Ministerio de Trabajo, Migraciones y Seguridad Social, MTMSS), and the WPAI:GH, taking into account the number of hours paid for each patient. The median 2017 weekly wages by age and sex obtained from the statistics section of the MTMSS were applied as unit costs to work productivity variables (absenteeism and presenteeism). The number of hours missed due to absenteeism and presenteeism were calculated for each respondent and multiplied by their associated estimated hourly wage, based on age and gender. These figures were annualized by multiplying by 50 work weeks in a year, and combined to estimate the total indirect costs. Costs were estimated in euros.
Days of work missed annually were calculated using reported work hours missed based on the WPAI:GH, assuming a 40-hour work week and 50 weeks worked annually.
Data collection
Sociodemographic data, anthropometric variables, gynecological information, and results of the study questionnaires were collected in all the patients. Moreover, we assessed the intensity of different types of pain using the Numerical Rating Scale (NRS). The NRS is a numerical scale, in which a respondent selects a whole number (0–10) that best reflects the intensity of the pain. 14,15 The common format is a horizontal bar or line with 0 indicating “no pain” and 10 the “worst pain imaginable.” This scale can be used for each type of pain, namely dysmenorrhea, dyspareunia, dyschezia, and nonmenstrual pelvic pain and dysuria. The degree of pain was divided into three categories as mild (1–3), moderate (4–6), and severe (≥7). 16
We assessed whether the patient had some type of pain with a NRS ≥4 and/or heavy menstrual bleeding (HMB). HMB was defined as a score ≥100 in “the Pictorial Blood Assessment Chart”, 17 which is equivalent to a blood loss of 80 mL.
Statistical analysis
The power analysis was calculated based on a previous study that assessed the psychological impact of endometriosis with pelvic pain versus asymptomatic endometriosis 18 ; the minimum number of patients needed with and without AD was estimated as 40 and 77, respectively (for a 1:2 ratio). Categorical variables are expressed as frequencies and percentages, and continuous variables as mean and standard deviation. The distribution of categorical variables in the AD and non-AD groups was compared with the chi-square test, and quantitative variables with the Student's t test for paired samples or the analysis of variance as appropriate. Statistical significance was set at p < 0.05. Statistical analysis was performed with the Statistical Package for the Social Sciences software, release 25.0 for Windows (SPSS, Chicago, IL).
Results
There were 89 patients diagnosed with AD and 203 healthy patients, with a mean age of 38 years. In the group of patients with AD, three had undergone hysteroscopy with exeresis of an endometrial polyp, while in the non-AD group, one patient had undergone hysteroscopy with exeresis of an endometrial polyp and one patient had undergone laparoscopic myomectomy for a subserous myoma. Demographic and clinical characteristics are shown in Table 1. Sixty-five (56%) women in the AD group had at least one type of pain ≥4 in the NRS and/or HMB, the latter being the most common complaint (59%) followed by dysmenorrhea, pelvic pain, and dyspareunia, whereas the remaining 33 women had no pain or mild pain and they did not have HMB.
Demographic and Clinical Data of Women With and Without Adenomyosis
Data as absolute numbers and percentages in parenthesis unless otherwise stated.
NRS, Numerical Rating Scale.
As shown in Table 2, there were statistically significant differences in HRQoL between women with and without AD, with lower scores for all dimensions of the SF-36 questionnaire and the PCS and MCS. Positive screening for anxiety and depression were found in 38.9% and 8.3% of women in the AD group compared to 13.2% and 0% in the non-AD group, respectively (p < 0.001). Significantly, higher mean scores in the subscales of anxiety and depression were also observed among women with AD (Table 2). Women with some type of pain ≥4 in the NRS and/or HMB showed a significantly worse quality of life and higher scores for anxiety and depression than those with no/mild pain without HMB (Fig. 1). The results of the HRQoL and HADS subscales of anxiety and depression were also significantly different in patients with AD compared to healthy women (Fig. 1A, B, respectively).
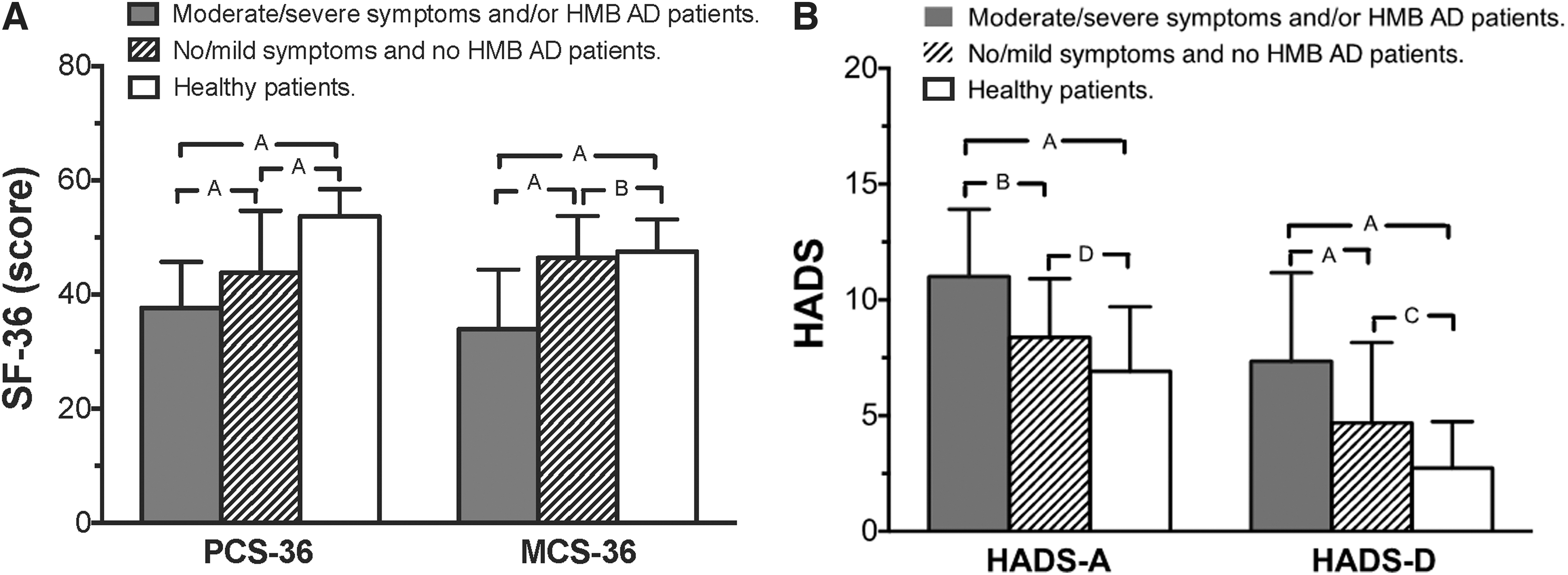
SF-36
Health-Related Quality of Life (Short Form 36) and Mental Health (Hospital Anxiety and Depression Scale) in Women With and Without Adenomyosis
Data as mean and standard deviation in parenthesis.
AD, adenomyosis; HADS, Hospital Anxiety and Depression Scale; MCS, mental component summary; PCS, physical component summary; SF-36, Short Form 36-item.
Most women (86.4%, n = 267) had a regular job when the study was conducted, with a significantly higher percentage of current workers among healthy women (91%) compared to AD patients (77.8%) (p = 0.007). The WPAI:GH questionnaire scores showed a significantly higher impact on work-related domains in women with AD compared with those without AD in absenteeism, presenteeism, overall productivity loss, and daily activity impairment. In addition, women with AD missed significantly more working days annually compared to women without AD, with a mean difference of 19.53 days lost per year (22.38 vs. 2.85; p < 0.001). Among women with AD, those with moderate/severe symptoms and/or HMB had a significantly higher degree of impairment in work productivity compared to women with no/mild symptoms and healthy women, whereas no differences were observed between AD women with no/mild symptoms and healthy women, except for daily activity impairment (Fig. 2A).

Work productivity and activity impairment variables
Moreover, women with AD had significantly increased costs resulting from both presenteeism (€5405.91 vs. €2232.01; p < 0.001) and absenteeism (€2583.76 vs. €228.78; p < 0.001) (Table 3). Based on overall loss of work productivity, estimated indirect costs were €5161.32 higher per employed respondent per year for those with AD compared with women without AD (€7928.00 vs. €2460.77; p < 0.001) (Table 3). On the contrary, the estimated indirect costs were 38.5% of the median annual salary for each patient in women with AD. As shown in Figure 2B, indirect costs were significantly higher in AD patients with moderate/severe symptoms compared to AD patients with no/mild symptoms and non-AD patients.
Work Productivity, Activity Impairment, and Indirect Costs in Women With and Without Adenomyosis
WPAI:GH, Work Productivity and Activity Impairment Questionnaire: General Health version.
Discussion
The presence of AD, particularly in symptomatic women, had a remarkable impact on HRQoL and mental health compared to the absence of the disease. Women with AD reported higher percentages of absenteeism, presenteeism, and overall loss of work productivity, as a result of which AD-related indirect costs were about €5000 higher annually than in women without AD.
A few studies have shown that symptoms and HRQoL in patients with AD improved after AD therapy. 7,19 Other studies have compared symptoms and HRQoL in patients with AD with a group of healthy patients demonstrating more pain, menstrual bleeding, and lower HRQoL in patients with AD. 20,21
In the present study, women with AD had lower scores in all the domains and in the PCS and MCS of the SF-36 questionnaire, as well as higher scores in the anxiety and depression subscales of the HADS compared to women without AD. These differences were found both in AD patients with moderate/severe symptoms and mild/any symptoms compared to non-AD patients. These findings indicate that the presence of AD per se is associated with a poorer quality of life and psychological health, and when it is associated with symptoms, the quality of life is further diminished. This may be because having AD, although with no or mild symptoms imply living with a chronic disease. These results in quality of life are similar to findings in other chronic diseases such as Sjögren's syndrome and diabetes mellitus. 22,23
Interestingly, AD had a clinically relevant impact on work productivity, with higher rates of absenteeism, presenteeism, overall loss of work productivity, and impairment of daily activities, mostly driven by AD patients with moderate/severe symptoms and/or HMB. No/mild symptoms in AD patients were associated with a numerical, but nonsignificant difference in work productivity when compared with non-AD patients.
The standard version of WPAI:GH considers the symptoms perceived by the patient during the last week, but as in other studies evaluating gynecological pathologies, 13 we used a 4-week assessment period. This may explain why WPAI:GH outcomes in our study were better compared to those in patients with endometriosis reported by Fourquet et al. 24 These authors assessed WPAI:GH outcomes according to how patients felt during the week of their last menstrual period (when exacerbation of symptoms most commonly occurs) or during the week of the month when symptoms were worse. In our study, we asked patients to respond to questions in relationship to how they felt in the preceding month, which may have included periods of absent or diminished symptoms.
Women in the AD group incurred an estimated €5161.32 more in indirect costs per year compared to women without AD, approximately two-thirds were ascribed to presenteeism and one-third to absenteeism, attributable to symptoms of AD. Similar findings have been reported in studies evaluating both chronic gynecological and nongynecological diseases. 25,26 The lower percentage of women working in the AD group is noteworthy compared with the non-AD patients, and may be related to the disease and accompanying symptoms.
The present study has several strengths: consistent inclusion criteria for AD were applied with TVU diagnosis established in >80 women by two expert sonographers, and the burden of AD on psychological health (HRQoL and mental health) and work productivity was evaluated in women with AD as compared to women without AD. Estimation of indirect costs associated with AD is a novel aspect of the study. However, this study has several limitations, the first being the relative small sample size, which was calculated according to a previous study on the impact of symptomatic endometriosis versus asymptomatic endometriosis. 18 Second, there are possible confounding factors such as urinary symptoms that might have had an impact on rates of anxiety/depression and work productivity, which were not assessed in our study, and also the fact of having HMB could cause fatigue and anemia in AD patients, which could also represent a depression-like symptom. Third, presenteeism was subjectively ranked by each patient and this could have generated a relative estimation of the indirect costs. Finally, we used a 4-week rather than the validated 1-week period in the WPAI:GH, and we have calculated “days of work missed annually” assuming a 40-hour work week and 50 weeks worked annually.”
Conclusion
This study shows that both the physical and mental quality of life of women with AD is reduced and may even be further decreased when these patients have moderate or severe symptoms. Furthermore, AD patients may be at high risk of anxiety and depression. It is also important to consider work impairment, which may translate into high indirect costs compared to women without AD, especially when moderate or severe symptoms are present. Clinicians should be aware of the need for the provision of care for the psychosocial aspects of AD.
Footnotes
Contribution to Authorship
A.M.A., M.A.M.-Z., and F.C. conceived and designed the study, analyzed and interpreted the data, wrote the first draft of the article, supervised the study, and corrected the final version. M.G., C.R., M.R., and I.N. were involved in the data collection as well as in the performance of transvaginal ultrasound.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.