
Abstract
Background:
Abnormal uterine bleeding (AUB) affects ∼1.4 million women in the United States each year. This study sought to identify differences in treatment decisions for managing noncancer-related AUB.
Materials and Methods:
IRB approval was obtained. This retrospective study analyzed data for all women 21–60 years old, diagnosed with AUB from July 1, 2013 through June 30, 2017, in an Obstetrics and Gynecology residents' clinic serving mostly underinsured patients. Patients with a diagnosis of postmenopausal bleeding or any gynecologic cancer were excluded. Two multivariable logistic regression models were used to identify variables independently associated with receiving surgical (vs. medical) treatment and any (vs. no) treatment.
Results:
Of 2,154 patients with AUB, 1,705 women met all inclusion criteria and had complete data for analysis. In the model examining receipt of surgical (vs. medical) treatment, women ages 41–60 were 4.8 times more likely than women 21–40 years old to receive surgical treatment. Women designated as “Other” (non-White) race/ethnicity were 80.8% less likely than Black/African American patients to receive surgery. Body mass index (BMI) and insurance type were not independently associated with receiving surgical treatment. In the model examining any (vs. no) treatment, women ages 41–60 (vs. 21–40) and of unknown (vs. Black/African American) race/ethnicity were 69.6% and 50.8% less likely to receive any treatment, respectively. BMI and insurance status were not independently associated with receiving any treatment.
Conclusion:
Management of AUB differed significantly by age and race/ethnicity, but not BMI or insurance. Further investigation among larger diverse populations is warranted to test the generalizability of these findings.
Introduction
In the United States, abnormal uterine bleeding (AUB) affects ∼1.4 million women each year. 1 AUB can be secondary to a wide array of anatomic and physiologic problems such as ovulatory dysfunction, uterine fibroids, endometrial polyps, and bleeding disorders. Women with AUB report health-related quality-of-life scores below the 25th percentile on key domains such as physical functioning, vitality, pain, and mental health. 2 In addition to these negative health outcomes, AUB has an estimated direct economic burden of ∼$1 billion per year. 2
While there are international guidelines for the diagnosis of AUB, 3 the choice of medical or surgical treatment is largely guided by the individual provider's approach depending on presumptive etiology, patient preference, provider judgment, and provider bias. Multiple medical therapeutic options are available, effective, and are often recommended as first-line treatments over a surgical approach. 3 –5 In a study of trade-offs of four treatment options using a hypothetical cohort of premenopausal women with heavy menstrual bleeding and no evidence of malignancy, the levonorgestrel-releasing intrauterine device (LNG-IUD) option demonstrated superior outcomes with regard to quality-adjusted life years and cost than hysterectomy and uterine ablation. 6 In a review of management options for AUB, surgical approaches, including hysterectomy, should be reserved for women with an anatomic cause for bleeding or whose bleeding does not improve with medical management. 7 However, a recent study found that, among women who underwent hysterectomy for uterine fibroids, endometriosis, or pelvic pain, no alternative treatment was documented in ∼40% of cases. 8 Women who were <40 years old and White were more likely to have documentation of nonsurgical treatment compared with women who were ≥40 and classified as Black/African American and from other racial/ethnic groups. 8 In addition, Lee et al. found women to be more likely to receive a laparoscopic hysterectomy than other modes of hysterectomy if they were <35 years, White, in the highest median income group, or had private insurance. 9,10
Analyses of differences in care for AUB have focused on specific diagnoses such as uterine fibroids and endometriosis; these studies primarily examined differences in surgical approaches. 11 –16 However, decisions regarding treatment are often made on a presumptive clinical diagnosis without conclusive preoperative evidence of the underlying etiology or postoperative supporting pathology. 8 Studies have identified clear racial and ethnic differences in the incidence, management, and outcomes of some but not all specific etiologies of AUB such as uterine fibroids. 11 –14 Currently, there is no research addressing differences in care for the broad diagnosis of AUB. The current literature lacks an analysis of differences in clinical decision-making and treatment options in the face of uncertain etiologies of benign AUB before the establishment of pathologic diagnosis. 8
The objective of this study was to describe differences in treatment decisions for the management of noncancer-related AUB among women seen in an Obstetrics & Gynecology (OBGYN) residents' clinic serving mostly Medicaid or uninsured patients. We hypothesized that differences in treatment decisions would be observed by age, race/ethnicity, body mass index (BMI), and insurance type.
Materials and Methods
After receiving approval of our Institutional Review Board, a retrospective descriptive study of existing data was performed at the institution's OBGYN resident clinic. This clinic is an urban, Midwest academic referral center and a safety-net hospital serving largely low-income African American women. Resident-clinic patients are managed through joint decision-making discussion between the onsite academic faculty and the individual resident. All patients who were seen in the resident clinic from July 1, 2013 through June 30, 2017 were potentially eligible for inclusion in the study. Women of reproductive age with a diagnosis of AUB were identified for inclusion using International Classification of Diseases (ICD)-9 and ICD-10 codes (Supplementary Table S1). Patients <21 years and >60 years at their first appointment during the study period were excluded as were any patients with a diagnosis of gynecologic cancer based on ICD-9 and ICD-10 codes (Supplementary Table S2).
For patients with AUB meeting our inclusion criteria, demographic information regarding age at first visit in the study period, race/ethnicity, BMI, and insurance status was collected from the resident-clinic database. Treatment information was collected from our billing data and medical records, and then categorized into medical treatment, surgical treatment, or no treatment. To classify receipt of medical treatment, a list of medications available in our clinic during the study period that could be utilized in the treatment of AUB was created and used to audit medical records. Medical treatment included tranexamic acid and reproductive hormone therapy in various routes of administration, including pill, patch, or ring forms of estrogens and/or progestins. We also included depot-medroxyprogesterone acetate, depot leuprolide, subdermal levonorgestrel implant, and LNG-IUD. We also included current procedural terminology (CPT) codes for insertion and/or removal of any IUD as medical management, as CPT coding does not distinguish hormonal from nonhormonal IUDs. Because all women in our study group had AUB, we presumed that IUD insertion or removal during the study period that was not additionally coded for contraception was involved in the AUB treatment plan, either to insert a hormonal IUD to treat AUB or to remove either a copper or hormonal IUD due to bleeding. Those AUB patients who received one or more of the aforementioned drugs or had insertion and/or removal of an IUD during the study period were identified and categorized as having medical treatment.
Information regarding surgical treatment for AUB was obtained using CPT codes corresponding to any type of hysterectomy, endometrial ablation, myomectomy, and uterine artery embolization (Supplementary Table S3). Patients who underwent any of these surgical procedures were classified as having surgical treatment for AUB, whether medical treatment was also given to these patients. Hysteroscopy, which in our population was always accompanied by a dilation and curettage, was considered diagnostic and not surgical treatment. Although polypectomies are performed as a surgical treatment for AUB, the CPT code for hysteroscopy with polypectomy is the same as that for hysteroscopy with sampling and thus indistinguishable from a diagnostic procedure (CPT code 58558). Finally, those AUB patients with neither medical nor surgical treatments recorded were categorized as having no treatment for AUB. This group included women who were intentionally observed and had spontaneous resolution, who might have declined recommended treatment, whose evaluation was not completed during the study period, or who were lost to follow-up.
Demographic characteristics of our sample include age, race/ethnicity, and insurance status. Age was categorized as 21–40 and 41–60 years. For analysis, race/ethnicity was categorized as Black/African American, White, Other, or Unknown. The Other category included patients designated as “Other,” Asian, Native Hawaiian/Pacific Islander, Native American/Alaska Native, “Multi-racial,” and Hispanic ethnicity. The Unknown race/ethnicity category included patients who were missing data or designated as “Unknown” or “Declined.” Insurance status was categorized as public (e.g., Medicaid or Medicare), private, and self-pay.
BMI in kg/m2 was calculated for each woman with weight and height data, and classified using the Centers for Disease Control and Prevention (CDC) overweight and obesity categories. 17 For analysis, BMI was grouped into four categories: BMI <25 kg/m2 (underweight/normal weight), 25 to <30 kg/m2 (overweight), 30 to <40 kg/m2 (Class 1 and Class 2 obesity), and ≥40 kg/m2 (Class 3–5 obesity). We combined the CDC Class 1 and 2 obesity groups 17 due to the relatively small numbers in each of these subgroups.
Statistical analyses were performed using IBM® SPSS® Statistics version 25 (IBM Corp., Armonk, NY, USA). We report descriptive statistics for characteristics of our sample and type of treatment received. Associations among categorical variables were assessed using chi-square tests. Two-tailed p-values <0.05 were considered significant. Separate multivariable logistic regression models were used to identify variables that were independently associated with the probability of receiving (1) surgical (vs. medical) treatment, and (2) any medical or surgical treatment (vs. no treatment). We report adjusted odds ratios and 95% confidence intervals. A post hoc power analysis showed that we have >95% power to detect significant differences in a comparison of surgical to medical treatment only and in comparison of any to no treatment.
Results
Records of all 13,127 women seen in the Barnes-Jewish Hospital OBGYN Resident clinic from July 1, 2013 through June 30, 2017 were reviewed. Of the 2,154 women with ICD-9/ICD-10 codes consistent with a diagnosis of AUB, we excluded 306 who were <21 years and 19 who were >60 years at the time of their first resident-clinic visit during the study period, and thus presumptively beyond reproductive age. We also excluded 45 women with a diagnosis of gynecologic cancer, 42 women whose BMI could not be determined, and 37 women without insurance status data (Fig. 1). The final sample of 1,705 women with complete data for analysis was 93.2% of 1,784 resident-clinic patients with a diagnosis of AUB who did not have a diagnosis of cancer and were 21–60 years of age.
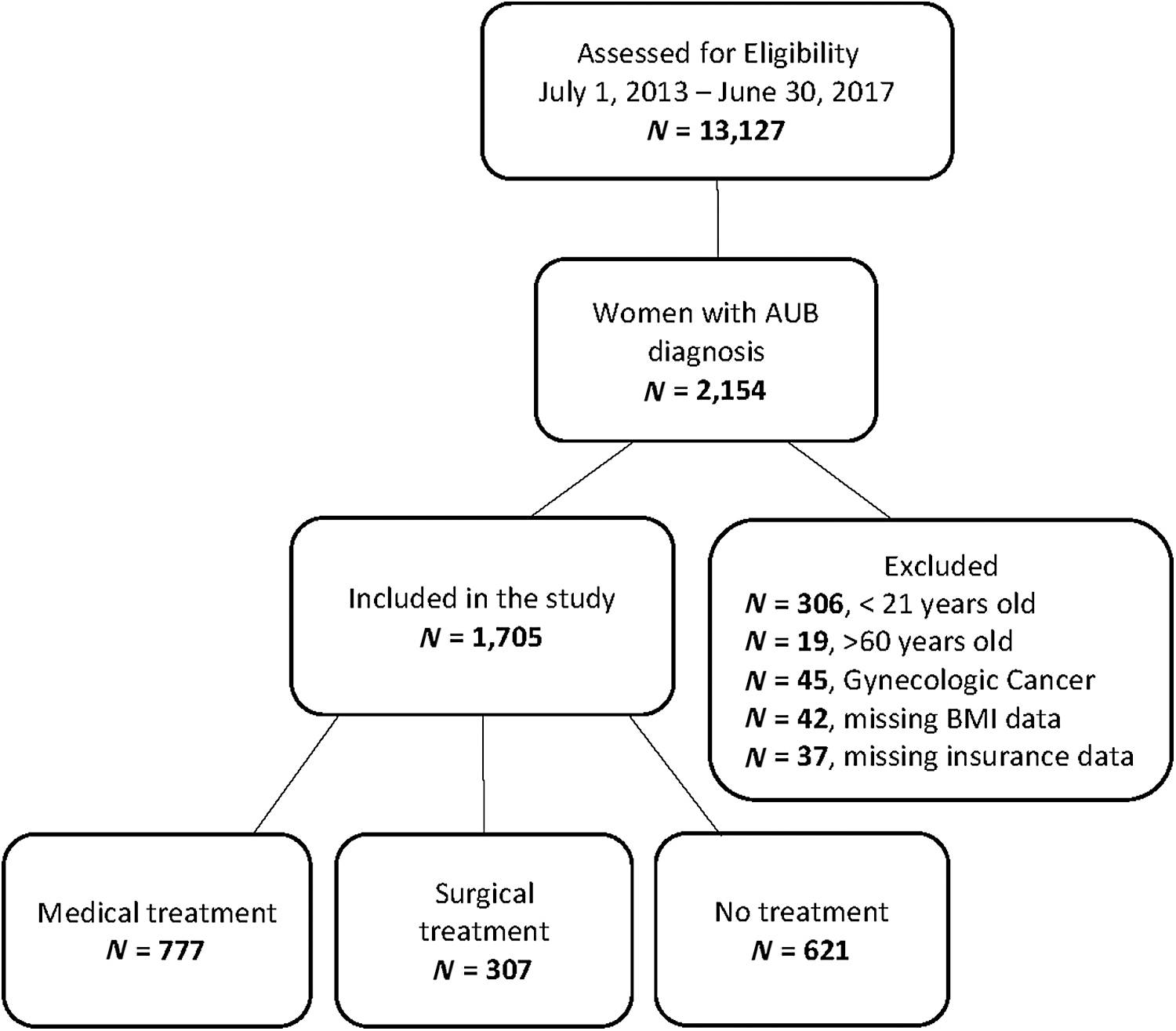
Resident clinic study sample selection process. AUB, abnormal uterine bleeding; BMI, body mass index.
As shown in Table 1, most patients in our study sample were Black/African American (67.7%), publicly insured (65.3%), age 21–40 (64.3%), and had a BMI ≥30 kg/m2 (62.6%). The Other race/ethnicity category included a heterogeneous group of 86 patients, 64 of whom were designated in the medical record only as “Other” race; the next largest group in this category included 17 Asian women. The Unknown category included 137 patients, 120 of whom were missing data. Of all 1,705 patients in our sample, 777 (45.6%) women received only medical treatment for AUB, 307 (18.0%) received surgical treatment (with or without medical treatment), and 621 (36.4%) received neither medical nor surgical treatment for AUB during the study period. In bivariate analyses, there were significant associations between each of the patient characteristics and treatment received except for insurance type (Table 1). Furthermore, there were significant associations among the various patient characteristics (each chi-square p < 0.05), except for the association between race/ethnicity and age (p = 0.44; data not shown). Notably, of 1,149 Black/African American patients, 796 (69.3%) were publicly insured and 753 (65.5%) were obese.
Characteristics of the Study Sample of Women with Abnormal Uterine Bleeding Seen in the Obstetrics & Gynecology Resident-Clinic July 1, 2013 Through June 30, 2017, by Treatment Received
Chi-square tests of significance.
The Other race/ethnicity category included designations of “Other,” Asian, Native Hawaiian/Pacific Islander, Native American/Alaska Native, “Multi-racial,” and Hispanic ethnicity.
The Unknown race/ethnicity category included designations of “Unknown,” “Declined” to respond, or data were not recorded.
BMI, body mass index.
Table 2 shows the results of two multivariable logistic regression models used to identify independent predictors of surgical (vs. medical) treatment and any (vs. no) treatment. In the first model, women in the 41–60 age group were more likely than women in the 21–40 age group to have had surgical (vs. medical) treatment. The Other race/ethnicity group was less likely than Black/African American patients to have received surgical treatment, but women who were White and Unknown race/ethnicity were as likely as Black/African American women to have received surgical treatment. Insurance status and BMI were not independently associated with receipt of surgical (vs. medical) treatment for AUB in this model.
Multivariable Logistic Regression Models to Identify Variables Associated with Surgical (Vs. Medical) Treatment for Abnormal Uterine Bleeding and with Any (Vs. No) Treatment Received in the Resident Obstetrics & Gynecology Clinic, July 1, 2013 Through June 30, 2017
Chi square tests of significance.
The Other race/ethnicity category included designations of “Other,” Asian, Native Hawaiian/Pacific Islander, Native American/Alaska Native, “Multi-racial,,” and Hispanic ethnicity.
The Unknown race/ethnicity category included patient-reported “Unknown” race/ethnicity, “Declined” to respond, or data were not recorded.
In the second model, women in the 41–60 age group were less likely than women in the 21–40 age group to have received any (vs. no) treatment. Women in the Unknown race/ethnicity group were less likely than Black/African American women to have received any treatment. However, women who were White and Other race/ethnicity were as likely as Black/African American women to have received any treatment. Insurance status and BMI were not independently associated with receipt of any (vs. no) treatment for AUB in this model.
Discussion
AUB is a common diagnosis among women in the United States, 1 and was present in 1,784 women of reproductive age without a diagnosis of cancer seen in our resident clinic during the study period. We found that among women with AUB who received treatment during the study period, race/ethnicity and age were independently associated with surgical (vs. medical) treatment decisions as well as with any (vs. no) treatment. BMI and insurance status were not independently associated with surgical treatment or any treatment for AUB. Our findings from analysis of our resident-clinic data are discussed in the context of the literature regarding treatment for noncancer-related AUB.
Our observation that women ages 41–60 who required treatment were more likely to receive surgical treatment than medical treatment for their AUB is consistent with knowing that most of these women have completed childbearing and may elect for definitive rather than conservative management options. An alternative reason may be the clinician's concern of failing medical treatment in older women due to a possible occult endometrial cancer. While a diagnosis of cancer was a reason for exclusion from our study, a recommendation for surgical treatment may reflect the uncertainty of diagnosis (such as the potential for an occult endometrial cancer) typical in evaluation and treatment of women with AUB. Such caution is consistent with utilizing a diagnosis of AUB rather than a final pathologic diagnosis as the pivotal decision point for our analysis. In addition, our finding that women 41–60 were less likely than women ages 21–40 to receive any treatment reflects the fact that many older women require only reassurance and watchful waiting once their evaluation is found to have a low probability for cancer. 3 Although this perimenopausal age group is less likely to need any treatment, if intervention is needed, it is more likely to be surgical than medical.
Compared with Black/African American patients, the Other race/ethnicity group was less likely to receive surgical management than medical management. Although our sample included 17 Asian women, an earlier cross-sectional survey study analyzing racial disparities in surgical management of benign gynecologic conditions found that among Asian women, hysterectomy rates were lower. 18 Asian women, compared with White women, were 56% less likely to receive a hysterectomy, and Black women were 66% more likely to receive a hysterectomy, in separate models fully adjusted for various clinical and demographic factors. 18 This suggests that factors such as cultural norms and preferences may contribute to the treatment decision-making process. Our finding that women in the Unknown race/ethnicity group were less likely than Black/African American women to receive any treatment should be interpreted with caution, as this was a small group that included patients who were primarily missing data entirely.
As our resident-clinic population includes predominantly Black/African American patients, we used this larger group as our reference category in the logistic regression models. A nonsignificant difference in treatment decisions between White and Black/African American patients may be due to the relatively small numbers of White patients in this resident-clinic patient population or to the shared variance between race/ethnicity and that of insurance status and BMI, as there were significant bivariate associations between race/ethnicity and these variables. Similarly, because very few patients had private insurance, a significant difference in treatment choices based on insurance status may not have been detectable.
We hypothesized that, among women requiring treatment for AUB, more obese women would be less likely to receive surgical than medical management secondary to higher potential for surgical complications and increased technical difficulty. 19,20 However, this hypothesis was not supported, suggesting that the presence of obesity as a risk factor for surgical complications did not preclude obese women from receiving surgery for AUB in the resident clinic. This observation is consistent with other findings in the literature, indicating that obesity itself is not an independent risk factor for postoperative morbidity. 21,22
Although BMI was not significantly associated with the odds of receiving surgical (vs. medical) management for AUB, the association between BMI and any (vs. no) treatment approached significance for women with BMI ≥40 kg/m2. While our study excluded women with a diagnosis of gynecologic cancer, clinicians who are presented with an obese patient with an unclear etiology for AUB may have higher suspicion for underlying premalignancy or malignancy, and thus favor treatment over observation. Prior studies have demonstrated an association between obesity and risk of endometrial hyperplasia or cancer among premenopausal women. 23,24 In addition, women with higher BMI may have chronic anovulation, which is unlikely to spontaneously resolve and therefore necessitate either medical or surgical management. The association between BMI and treatment decisions for AUB is worthy of further investigation.
A strength of our study lies in the large volume of women seen in our resident clinic, which yielded a sufficiently large study sample of women with AUB to allow us to test our hypotheses. In addition, focusing on patients with a diagnosis of AUB in the absence of cancer reflects the points of critical clinical decision making in the care of these patients.
Our study also has limitations. We used data from an administrative database in the OBGYN resident clinic at one, large, academic medical center. Our study population was largely Black/African American, 21–40 years old, obese, and publicly insured. Thus, our findings might not be generalizable to other patient populations. Our study design precluded examination of temporal relationships. We could not determine whether women who received surgical treatment had previously declined or failed medical treatment. Using administrative data precludes determination of a definitive cause for not receiving treatment during this study time frame. Many patients also might have received care for AUB elsewhere before entering our clinic system. In addition, we were unable to determine the exact reason for IUD insertion or removal, and presumed that this was related to medical treatment of AUB if contraception was not also coded. Administrative databases, in general, are limited by the type of data collected and the quality of diagnostic coding by providers; therefore, conclusions based on analyses of these data must be interpreted with caution. 25 A lack of data about comorbidities in our database is also a notable limitation, as comorbidities will have an impact on the treatment decision-making process.
In summary, older patients in the resident clinic who required treatment were more likely to have received surgical (vs. medical) treatment, but overall less likely to have received any (vs. no) treatment. Women in the Other race/ethnicity group were less likely than Black/African American women to receive surgical treatment. Obese women were neither more nor less likely than women with BMI <25 kg/m2 to receive surgical treatment or to receive any treatment. BMI and insurance status were not independently associated with treatment for AUB. Additional studies in larger and more diverse populations are warranted to assess whether obesity and other unmeasured variables are associated with treatment decisions for women with AUB, and if there are health care disparities in those decisions based on specific patient characteristics, such as race/ethnicity and BMI. The role of bias in treatment decisions leading to health care disparities also warrants investigation. Prospective studies would allow further insight into the care of women with AUB, especially among patients who receive multiple different treatments or who proceed to surgical management after medical management options have been exhausted.
Conclusions
Management of AUB differed significantly by age and race/ethnicity but not by BMI and insurance type. In this resident-clinic sample, women 41–60 years of age who required treatment were, not surprisingly, more likely to receive surgical treatment, although they were less likely to receive any (vs. no) treatment for AUB. To our knowledge, this study is the first to investigate the care of women of reproductive age with the broad diagnosis of AUB (excluding a cancer diagnosis) using an administrative database, and thus expands the literature on an understudied gynecologic topic and on health care disparities in treatment for women with AUB. Although our study examined patient characteristics that could be associated with healthcare disparities in AUB treatment, additional research is needed. To aid in future research about this topic, providers should clearly document their clinical decision-making process in management decisions, specifically if patients have exhausted or declined medical management options before proceeding to surgery and if comorbidities were considered in the choice of management options for AUB. Administrative databases are notoriously limited in this regard. Thus, planned data collection to answer research questions such as ours regarding potential disparities in clinical-management decisions for AUB are still needed, using a larger and more diverse sample of patients and examining clinical-treatment decisions in relation to other social determinants of health.
Footnotes
Authors' Contributions
Dr. Lulu Yu, Ms. Bhavana Janga, Dr. Rebecca McAlister, Dr. Donna Jeffe, and Dr. Tammy Sonn confirm that they meet the following criteria for authorship: (1) substantial contribution to the conception or design of the work; or acquisition, analysis, or interpretation of data for the work; (2) drafting the work or revising it critically for important intellectual content; (3) final approval of the version to be published; and (4) agreement to be accountable for all aspects of work in ensuring questions related to accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official view of the NIH.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication or project was supported by the Washington University Institute of Clinical and Translational Sciences grant (UL1TR002345) from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). In addition, we received internal grant funding from the Washington University Department of Obstetrics and Gynecology.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.