
Abstract
After its identification as a human pathogen in 2019, the novel coronavirus, SARS-CoV-2, has spread rapidly around the world. Health care workers worldwide have had the task of preparing and responding to the pandemic with little evolving data or guidelines. Regarding the protocols for our labor and delivery unit, we focused on applying the four pillars of biomedical ethics—beneficence, nonmaleficence, autonomy, and justice—while considering the women, their fetuses, their significant others and support persons, health care professionals and auxiliary staff, and society as a whole. We also considered the downstream effect of our decisions in labor and delivery on other disciplines of medicine, including pediatrics, anesthesiology, and critical care. This article focuses on how these prima facie principles helped guide our recommendations in this unprecedented time.
Introduction
Since its emergence as a human pathogen in 2019, the novel coronavirus, SARS-CoV-2, has spread rapidly around the world. As of September 8, 2020, Johns Hopkins University had tabulated 27,401,024 cases of COVID-19, the illness caused by SARS-CoV-2, in 188 countries, regions, or sovereignties. 1 Of these cases, 6,613,314 were in the United States. The virus had caused 893,871 deaths worldwide, including 189,366 deaths in the United States. 1
In response to the rapid spread of the virus, the World Health Organization characterized COVID-19 as a pandemic on March 11, 2020, 2 and the President of the United States declared a national emergency on March 13, 2020. 3
The pandemic has disrupted life in myriad ways. In the United States, state governors responded with executive orders closing schools, daycares, and businesses; restricting travel; prohibiting mass gatherings; imposing quarantines; and requiring other changes that have significantly impacted individuals and organizations, both public and private. 4 Other nations have enacted similar measures to address public health needs.
Health care workers worldwide have had the task of preparing and responding to the pandemic with a paucity of data, which is also evolving. For example, initial reports out of China showed that children exposed to COVID-19 did well, 5 whereas more recent data call that into question. 6 International and national medical guidelines have begun to appear, but they are often broad in scope and continue to require modifications. 7,8
In the hospital setting, each unit faces its own particular challenges. In the labor and delivery unit, patients arrive unscheduled, and physicians and staff care for both mother and fetus simultaneously. Maternal COVID-19 test status may affect care plans for infants and logistical approaches to caring for the mother, but procedures cannot always be safely delayed until results return. Furthermore, testing has not been broadly accessible for many institutions, and even when available, turnaround time impedes the usefulness of testing to inform patient care plans. Approximately 30% of women in the United States will need a cesarean delivery, 9 often unplanned, and it is not possible to predict in advance who may require general anesthesia with intubation, which is an aerosol-generating procedure that could spread COVID-19. 10
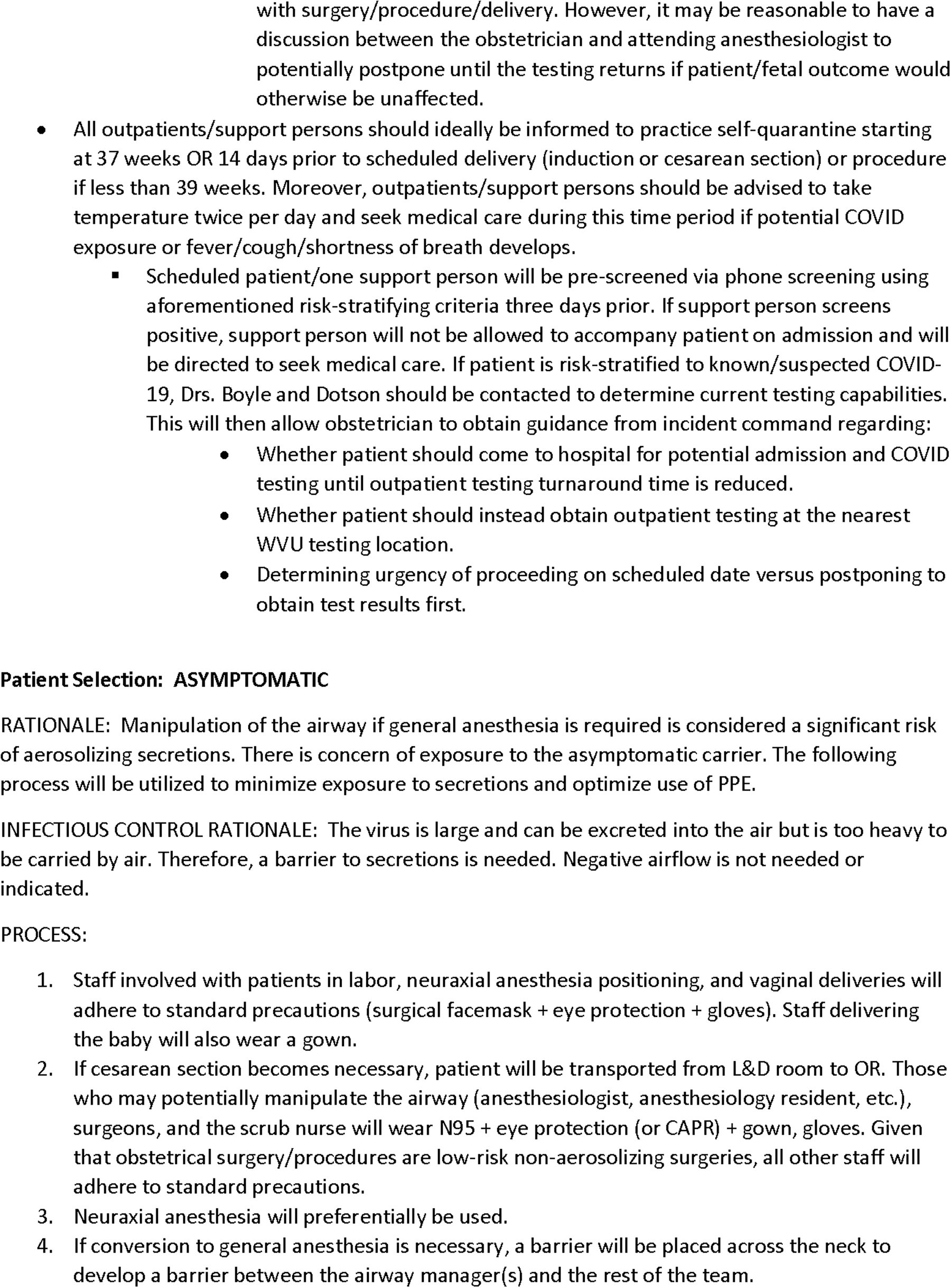
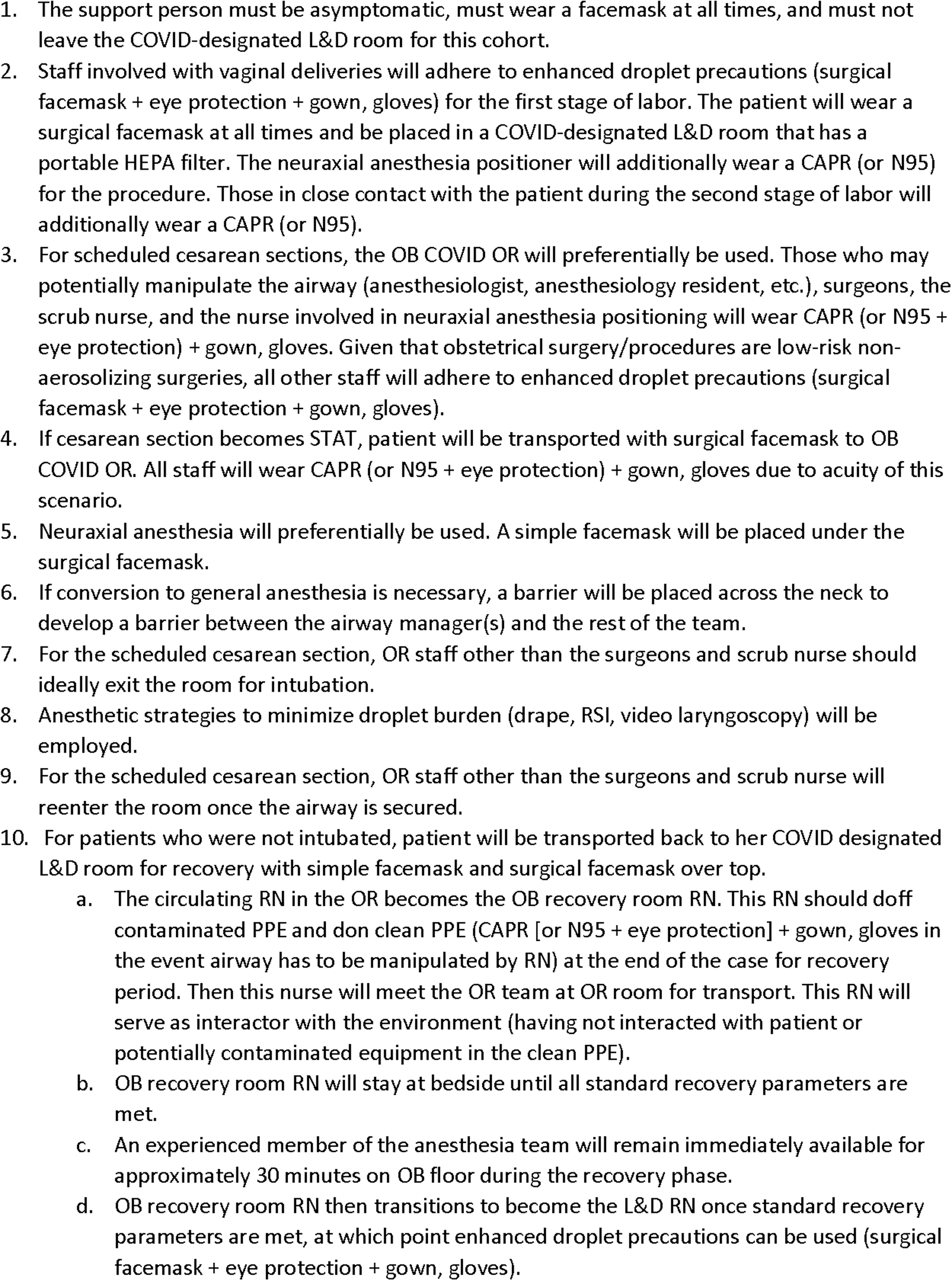
With broad guidance from national and international organizations, the authors were tasked with developing specific protocols for women who presented to the labor and delivery unit at West Virginia University Hospitals during the pandemic (Figs. 1 and 2).
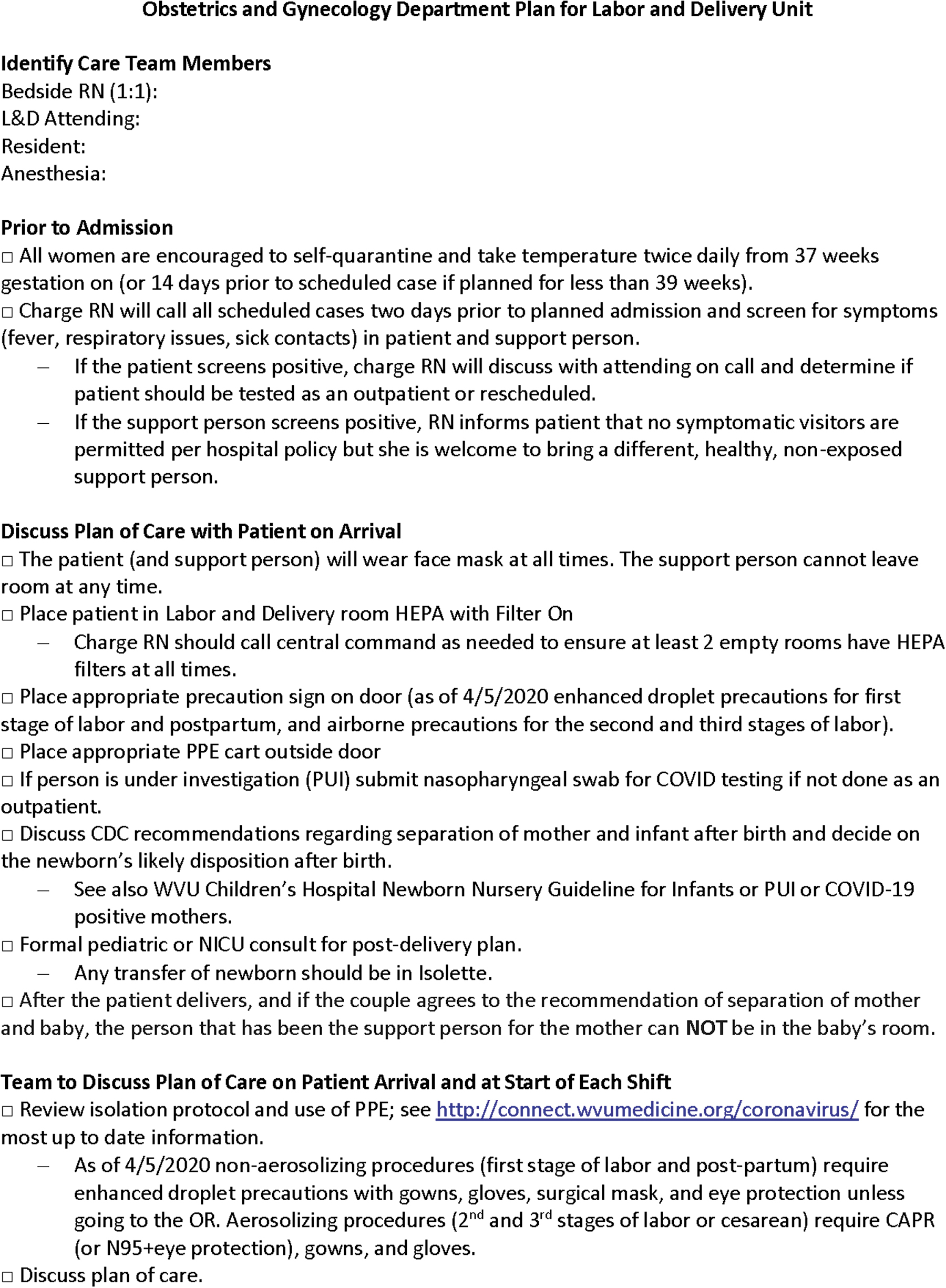
Obstetrics and gynecology department plan for labor and delivery unit.
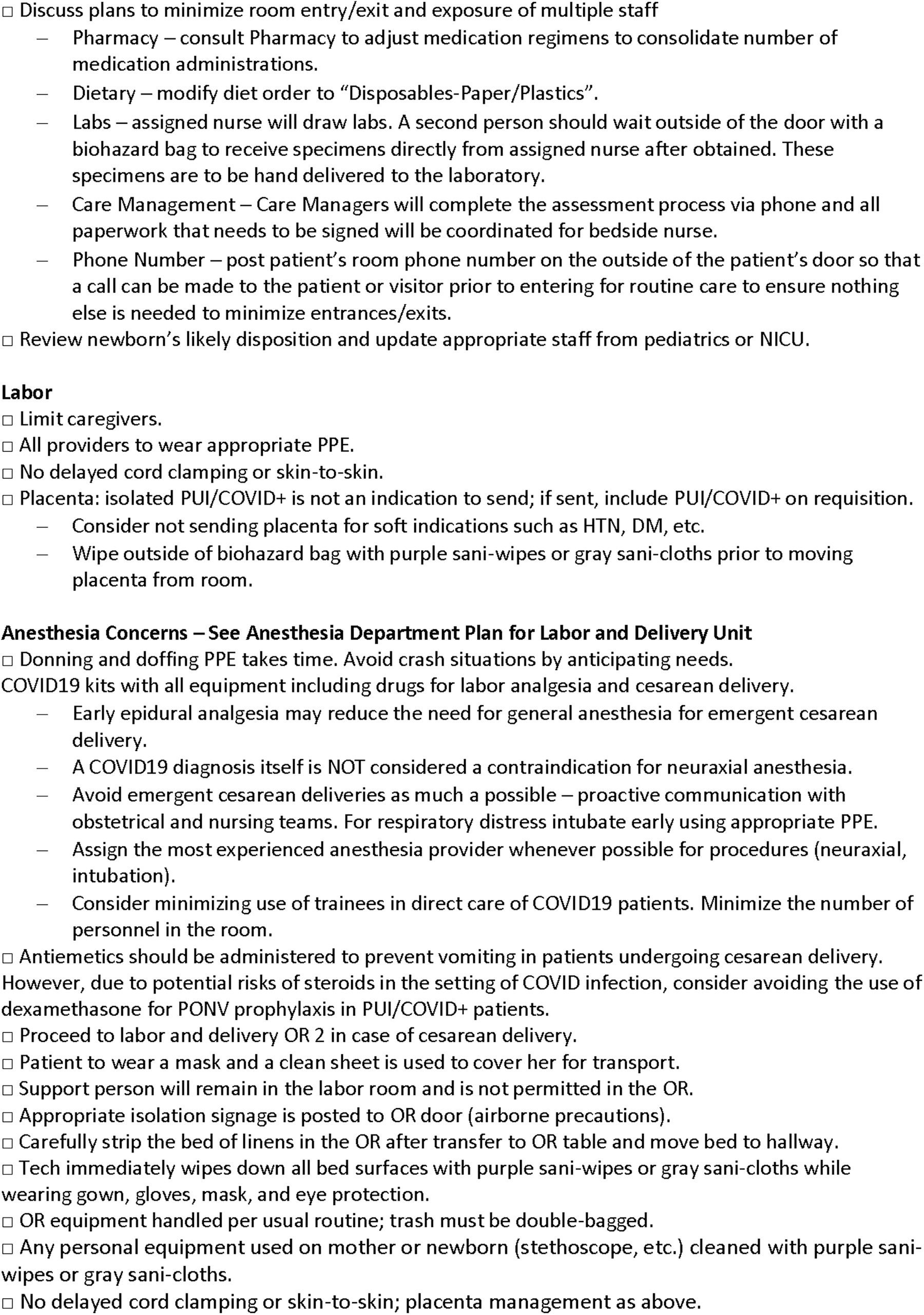

Anesthesia department plan for labor and delivery unit.



In developing our protocols, we focused on applying the four pillars of biomedical ethics—beneficence, nonmaleficence, autonomy, and justice 11 —while considering the women, their fetuses, their significant others and support persons, our health care professionals and auxiliary staff, and society as a whole. We also considered the downstream effect of our decisions in labor and delivery on other disciplines of medicine, including pediatrics, anesthesiology, and critical care. This article focuses on how these prima facie principles helped guide our recommendations in this unprecedented time.
Beneficence versus nonmaleficence
Discussions of biomedical ethics often focus almost exclusively on patients, but as COVID-19 is contagious through asymptomatic transmission, 12 we expanded our focus to include health care workers, the health care system, and society as a whole. Many of our hardest decisions while developing protocols for women in labor during this pandemic have been made in an effort to meet the needs of our patients while trying to mitigate the risks to our staff.
To curb the spread of the virus and protect frontline workers, West Virginia University Hospitals restricted visitors in the inpatient setting and eliminated them in the outpatient setting. Our concern was that limiting support for laboring women could be psychologically damaging and that it could push women toward out-of-hospital births, without being fully informed that the neonatal morbidity is twice that of in-hospital births. 13 –15 Therefore, we advocated women have a support person for labor and delivery, as well as postpartum recovery, but we limited that to one individual. The hospital administrators accepted this and additionally made exceptions for visitors for end-of-life care, those with limited capacity, and pediatric patients. The question of a doula being allowed as a second support person was discussed, but we believed this could (1) result in a two-tiered system where women with more resources would have more support than women with fewer resources and (2) create a loophole for women to bring in additional family members or friends. Therefore, we ultimately did not make an exception for doulas.
In an effort to protect staff, we have stressed frequent communication through team huddles, minimizing the use of trainees in direct care of known or suspected COVID-19 patients, and limiting the number of personnel in a patient's room. We do not allow symptomatic or potentially exposed support persons, and we screen all patients with scheduled procedures, such as cesarean delivery or induction of labor 3 days before their admission date and again upon entry to the hospital. A woman who is suspected or known to have COVID-19 is instructed to wear a mask at all times. Support people are required to wear a mask any time they are outside a patient's room.
We recommend quarantine for all women and their support person from 37 weeks gestation on, or 14 days before a scheduled delivery if the delivery is planned for <39 weeks gestation. Recognizing that this has the potential to affect a family's income and to shorten parental leave after birth, which could impact bonding with the baby, quarantine is not mandated. Such a mandate would be unenforceable in any case.
In the operating rooms situated in the labor and delivery unit at our hospital, we are unable to use portable high-efficiency particulate air (HEPA) filtration or negative pressure. In developing our COVID-19 protocols, we weighed this against the fact that surgeries and procedures in the labor and delivery unit are generally considered to be low risk for viral transmission and nonaerosolizing, given the preference for neuraxial anesthesia and infrequent need for general anesthesia in this patient population. We decided not to transfer women with known or suspected COVID-19 outside the unit if a cesarean section is indicated, which also offers logistical advantages, such as access to commonly used equipment and medications, as well as a sense of familiarity with and proximity to the primary team.
In each of these examples we attempted to strike a balance between what would be most beneficial to a woman and her family, and what would present the lowest risk of infection to hospital personnel. We recognize that there is the potential for harm with each decision we made, but we carefully considered the principles of beneficence and nonmaleficence in arriving at these decisions.
Autonomy
At the most basic level, autonomy can be defined as the ability of a person to make his or her own decisions. In developing our protocols, we focused on providing information to women to allow them to make informed decisions, which we then respected. Examples of how we respect women's autonomy in our protocols include (1) education to allow women to make informed decisions about an epidural and (2) discussions about the Centers for Disease Control and Prevention (CDC) recommendation to separate a woman who is positive for COVID-19 from her newborn(s). 16 These examples, and our decisions, are examined as follows.
As part of our protocols, we encourage, but do not compel, an early epidural in laboring women, especially those with known or suspected COVID-19, to avoid the risks inherent in urgent or emergent general anesthesia. This is discussed with women upon admission and again at their request. With general anesthesia, in addition to the risks of aspiration and fetal exposure to anesthetic, intubation may potentially spread droplet burden through aerosolization and cross-contamination. To avoid emergent cesarean deliveries as much as possible, we encourage proactive communication among the obstetric anesthesiologists, obstetricians, and obstetric nurses. The most experienced anesthesiologist, whenever possible, performs neuraxial anesthesia, and if necessary intubation, so as to limit the possibility of complications.
The CDC's original recommendation was to separate women who are COVID-19 positive from their neonates. As of May 20, 2020 they revised that recommendation to “strongly consider.” 16 When devising our protocols, we felt that the original recommendation was made with limited data and did not seem to consider the fact that women and their babies would likely be returning to the same home after delivery. 16 We felt that infant separation should be an individual decision, as opposed to the standard of care. Therefore, our protocols do not recommend or mandate separation. Instead, they call for discussion with a woman and her support person upon arrival to labor and delivery, during which we provide the rationale for the CDC recommendation and offer a formal pediatric or neonatology consult for postdelivery planning. Only after a woman has been given the appropriate information is a neonatal disposition made; this is ultimately based on the mother's wishes. We varied from the CDC's original recommendation in an effort to support women's autonomy.
Justice
The components of justice include equity and equality. This comes into play when considering resource allocation to our unit versus the remainder of the hospital. On a national and local level, allocation of resources during the COVID-19 pandemic has been challenging. HEPA filters and negative-pressure rooms are a limited commodity. There are also national shortages of personal protective equipment for frontline staff.
In our hospital, anesthesiologists were among the first to get personal N95 respirator masks, given their frequent potential exposure to the virus during intubation. Outside the labor and delivery unit, the anesthetic plan requires anyone not involved with intubation to step out of the room or stand >6 feet (>1.8 meters) away from the patient distal to a drape that is placed a few inches caudad to the patient's head. This is not feasible or realistic during an emergency delivery requiring general anesthesia because of the time-sensitive nature of such an event in trying to minimize maternal and fetal complications and fetal exposure to anesthetic.
We were able to effectively advocate for our staff and secure personal protective equipment so that all staff can don a powered air-purifying respirator (or N95 mask plus eye protection). It was debated if the second stage of labor (pushing) also has a risk of viral spread but securing the appropriate personal protective equipment for staff to use during a cesarean delivery also facilitated its availability for vaginal delivery.
Another issue of justice is whom to test for COVID-19. Given the low prevalence of this disease in West Virginia at this time—248 deaths and 8581 recoveries of September 8, 2020 17 —we have deferred universal screening for the time-being. We have taken a heightened approach to standard precautions with all patients. If patients have fever, cough, or shortness of breath of unknown etiology or have had potential exposure to people who are positive for COVID-19, for example, imprisoned patients or immediate family members with the disease, these patients are tested. We understand that other hospitals may make different decisions and that our own policy may change as the situation evolves.
Conclusions
When the authors were called to assist in West Virginia University Hospitals' COVID-19 response, we quickly perceived that our development of protocols during the pandemic required specific attention to biomedical ethics. Recognizing that our response had to meet the needs of the women we serve while also protecting our staff, we employed the pillars of beneficence, nonmaleficence, autonomy, and justice to help guide our development of protocols for labor and delivery. This approach helped us frame important questions and balance competing needs. Feedback from stakeholders has been generally favorable as most recognize that these are historic and evolving times.
Since we were creating protocols for a specific hospital unit, certain issues are out of the scope of this article, such as allocation of resources on an international level and the ethics of out-of-hospital birth in the United States. In addition, our protocols may not be generalizable to other institutions with different patient populations, different prevalence of the novel coronavirus, and unique supply-chain issues, such as personal protective equipment availability and preservation techniques, as well as testing capabilities.
As the COVID-19 pandemic evolves, so will our knowledge and guidelines. However, with this and future challenges, a bioethical framework can be used as a guide in developing protocols that are equitable, while further research will guide evidenced-based best practices for health care during a global pandemic.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.