
Abstract
Background:
Maternal subclinical hypothyroidism (SCH) has been associated with adverse pregnancy outcomes. This study aimed to explore whether SCH in the first trimester contributed to the development of gestational diabetes mellitus (GDM).
Materials and Methods:
A total of 8,777 pregnant women who first visited before 13 weeks and 6 days of gestation and accepted routine prenatal service at the Third Affiliated Hospital of Sun Yat-Sen University from January 2015 to September 2018 were recruited in this study. Thyroid functions (thyroid stimulating hormone [TSH], free T4, and thyroid peroxidase antibody [TPOAb]) were measured before 13 weeks and 6 days of gestation and data of 7,536 subjects with TSH ≥0.1 mIU/L were analyzed. A 2-hour 75-g oral glucose tolerance test was performed between 24 and 28 gestational weeks. Chi-square test and multivariate logistic regression analysis were applied to evaluate the relationship between SCH and GDM.
Results:
The prevalence of SCH in this population was 7.53%. After stratifying the relationship between SCH and GDM according to TSH concentrations (slightly elevated TSH: ≥2.5, <4.0 mIU/L; moderately elevated TSH: ≥4.0, <10.0 mIU/L) and TPOAb status, a moderately elevated TSH combined with positive TPOAb (23.9% vs. normal 13.0%, chi-square = 6.317, p = 0.012) was found to increase the incidence of GDM. Furthermore, after adjusting for confounders (maternal age, educational levels, parity, and pregestational body mass index [preBMI]), the SCH group still exhibited a higher risk of GDM (relative risk [RR] 1.867, 95% confidence interval [CI] 1.018–3.424).
Conclusion:
Our findings indicated that SCH during early pregnancy, in the presence of moderately elevated TSH levels and positive TPOAb, might lead to an increased risk of GDM.
Introduction
Due to the increased serum concentrations of human chorionic gonadotropin and thyroxine-binding globulin, the concentrations of thyroid stimulating hormone (TSH) and circulating thyroid hormones differ from that observed in nonpregnant women. 1 In addition, maternal thyroid disorders, especially those in early pregnancy, may lead to adverse obstetric complications and affect the health status of the offspring. 2 Subclinical hypothyroidism (SCH) is one of the common thyroid disorders during pregnancy, and is characterized by an elevated TSH and a normal free thyroxine 4 (fT4). 3 SCH is associated with adverse pregnancy outcomes, 4,5 and has been reported to affect up to 15% of pregnant women in the United States and 28% in China. 6,7 According to the criteria published in the 2011 American Thyroid Association (ATA) guidelines, the upper limits of TSH were 2.5 mIU/L in the first trimester and 3.0 mIU/L in the second and third trimesters. However, SCH might be overdiagnosed using this criterion, and an upper reference limit of 4.0 mIU/L for TSH was thus recommended in the 2017 ATA guidelines. 8 Whether slightly elevated TSH levels are related to adverse pregnancy outcomes remains controversial, and the role of thyroid peroxidase antibody (TPOAb) should also be taken into account since the presence of TPOAb increases the risk of thyroid dysfunction during pregnancy. 2,9,10
Gestational diabetes mellitus (GDM), which is defined as “any degree of glucose intolerance with the onset or first recognition during pregnancy,” represents another highly prevalent endocrine disorder during pregnancy. Insulin resistance and glucose intolerance are critical for the pathophysiology of diabetes. 11 In nonpregnant peoples, hypothyroidism has been highlighted for its involvement in diabetes mellitus (DM). 12 The lack of thyroid hormone is associated with insulin resistance and glucose intolerance. 13 Nonetheless, whether elevated TSH in pregnant women with SCH confers an effect on glucose metabolism and promotes GDM development remains controversial. Herein, with the aim to further examine the effects of SCH on GDM during early pregnancy, we divided TSH into slightly elevated levels (2.5 ≤ TSH <4.0 mIU/L) and moderately elevated levels (4.0 ≤ TSH <10.0 mIU/L) and took TPOAb status into consideration.
Materials and Methods
Subjects
The current study was conducted at the Third Affiliated Hospital of Sun Yat-Sen University from January 2015 to December 2018. A total of 8,777 women who first screened before 13 weeks and 6 days of gestation and accepted routine prenatal service were included in the study. The exclusion criteria included the following: personal history of thyroid diseases (n = 124), multiple pregnancies (n = 68), pregestational DM (n = 46), usage of drugs that may influence thyroid function (n = 72), and received no oral glucose tolerance test (OGTT) during 24–28 gestational weeks (n = 230). A schematic for this experiment design is shown in Figure 1.
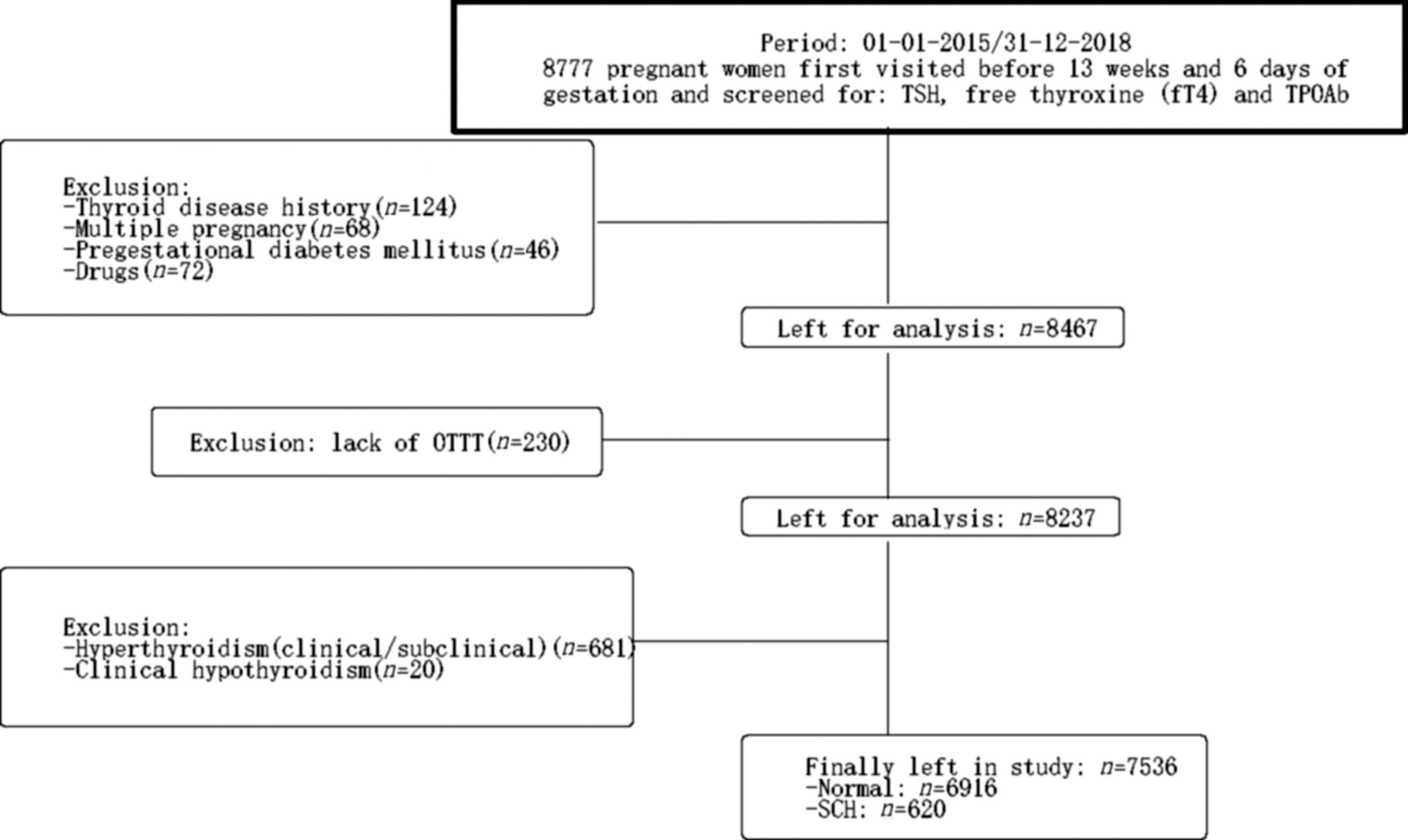
Flowchart showing the women selected in the study. fT4, free thyroxine 4; OGTT, oral glucose tolerance test; SCH, subclinical hypothyroidism; TPOAb, thyroid peroxidase antibody; TSH, thyroid stimulating hormone.
Methods
The current study was approved by the Human Research Ethics Committee of the hospital and conducted in strict accordance with the Declaration of Helsinki. Signed informed consents were obtained from all participants before enrollment. Following enrollment, thyroid function tests were measured at their first visit to the hospital before 13 weeks and 6 days of gestation. Serum samples were obtained in the morning after at least an 8-hour fasting. Serum TSH, fT4, and TPOAb levels were measured at a clinical analysis laboratory by using an automated two-step chemiluminescent immunoassay on an ARCHITECT analyzer (Abbott Diagnostics). The normal range of TSH in the first trimester was 0.1 – 2.5 mIU/L, according to the 2011 ATA guidelines. 14 The reference ranges of TPOAb (<5.61 IU/mL) and fT4 (9.01–19.05 pmol/L) were provided by the manufacturer. TPOAb was considered positive if levels were ≥5.61 IU/mL. Of the 8,237 qualified women, those who met any of the following criteria were excluded: clinical and subclinical hyperthyroidism (TSH <0.1 mIU/L) (n = 681) and clinical hypothyroidism (TSH ≥2.5 mIU/L and fT4 < 9.01 pmol/L) (n = 20). Thus, a total of 7,536 pregnant women were recruited in the final analysis, including 6,916 healthy women (TSH: ≥0.1, <2.5 mIU/L) and 620 SCH women (TSH ≥2.5, <10.0 mIU/L) (Fig. 1).
Baseline characteristics of these subjects were also recorded at the patient's first visit before 13 weeks and 6 days of gestation, which included age, pregestational body mass index (preBMI), which was calculated by using the formula: BMI = weight (kg)/height (m2), parity, personal history of diseases (thyroid disease, hypertension, pregestational DM, and systemic lupus erythematosus), medications, and education levels.
One-step diagnosis was used for GDM. A 2-hour 75-g OGTT was performed between 24 and 28 weeks in the morning after at least an 8-hour fasting. Blood glucose levels were measured by using the glucose oxidase method (Roche Diagnostics). The diagnostic criteria for GDM were based on the International Association of Diabetes and Pregnancy Study Groups (IADPSG), that is, one or more plasma venous glucose values ≥0 hour, 5.1 mmol/L; 1 hour, 10.0 mmol/L; or 2 hours, 8.5 mmol/L. 15
Statistical analysis
SPSS 19.0 software (IBM Corp., Armonk, NY) was used for data analysis. Data were presented as median (interquartile range) for non-normally distributed data and frequency (percentage) for categorical variables. Chi-square test was performed to analyze the differences in variables between groups. Multivariate logistic regression analysis was applied to evaluate the correlation between SCH and GDM. The results were represented as relative risk (RR) and 95% confidence interval (95% CI). p < 0.05 was considered statistically significant.
Results
Following initial inclusion and analyses, the prevalence of SCH was 7.53% (620/8,237) in this population. Of the 7,536 studied women, 620 were diagnosed with SCH and 6,916 were normal. The characteristics of these participants are shown in Table 1. The average concentrations of TSH in the SCH group and the normal group were 3.02 (2.72–3.90) mIU/L and 0.98 (0.58–1.45) mIU/L, respectively. Meanwhile, blood glucose levels during 75-g OGTT presented with no obvious differences between the SCH group and the normal group at three time points [0 hour: 4.18 mmol/L (3.99–4.38) vs. 4.16 mmol/L (3.97–4.39), p = 0.594; 1 hour: 7.65 mmol/L (6.73–8.66) vs. 7.79 mmol/L (6.83–8.85), p = 0.072; and 2 hours: 6.58 mmol/L (5.75–7.55) vs. 6.67 mmol/L (5.81–7.66), p = 0.163, respectively]. In addition, no significant differences were observed in regard to the age and preBMI between the two groups (all p > 0.05). However, there were more nullipara (57.90% vs. 50.40%, p < 0.001) and low-educated women (19.19% vs. 15.88%, p = 0.032) in the SCH group than in the normal group.
Clinical Characteristics of Subclinical Hypothyroidism and Normal Pregnant Women
Medians (interquartile ranges).
BMI, body mass index; fT4, free thyroxine 4; OGTT: oral glucose tolerance test; SCH, subclinical hypothyroidism; TPOAb: thyroid peroxidase antibody; TSH, thyroid stimulating hormone.
As shown in Table 2, 7,536 pregnant women were further divided into the following subgroups according to TSH levels: the normal group: TSH ≥0.1, <2.5 mIU/L; the slightly elevated group: TSH ≥2.5, <4.0 mIU/L; and the moderately elevated group: TSH ≥4.0, <10 mIU/L. Chi-square test was then performed to compare the prevalence of GDM between the subgroups. It was found that moderately elevated TSH levels rather than slightly elevated TSH levels increased the incidence of GDM (20.1% of the moderately elevated group vs. 13.8% of the normal group, chi-square = 4.738, p = 0.029; 13.4% of the slightly elevated group vs. 13.8% of the normal group, chi-square = 0.046, p = 0.831). In addition, TPOAb status (TPOAb-negative or TPOAb-positive) was further analyzed. It was found that in TPOAb-negative women, the prevalence of GDM was not increased with elevated TSH levels (13.6% of the slightly elevated group vs. 13.9% of the normal group, chi-square = 0.020, p = 0.887; 12.9% of the moderately elevated group vs. 13.0% of the normal group, chi-square = 0.000, p = 0.999). However, in TPOAb-positive women, the prevalence of GDM was observed to be significantly increased in the moderately elevated group (23.9% vs. 13.0% of the normal group, chi-square = 6.317, p = 0.012), but not in the slightly elevated group (16.9% vs. 13.9% of the normal group, chi-square = 0.554, p = 0.457).
GDM Risk Analysis of Subclinical Hypothyroidism Women with Differently Elevated TSH Levels and TPOAb Status in the First Trimester
GDM, gestational diabetes mellitus.
The upper limit was 10.0 mIU/L.
As shown in Table 3, multivariate logistic regression analysis was then performed to further investigate whether SCH in the first trimester was associated with GDM. It was found that among TPOAb-negative women, after adjusting for confounders (age, preBMI, parity, and educational level), elevated TSH levels showed no correlation with GDM (all p > 0.05). However, among TPOAb-positive women, moderately elevated TSH levels [unadjusted model: RR (95% CI): 2.468 (1.392–4.377), p = 0.002; adjusted model: RR (95% CI): 1.867 (1.018–3.424), p = 0.044] rather than slightly elevated TSH levels [unadjusted model: RR (95% CI): 1.000 (0.588–1.699), p = 0.999; adjusted model: RR (95% CI): 1.072 (0.621–1.851), p = 0.802] exhibited effects on the prevalence of GDM in both unadjusted and adjusted models. Moreover, 155 subjects among the 620 subjects with TSH ≥2.5 mIU/L received levothyroxine treatment, and 26 subjects (16.8%) of them developed GDM; in contrast, 69 subjects (14.8%) of the 465 untreated subjects developed GDM (chi-square = 0.336, p = 0.562).
Multivariate Logistic Regression Analysis of the Relationship Between Subclinical Hypothyroidism in the First Trimester and Gestational Diabetes Mellitus
Adjustment for maternal age, maternal preBMI, parity, and educational level.
The upper limit was 10.0 mIU/L.
preBMI, pregestational BMI; RR, relative risk.
Discussion
The purpose of the current study was to evaluate whether SCH in the first trimester exerted any effects on the risk of GDM. First, in accordance with the 2017 ATA guidelines, 8 we subdivided SCH patients into two groups based on different degrees of the elevation in TSH levels (the slightly elevated group and the moderately elevated group) to evaluate the relationship between increased levels of TSH and GDM in a more accurate way. Our findings indicated that only maternal SCH with moderately elevated TSH levels and positive TPOAb in the first trimester increased the risk of GDM. In addition, we also performed a multivariate logistic regression analysis to adjust the confounders (maternal age, parity, educational levels, and preBMI), and the results further verified the conclusion.
Currently, whether SCH has an impact on GDM is still debatable. In a large meta-analysis comprising 35,350 pregnant women, Toulis found that the risk of GDM was substantially increased in SCH women (odds ratio [OR] 1.35, 95% CI: 1.05–1.75). 16 Similarly, another meta-analysis reported a similar result (OR 1.56, 95% CI: 1.29–1.88), in which pregnant women with SCH presented with an increased risk of GDM. 17 Meanwhile, the meta-analysis performed by Jia et al. revealed that pregnant women with SCH and positive antithyroid autoantibodies markedly increased the risk of GDM (OR 3.22, 95% CI: 1.72–6.03). 18 In agreement with the aforementioned previous studies, our cohort analysis further indicated that SCH women with moderately elevated TSH levels and positive TPOAb led to an increased risk of GDM (RR 1.867, 95% CI: 1.018–3.424). On the contrary, in Arbib's study, 2 by using similar TSH cutoffs, they failed to find the relationship between SCH in the first trimester and GDM. A possible explanation for the aforementioned discrepancy may be different ethnicities and lack of TPOAb measurement. However, in Chen' s study, 5 they selected the same ethnic women as us, yet they failed to find the similar effect of SCH on GDM development (the euthyroid group vs. the SCH group: 3.734% vs. 2.156%, p = 0.112). It was notable that their research included women with SCH throughout the pregnancy instead of only those with SCH limited to early pregnancy as was the inclusion protocol in our study. Moreover, the usage of different instruments and equipment for the test (Beckman vs. Abbott) and different cutoffs for the diagnosis (local trimester-specific reference values vs. ATA diagnostic criteria) might also precipitate inconsistencies in our findings.
Furthermore, elevated levels of TSH are also found to influence the relationship between SCH and GDM. One study even highlighted the direct relationship between increasing levels of TSH and the incidence of GDM. 19 Moreover, our previous study 4 and some other studies 20,21 further substantiated that the slightly elevations in TSH did not amplify the risk of adverse pregnancy outcomes. Expanding on our previous knowledge, our current findings unveiled that moderate elevations (≥4.0, <10.0 mIU/L) rather than slight elevations (≥2.5, <4.0 mIU/L) in TSH precipitated an increased risk of GDM. In addition, we also uncovered evidence indicating that the upper normal range of TSH in the first trimester was much higher than 2.5 mIU/L. These findings suggested the necessity of upregulating the upper reference limit for TSH to facilitate a more accurate assessment of pregnancy prognosis, and, in this regard, a higher TSH upper normal range of 4.0 mIU/L was recommended in the 2017 ATA guidelines.
In addition, the status of TPOAb also plays a role in regard to the effects of SCH on GDM. Our data illustrated that elevated TSH levels accompanied by positive TPOAb augmented the risk of GDM. This finding corroborated several published reports. For instance, Männistö et al. 22 reported that pregnant women with thyroid disease and abnormally high thyroid antibody levels were at a high risk for later developing noninsulin-dependent DM. Meanwhile, Ying et al. 23 also found that elevated TSH levels combined with positive TPOAb in the first trimester were associated with an increased risk for GDM, while those with negative TPOAb did not show this correlation, which was very much in accordance with our findings. Taken together, it would be prudent to elucidate the role of TPOAb status in the interaction between SCH and GDM in future endeavors.
What is noteworthy was that a large national U.S. data set analysis revealed that thyroid hormone treatment might also affect the relationship between SCH and GDM during pregnancy, as reflected by the increased risk of GDM in SCH women who received thyroid hormone therapy. 24 In the current study, we failed to ascertain the aforementioned correlation between thyroid hormone therapy and GDM, which might be attributed to the small sample size.
Nevertheless, our study presented with its own strengths. First, this was a large population-based cohort. Second, we evaluated the relationship between SCH and GDM by using the new TSH cutoff value of 4.0 mIU/L in the first trimester. Furthermore, we adjusted the potential confounders in our analyses. Simultaneously, there were also some limitations in our research. First, we performed a single-center study, which might limit the widespread application of our findings. Second, we did not establish the trimester-specific reference values for thyroid function in our center. Due to the presence of substantial variations between populations, elevations in serum TSH concentrations during pregnancy should ideally be defined by using pregnancy- and population-specific reference ranges. Thus, further studies are still required to confirm our findings.
Conclusion
Altogether, the findings obtained in our study elucidated that SCH in early pregnancy resulted in an increased risk of GDM in the presence of moderately elevated TSH levels and positive TPOAb. Our study suggests that the assessment of thyroid function in early pregnancy may be necessary and that OGTT should be carried out earlier for SCH women.
Footnotes
Authors' Contributions
All authors have read and approved the content, and agree to submit it for consideration for publication.
Acknowledgments
The authors thank all the doctors working in the Department of Obstetrics and Gynecology of the Third Affiliated Hospital of Sun Yat-sen University for their immense help in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a research grant from the Science and Technology Planning Project of Guangdong province (2017A020215026).