
Abstract
Background:
Hormonal contraceptive use is common among reproductive-aged women, but research evaluating its etiological relationship to vulvodynia remains mixed. We sought to evaluate this association and examine the potential for bias due to care-seeking behavior.
Materials and Methods:
We conducted a case–control study of women recruited from a large health care network database from 2008 to 2011. Of 26,455 eligible respondents, 1168 met the case definition for chronic vulvar pain (CVP). We matched each case to three controls by age and used conditional logistic regression to calculate odds ratios (ORs) for prior hormonal contraception (HC) use and CVP, stratifying cases by whether or not they sought care for their vulvar pain. We also simulated the influence of potential biases due to care seeking, using parameters based on this dataset.
Results:
HC users had higher odds of CVP (adjusted OR = 2.6, 95% confidence interval [CI]: 2.2–3.2). Effect estimates were stronger when cases were restricted to care seekers (adjusted OR = 2.9, 95% CI: 2.2–3.7). Effect estimates decreased slightly as time increased between HC initiation and pain onset. Our simulations suggested that effect estimates may be spuriously strengthened when cases are restricted to care-seeking women, but controls are recruited from the general population.
Conclusions:
Our results suggest an association between antecedent HC use and CVP that is potentially spuriously strengthened in case–control studies when cases are restricted to care seekers but controls are not.
Introduction
Vulvodynia causes persistent pain present for at least 3 months that can be localized to the vulvar vestibule, or as more generalized vulvar pain, and has no identifiable cause. 1 Population-based studies report a point prevalence of 7%–8% and a lifetime incidence of 16%. 2,3 Vulvodynia adversely affects quality of life, with women reporting sexual and relationship issues, anxiety, and depression. 4
Despite its high prevalence and considerable impact, the causes of vulvodynia remain largely uncharacterized, although vulvodynia is generally understood to be multifactorial. 5 One important potential determinant is the use of hormonal contraception (HC). Vaginal tissue is sensitive to hormonal changes, 6 and HC use has been associated with morphological changes in vaginal tissue that may be related to pain. 7 –9 Because HC use is common among reproductive-aged women, 10 elucidating its effects on vulvodynia is critical.
Case–control studies with participants recruited from vulvovaginal clinics have consistently reported a positive association between HC and vulvodynia. 11,12 Some studies further suggest that the association strengthens with younger age of contraception initiation and longer length of use. 11,12 Alternatively, studies with population-based recruitment have found associations that are smaller 13,14 or null. 15
A possible explanation for the discrepancy is selection bias. Selection bias in the context of effect estimation occurs when the measure of association estimated from a sample differs from what would have been observed had the entire target population been included. Selection bias occurs when selection into a study is dependent on a factor that is related to the exposure and outcome under study. 16 Selection bias is particularly common in case–control studies because sampling is integral to its design: cases are disproportionately oversampled, and controls are sampled with the goal of representing the distribution of exposure in the target population. 17 Because of the relative rarity of vulvodynia, and the fact that a detailed clinical examination is required to confirm a diagnosis of vulvodynia, case–control studies are frequently used for etiologic studies of vulvodynia.
Clinic-based study recruitment restricts the sample to women actively seeking care. Approximately 40% of women with chronic vulvar pain (CVP) do not seek medical care. 18 In the United States, women who use HC are also more likely than nonusers to seek care, because this contraception requires a health care provider prescription. Harlow et al. 14 compared prior use of oral contraception among vulvodynia cases recruited in a clinic, with use among cases recruited from the general population, and found that clinic-based cases were almost twice as likely to have used oral contraceptives. Therefore, studies evaluating the association between HC and vulvodynia may need to address the potential influence that care-seeking behavior may have on observed effect estimates to make informed decisions about study design and recruitment.
We used data from a large community-based sample of women in the Midwestern United States, including women who did and did not seek care for CVP, to investigate the potential for bias due to sampling strategy in assessing the relationship between HC use and CVP. We compared effects estimated in the overall population and when cases were separated into groups defined by whether or not they reported seeking care for their vulvar pain.
Materials and Methods
Study sample and design
We used data from a self-administered screener survey questionnaire sent to 66,857 women 18–40 years old seen for any medical reason within the past 2 years in one of 40 outpatient clinics at a large health care network in the Minneapolis/St. Paul metropolitan area between March 2008 and July 2011. While this sample is not strictly population based, it is also not strictly clinic based, as women could have been seen for any reason up to 2 years ago. A clinic-based sample would imply women actively seeking care, likely within a specific department. As such, and based on previous research demonstrating that the sample recruited using this methodology is generally reflective of the underlying population, 19 we consider this a community-based sampling strategy, which is closer to population based than clinic based.
The questionnaire asked about women's lifetime history of vulvar pain symptoms. A total of 30,676 women (43%) returned a completed survey. The University of Minnesota Institutional Review Board approved this study, and consent was implied based on questionnaire completion.
We excluded 2068 women (6.7%) missing data on the exposure, outcome, or confounders. In addition, five women were excluded because they had not yet started menstruating, and 191 were excluded because they reported CVP onset before age 13, which may have precluded them from experiencing pain due to tampon use or sexual intercourse. Finally, due to the survey design, 2039 women were excluded because they reported that they had experienced burning or pain that lasted 3 months or more, but that it had not occurred within the previous 6 months. Women who were not experiencing prevalent burning or pain did not answer follow-up questions required for the case definition (outlined below), so the chance of outcome misclassification among these women was high. The resulting sample from which we matched cases to noncases included 26,287 participants (Fig. 1).
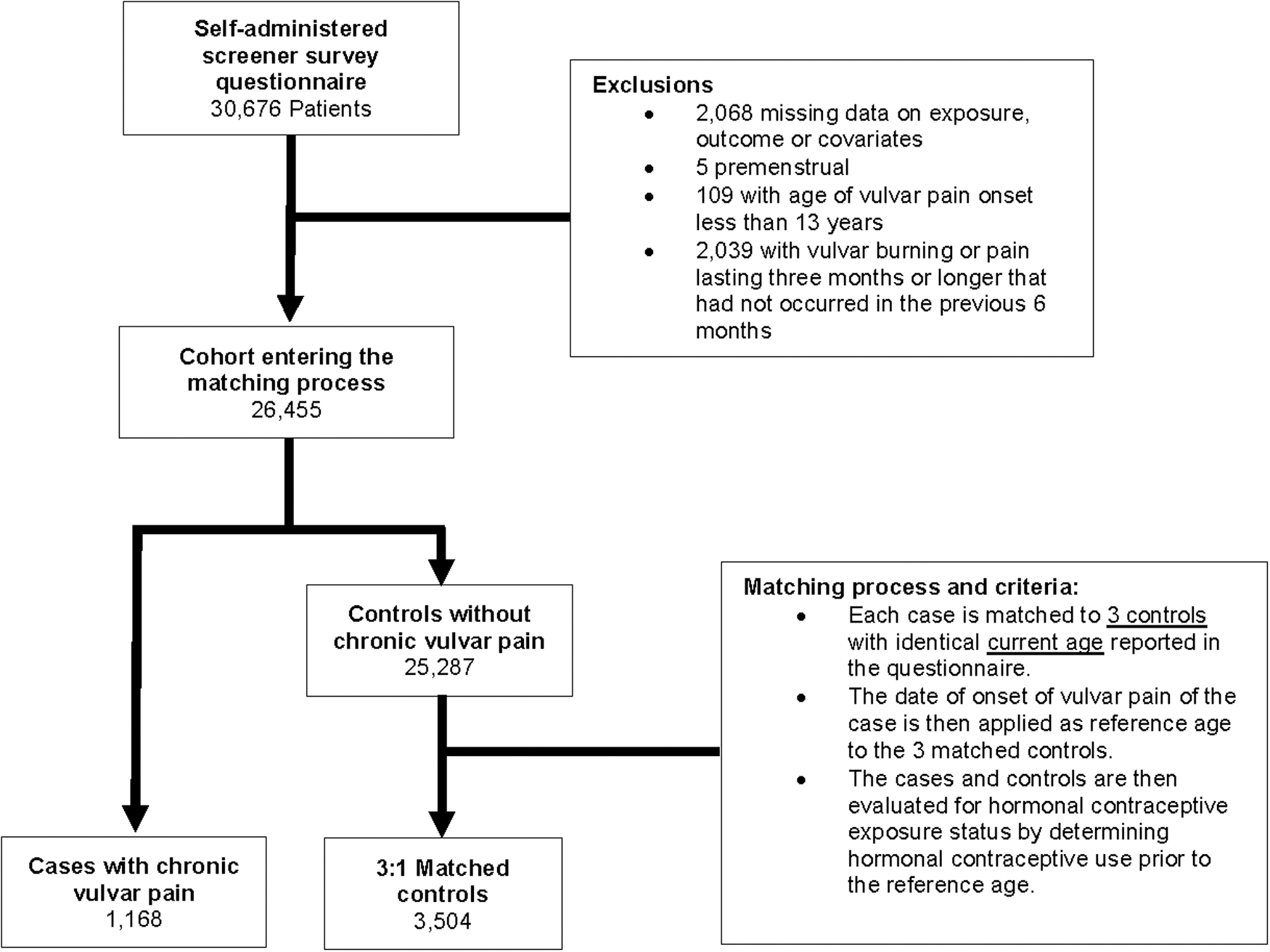
Flowchart outlining the patient selection and matching process.
Measures
Chronic vulvar pain
We assessed CVP through questions on vulvar burning, vulvar pain, and vulvodynia diagnosis. Women were classified as having CVP if they received a diagnosis of vulvar pain/vulvodynia and had experienced burning or pain on contact in their vulvar area that persisted for 3 months or longer. In the absence of a vulvodynia diagnosis, women were classified as having CVP if they reported experiencing burning or pain on contact in their vulvar area that persisted for 3 months or longer, that was either constant or had occurred intermittently at least 10 times, and had limited or prevented intercourse. This self-reported CVP classification has shown high sensitivity and specificity for clinically confirmed vulvodynia. 20,21 Age of CVP onset was determined from the earliest of reported age at first symptoms of CVP/vulvodynia diagnosis, first experience with burning in vulvar area that persisted for 3 months or longer, or first experience of excessive CVP on contact or touching.
To account for the fact that our case definition of CVP, combined with survey skip patterns, essentially limited the cases in our primary analysis to women who had prevalent CVP, we conducted a sensitivity analysis in which we added back in the 2039 women who reported a history of burning or pain lasting 3 months or more but not within the past 6 months, and repeated the entire analysis, including matching procedures. For this sensitivity analysis, women meeting our primary definition of CVP were again considered cases, as well as any woman who reported experiencing burning or pain on contact that lasted 3 months or more but had not occurred within the past 6 months.
Care-seeking behavior
Women who had CVP were classified as care seeking if they reported a diagnosis of vulvar pain/vulvodynia or if they answered yes to the question: “Did you ever see a health care practitioner about this discomfort?.” Care-seeking women would be the source population for recruitment into a clinic-based study of CVP or vulvodynia. Women classified as having CVP who did not report ever seeing a health care practitioner for CVP and did not report being diagnosed with CVP/vulvodynia were classified as not seeking care for CVP.
Prior hormonal contraceptive use
Prior HC use was defined as a positive response to: “Have you ever used hormonal contraceptives (e.g., birth control pill, Depo-Provera, NuvaRing)?” Women were considered exposed to HC if the reported age of first HC use was at the same age or before age at first onset of pain in CVP cases and the reference age among controls. If reported age of first HC use was after reported age of CVP onset (or reference age), women were not considered exposed to HC. Prior HC use was categorized according to years since first use. Years since HC initiation were calculated by subtracting the age of first HC use from the reference age.
Covariates
Covariates were prespecified using published literature 14,15 and plausible confounders. Covariates included race/ethnicity (white, Asian, Hispanic, Black/African American, or multiracial/other/missing), age at first menstrual period, and typical menstrual pain (no cramps or pain, mild cramps with medication seldom needed, moderate cramps with medication usually needed, and severe cramps with medication and bed rest required).
Matching process
We used a cumulative sampling strategy and matching to emulate a case–control study using our data. Each case was randomly matched, using exact matching without replacement, to three controls based on self-reported age at time of survey. Once matched, each control was assigned an index age equal to the age at first onset of CVP in the matched CVP case. We repeated the entire analysis using a different random number seed for the matching algorithm to test the results' sensitivity to the particular sample drawn.
Control women were considered exposed to HC if age at first use was younger than the index age assigned to them based on their matched case. As a sensitivity analysis, we repeated the analyses with a different matching strategy: matching the age of pain onset of cases to the current age of controls. The other elements of the matching (i.e., use of exact matching and a 1:3 ratio of cases to controls) were the same.
Statistical analysis
We used conditional logistic regression to estimate the odds of developing CVP in women who reported prior HC use compared with the odds among nonusers, overall and stratified by care-seeking status of cases, within the matched sample. In addition, prior HC use was categorized by years since first HC use. Using no HC use as the reference category, we modeled the odds ratio (OR) of developing CVP corresponding to each category of years since first HC use. The final model included adjustment for all prespecified confounders. All analyses were performed in SAS 9.4 (SAS Institute, Cary, NC).
Simulations
We conducted simulations to more robustly explore the potential effect of selection bias under various scenarios. We modeled two potential sources of selection bias, depicted with simulation inputs in Supplementary Figure S1a and b. We used data from our sample to inform the relationships depicted in the directed acyclic graphs. We simulated populations of 10,000,000 to reduce random error.
Scenario 1 was a truly null association between HC and CVP. We designated 67% of the simulated population as “general care seekers” based on a nationally representative U.S. survey reporting 33% of those aged 18–49 not seeing a doctor in the past year. 22 We simulated a baseline CVP prevalence of 5%, reflecting the prevalence in our sample. We randomly simulated HC use among 20% of nongeneral care seekers and 70% of general care seekers. We implemented CVP care seeking as highly dependent on general care seeking: among those with CVP, 90% general care seekers were assigned to be CVP care seekers, resulting in 62% of those with CVP being designated as care seekers for CVP, similar to our sample. Fifty percent of CVP care seekers were selected into the study, to reflect sampling from clinics. We simulated two types of control selection as follows: a random 10% of people without CVP and a random 10% of general care seekers without CVP. The former would approximate population-based control sampling, while the latter would approximate clinic-based control sampling.
Scenario 2 depicted a causal relationship between HC and a phenotype of severe CVP. We set the same prevalence of general care seeking as in Scenario 1. We assigned HC use as in the previous simulation. We divided CVP into two phenotypes with differing proportions of “severe” cases. Phenotype 1 was assigned randomly to 1% of the simulated population. Ten percent of people with Phenotype 1 were severe. Phenotype 2 was assigned to a random 1% of the population and 5% of those with HC use (indicating a causal risk difference of 0.05 for Phenotype 2 for HC users compared to nonusers). Seventy percent of people with Phenotype 2 were assigned to be severe.
The overall prevalence of CVP in the simulation was 5.3%, similar to our sample. CVP care seeking was assigned to 40% of general health care seekers with CVP of any severity, 10% of those with severe CVP regardless of care seeking, and 40% of those with general health care seeking and severe CVP. The final proportion of care-seeking women with CVP was 62%, reflective of our sample. Selection was assigned as above. All variables included in the simulations are binary.
We calculated ORs for the effect of HC on CVP among the entire simulated sample, then among only those who would be selected according to our two selection paradigms. We conducted sensitivity analyses with varied parameters.
The full SAS code is contained in a Supplementary Data.
Results
Participant data
Our final sample included 1168 women with CVP and 3549 women without CVP. Eighty percent of women with CVP and 65% of women without CVP reported HC use. Most of our sample identified as non-Hispanic white (89% of women with CVP and 86% of women without). A higher proportion of women with CVP reported moderate and severe menstrual cramps compared to women without CPV (Table 1). Table 2 displays details of HC use by CVP.
Sample Characteristics by Chronic Vulvar Pain Status in a Study of Women Recruited
Only among ever users.
CVP, chronic vulvar pain; SD, standard deviation.
Details of Hormonal Contraceptive Use Across Chronic Vulvar Pain Categories
Only among ever users.
Overall, the crude OR of developing CVP in HC users was 2.9 (95% confidence interval [CI]: 2.4–3.9) compared with nonusers (Table 3). Adjustment for prespecified confounders (race, age at menarche, and usual amount of menstrual pain) did not appreciably change this estimate. The estimate was smaller when cases were not care seeking (adjusted OR 2.3, 95% CI: 1.7–3.1) and larger when cases were those who sought care (adjusted OR 2.9, 95% CI: 2.2–3.7).
Crude and Adjusted Odds Ratios for Prior Hormonal Contraceptive Use and Chronic Vulvar Pain, Stratified by Care Seeking Status of Cases
Adjusted for race/ethnicity, age of menarche, typical menstrual pain, and difficulty with first tampon use.
Reference category is women who did not use HC (N = 1440).
The amount of years from onset of first hormonal contraceptive use until age of pain onset for cases and index date for controls.
CI, confidence interval; HC, hormonal contraception; OR, odds ratio.
When we considered HC use by interval between HC initiation and reference age, we found that associations were highest in women who first used HC <1 year before first onset of CVP or reference age in those without CVP. These associations became attenuated with longer time intervals between first use of HC and CVP onset in cases and reference age among controls. This attenuation pattern was similar in associations with cases who did and did not seek care. Overall, the ORs were about twice as high when HC initiation preceded pain onset within 1 year compared with these events being more than 10 years apart. Effect estimates were stronger in analyses of care-seeking cases than noncare-seeking cases.
Table 4 has the results of the sensitivity analysis in which women with a history of burning or pain that had not occurred in the past 6 months were considered cases. Most estimates were slightly attenuated, particularly those among women with <1 year between HC use and onset of vulvar pain. The association between prior HC use and CVP persisted among this sample and was stronger when cases were restricted to those who sought care.
Crude and Adjusted Odds Ratios for Prior Hormonal Contraceptive Use and Chronic Vulvar Pain, Among a Sample in Which Participants with Nonprevalent Burning or Pain Were Included as Cases
Adjusted for race/ethnicity, age of menarche, typical menstrual pain, and difficulty with first tampon use.
Reference category is women who did not use HC (N = 2816).
The amount of years from onset of first hormonal contraceptive use until age of pain onset for cases and index date for control.
The sensitivity analysis in which we changed the matching schema did not change the overall results except that the ORs for those with <1 year between first hormonal contraceptive use and age of CVP onset for cases or index age for controls were larger compared to the main analysis (Supplementary Table S1).
Simulations
In simulations where controls were sampled from clinics, neither scenario 1 (null association) nor scenario 2 (severe disease phenotype) consistently produced bias in the hypothesized direction (larger effect estimate among the selected compared with the effect in the full population) (Table 5).
Results of Simulations of Collider Stratification Bias
Scenario 1 models bias caused by conditioning on selection into the study, which is a collider of general health care seeking and care seeking for vulvodynia.
Scenario 2 models bias caused by conditioning on selection into the study, which is a collider of general health care seeking, care seeking for vulvodynia, and severe vulvodynia. In this scenario, there are two phenotypes of vulvodynia, one of which (Phenotype2) is caused, in part, by exposure to HC. This phenotype is more severe, which leads to an increase in vulvodynia-related care seeking.
Phenotype 2 is caused, in part, by prior exposure to HC and has a higher proportion of severe disease than Phenotype 1.
In simulations where controls were sampled from the general population, the bias consistently operated in the hypothesized direction, amplifying the effect estimate. This was consistent across both scenarios and all sensitivity analyses. The magnitude of the bias was similar across both scenarios.
Discussion
In a large community-based sample of women, we observed an association between prior HC use and CVP. This association persisted after adjusting for race, age of menarche, and average menstrual pain.
We found a stronger association when we restricted cases to women who reported seeking care for CVP than when we restricted cases to noncare seekers, although an association between HC use and CVP was present in both approaches. We did not have information about the care-seeking status of controls in our data, so our analyses compared cases, stratified by care-seeking status, to a consistent control population that approximated a population-based control sample. When cases were restricted to only care seekers, the effect estimates were magnified. Our simulations also found that clinic-based case recruitment coupled with population-based control recruitment consistently magnified effect estimates. In fact, under Scenario 1, a true null association, this bias resulted in a spuriously positive association between HC and CVP.
Therefore, our findings, together with our simulations, suggest that observed associations evaluating the relationship between HC and CVP may be influenced by sampling strategies for cases and controls. Clinic-based recruitment of cases and population-based recruitment of controls seem to result in the most magnified effect estimates. Future studies evaluating the etiology of CVP/vulvodynia considering the use of a case–control design should carefully consider these potential biases when considering sampling schemas.
In addition to implications for study design, our findings also have clinical implications. Our findings are similar to other case–control studies that have reported a positive association between HC use and vulvodynia. 11 –14 We found that the effect estimates were slightly stronger when the interval between the initiation of HC and the onset of CVP was shorter, although we lacked information on whether women were continuously using HC which precludes comparison of our results with results from other studies reporting higher odds of vulvodynia with longer use of HC. 11,12 In addition, there was a strong possibility for exposure misclassification within the <1 year difference category because we did not know whether pain preceded HC use when they occurred at the same age. Nonetheless, our results may add to existing evidence that some women develop CVP following HC use. 11 –13,23
Women report barriers to seeking care from clinicians for chronic sexual pain, including fear of their concerns being dismissed. 24 Thus, providers should consider querying patients about any new or worsening experiences of vulvar pain after initiation of HC. Furthermore, recommending that women report the development of vulvar pain when initiating HC may be a productive way to signal support to patients with regards to pain. It is important to note that although we explored one possible source of selection bias in case–control studies of HC and CVP, we cannot rule out the possibility of selection bias due to other factors in our and other case–control studies addressing this issue.
Our study was limited by use of data from a questionnaire with limited covariates, including no data on the reason for HC use, (including whether or not participants were partnered and/or currently sexually active), nor adherence, dosing, or specific name of contraception agents. While we classified hormonal contraceptive users in terms of years since first use, we do not know details about their usage pattern during that time, so this measure is not necessarily an accurate approximation of duration of use.
Furthermore, in our question asking about hormonal contraceptive use, we did not specify an example of a long-acting reversible contraceptive (LARC; i.e., an intrauterine device or implant), nor the contraceptive patch. Thus, it is possible that some women who had exposure to HC via these methods mischaracterized themselves as unexposed. The prevalence of the use of LARCs in the United States was relatively low (∼8.5%) at the start of our sample collection in 2008, but likely increased over the study period. 25 However, having asked about lifetime exposure to HC may have mitigated any possible misclassification of these women, if they used another method before or after using a LARC.
We do not know the potential implications of the possible misclassification of women who used LARCs, as there is little research that evaluates the association of different types of HC and CVP. Future research into the association between HC and CVP would benefit from evaluating different types of HC separately.
Finally, it remains possible that women who chose to respond may not accurately reflect all women asked to participate in the questionnaire. However, we have previously reported that respondents and nonrespondents were comparable by age. 3 In addition, it is not likely that women who chose or chose not to respond were more or less likely to be hormonal contraceptive users. Therefore, nonresponse would be expected to bias the true associations toward the null. In addition, if women with vulvar pain chose more so than others not to respond, then our estimates of associations will also be expected to be an attenuation of the true estimates.
A further limitation is that we relied on self-reported symptoms to categorize CVP. In previous research, these questions had strong sensitivity and specificity in relation to women with clinically confirmed vulvodynia, 20,21 but outcome misclassification is still possible, and our sample likely includes women with CVP that would not be diagnosed as vulvodynia upon clinical examination. Our case definition combined with survey skip questions meant that our cases in our primary analyses were restricted to prevalent (within 6 months) cases. CVP symptoms may resolve over time, 26 so it is possible that we are missing women with a history of CVP. To estimate the impact of this, we conducted a sensitivity analysis in which we added all women with nonprevalent burning or pain lasting 3 months or more as cases. We found slightly attenuated estimates, but the trends observed in the overall analyses held.
Finally, we do not have information on sexual activity, which could be an important confounder if it is associated both with obtaining HC and women discovering that they have vulvar pain. We did ask women with CVP whether they had experienced intercourse, and overall the vast majority of women reported having had intercourse (95%). However, we do not know the percentage of controls who had never had intercourse, and it is possible that having never had intercourse would reduce the chances of women both requiring HC and reporting vulvar pain.
Importantly, our sample is not truly a population-based sample, but rather was recruited from the administrative database of a large health care network. An assessment of this sampling method suggests that it generally produces a sample that is reflective of the underlying population. 19 The fact that this sample was recruited from a health care network likely means that our control group has a higher proportion of care-seeking women than would be found in a true population-based sample. However, given that these women could have been seen as long as 2 years ago for any reason, we believe that our sample is likely closer to a population-based sample than a clinic-based sample, where participants would have to be actively engaged in care. Future studies could validate our findings using a population-based sample not recruited from a health care network.
Conclusions
Our study is an important call for careful sampling selection in the context of exposures that would reasonably be related to care-seeking behaviors and suggests that in situations where cases are exclusively recruited from health care settings, but controls are sampled from the general population; the association between HC and CVP or vulvodynia may be spuriously strengthened. This is an important consideration for etiologic research into this condition, especially in the context of research involving the potential role of HC. Because exposure to HC is highly prevalent among reproductive-aged women, 10 effective study design in research addressing its etiological role in CVP and vulvodynia could influence the health of a vast number of women.
In our overall analyses, which would best approximate a population-based sample, we found increased odds of CVP among those with a history of HC use. Health care providers prescribing HC may wish to actively follow-up with new patients to screen for the development of vulvar pain, as women may not seek care even when experiencing it.
Footnotes
Authors' Contributions
B.L.H. planned and carried out the data collection. J.C.B. and J.J.K. performed the data analyses with oversight from B.L.H. J.C.B. conducted the simulations with oversight from M.P.F. J.C.B. and J.J.K. wrote the article, all authors revised critically. All authors read and approved the final article.
Author Disclosure Statement
No competing financial or personal interests exist.
Funding Information
This work was partially supported by the National Institute of Child Health and Human Development at the National Institutes of Health (grant NIH-NICHD-R01 HD058608).
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.