
Abstract
Background:
In the last decade, there has been an unprecedented amount of advocacy and attention surrounding the issue of breast density (BD) in relation to mammography screening. It is largely unknown what impact notifying women of their BD has had on clinical practice for PCPs. This systematic review aimed to synthesize evidence from existing studies to understand the impact of BD notification on primary care practitioners' (PCPs) knowledge, attitudes, and practice implications.
Methods:
Empirical studies were identified through relevant database searches (database inception to May 2020). Two authors evaluated the eligibility of studies, extracted and crosschecked data, and assessed the risk of bias. Results were synthesized in a narrative form.
Results:
Six studies of the 232 titles identified and screened were included. All studies were undertaken in the United States, with five conducted postlegislation in their respective states, and one study conducted in states that were both prelegislation and postlegislation. Five studies were quantitative, including four cross-sectional surveys, and one study was qualitative. Findings consistently demonstrated PCPs' overall lack of knowledge about BD, low level of comfort in discussing and managing patients in relation to dense breasts, and limited consensus on the most appropriate approach for managing women with dense breasts, particularly in relation to supplemental screening.
Conclusions:
This review highlights important gaps in PCPs' understanding of BD and confidence in having discussions with women about the implications of dense breasts. It identifies the need for high-quality research and the development of evidence-based guidelines to better support PCPs.
Introduction
Breast density (BD) refers to the relative amount of fibrous and glandular tissue in a woman's breasts compared with the amount of fatty tissue, as seen on a mammogram. There are four categories of breast density as classified by the Breast Imaging Reporting and Data System (BI-RADS) Atlas 1 : almost entirely fatty, scattered areas of fibroglandular tissue, heterogeneously dense, and extremely dense. The latter two categories (classified as having dense breasts) are estimated to be prevalent in 40%–50% of women in the breast screening population in the United States. 2 Dense breast tissue independently increases the risk of breast cancer 3 and, through its masking effect, lowers the sensitivity of mammography, which can increase the chance of a cancer going undetected. 4 The latter may lead to a higher frequency of interval cancers, breast cancers that are diagnosed after a clear mammogram and before a woman's next mammogram. 5
In the last decade, there has been an unprecedented amount of advocacy and attention in the United States surrounding the issue of breast density in relation to mammography screening. 6 Before this time, breast density was less frequently discussed in relation to the risk of developing and being diagnosed with breast cancer. However, as a result of a largely consumer-driven movement highlighting the importance of informing women about whether they have dense breasts, with the overall intention of improving health care decision-making, breast density legislation has now passed in majority of the United States. Since the enactment of such legislation, 7 women are now routinely notified of their breast density after each mammogram.
Primary care practitioners (PCPs) are at the forefront of health care decision-making with patients. Their understanding of and how they communicate about a wide range of health issues is of upmost importance in informing patients' decisions. Breast density is now one of these many health issues. With numerous states in the United States now recommending that women receive their BD notification follow-up with primary care, PCPs along with obstetrician-gynecologists and radiologists may be faced with BD discussions with patients without adequate support and evidence to guide them in making BD-related recommendations. 8 While the exact role of PCPs differs across health systems internationally, in the United States PCPs, obstetrician-gynecologists, and radiologists play a complementary role in the notification, discussion, and recommendations around BD and the issue of supplemental screening. Radiologists are required by most states to inform women of their breast density and encourage conversation with their PCP or usual physician.
The issue of breast cancer risk and supplemental screening, in particular, is not straightforward. First, BD is a risk factor that is not readily modifiable, which may make it challenging for women to understand what this means for them, and for PCPs to have discussions about risk-based strategies. Furthermore, while supplemental screening with imaging modalities such as ultrasound and magnetic resonance imaging (MRI) has been shown to enhance detection of cancer in dense breasts, 9 the evidence is lacking to support long-term outcomes in terms of the rate of advance breast cancer diagnosis and mortality. 9 –11 The potential benefit from increased detection of cancers through supplemental screening in women with dense breasts may not outweigh the associated downsides, including false positives, overdiagnosis, and overtreatment of breast cancer.
It is largely unknown what impact legislation for BD notification has had on clinical practice for PCPs, in particular, in relation to their knowledge about BD, how they feel about the legislation and its implications for discussions with patients, and importantly, recommendations for supplemental screening. This understanding is not only of central relevance for the care of women in the United States moving forward, but is gaining importance for other countries currently considering implementing similar BD legislation or widespread notification. This systematic review aims to synthesize evidence from existing studies to understand the impact of breast density notification on PCPs' knowledge, attitudes, and practice implications.
Methods
Review registration
The systematic review's protocol was prospectively registered with PROSPERO (an international prospective register of systematic reviews), registration number: CRD42020189628
Search strategy
In consultation with a literature search specialist, a comprehensive list of search terms was developed and tested for the return of potentially appropriate results (Supplementary Table S1). The keywords, phrases, and subjects-headings included in the database search strategy were informed by a similar systematic review on the topic of breast density notification conducted by study authors 12 and were further refined to specifically capture the population and outcomes of interest. The database search of Cinhal, Embase, Medline, Pre-Medline, PyscINFO, and PubMed was conducted from database inception to May 2020. A general search of the Cochrane Reviews database and extensive gray literature search using Google and Proquest to look for conference presentations and proceedings, dissertations, and media, as well as a search in specific international gray literature databases for government publications and reports were also conducted. After removing any duplicate, the returned search results were screened by title and abstract independently by two researchers (B.N. and T.C.) for eligible articles. Study eligibility criteria (Box 1) were used by the authors to guide the selection of appropriate studies. Decisions regarding inclusion and exclusion of studies were then made independently by the same two researchers (B.N. and T.C.), and any disagreement was carefully discussed to reach consensus.
Systematic Review Eligibility Criteria
BD, breast density; PCPs, primary care practitioners.
Criteria of inclusion and exclusion
Studies were included in the review if they empirically assessed the impact of breast density notification on PCPs' knowledge, perceptions, practice, or recommendations. No restrictions were placed on country, year of publication, or written language. Studies were excluded if they were protocols, reviews, editorials, or commentaries. Studies were also excluded if they exclusively assessed the impact of breast density information or notification only on radiologists, as the practice implications were deemed to be vastly different to those of PCPs.
Quality assessment and data extraction
All studies that met the inclusion criteria were appraised for study quality (risk of bias) by two authors (B.N. and T.C.) independently using the Joanna Briggs Institute (JBI) critical appraisal tools. 13 Based on the scoring of the individual items used in each appropriate checklist, three categories of study quality (low, moderate, and high risk of bias) were identified according to each study's methodological characteristics. In high-quality studies (low risk of bias), the majority of criteria were fulfilled and done well, while in low-quality studies (high risk of bias), the majority of criteria were not addressed, unclear, or addressed poorly.
Data from the final studies included in the review were extracted by one author (B.N.) into a standardized template in Excel and checked by a second author (T.C.). Results from the studies were synthesized in a narrative form, as the heterogeneity of the studies did not support the pooling of results. 14
Results
The initial search yielded 400 articles. After removal of duplicates (n = 232) and screening by title and abstract, 10 articles from the search underwent full text review. Six articles were then identified and agreed upon for final inclusion (Fig. 1).
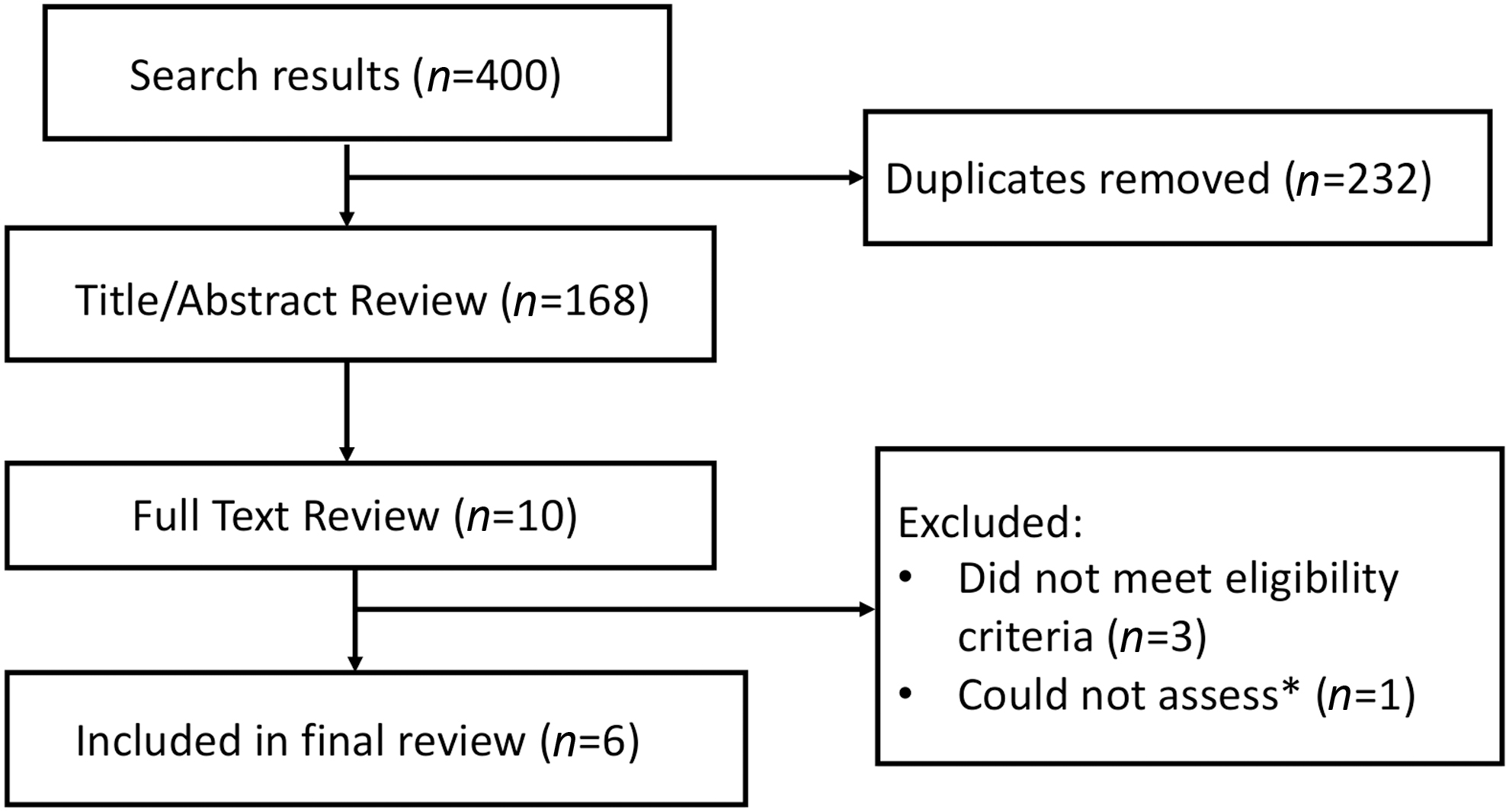
Flow diagram of included studies. *For one study where only the conference abstract was published, the study authors were contacted for additional information as the level of detail was not appropriate to systematically assess. As the authors did not respond, it was excluded from the final analysis.
Characteristics of six included studies are summarized in Table 1. There were five quantitative studies, including four cross-sectional surveys (sample size [N] range = 77–362), 15 –18 and one quasi-experimental study (N = 63) 19 assessing a workshop aimed at improving PCP's knowledge of BD, and increasing confidence in counseling patients about supplemental screening. The final included study was a qualitative interview study. 20 There were no randomized controlled trials. All studies were undertaken in the United States. 15 –20 Three of the six studies were conducted in Massachusetts, 16,19,20 and there were no studies that included a national sample. Five of the studies 15 –17,19,20 were conducted in their respective states postlegislation, and one study 18 was conducted in states that were both prelegislation and postlegislation. The main outcomes of interest across the studies were knowledge, attitudes, and practice implications for PCPs.
Characteristics of Included Studies
As reported in the article
As decided on by study authors based on the explicit checklist items in The Joanna Briggs Institute Critical Appraisal Tools (
BD, breast density; OBG, obstetrics and gynecology; PCPs, primary care practitioners.
Two studies 16,20 were of higher quality with a low risk of bias; the other four studies 15,17 –19 had moderate to high risk of bias, as the overall quality of reporting was deemed to be low. The high-quality studies included one of the quantitative surveys 16 and the included qualitative study 16 (Supplementary Table S2).
Results from the studies are narratively synthesized below by PCPs' knowledge of BD notification and BD generally, PCPs' attitudes toward BD notification, and practice implications in relation to BD notification. Table 2 describes these findings in more detail by individual study.
Key Findings Summarized by Knowledge, Attitudes, and Practice Implications
MRI, magnetic resonance imaging.
PCPs' knowledge of BD and BD notification laws
General awareness of BD notification laws and knowledge surrounding the topic of BD was highly variable across the studies. Two studies 15,17 reported just over half of the sample were aware of the laws and other three studies 16,18,20 indicated that the majority of the PCPs were aware of the laws. However, in two of the three studies with higher awareness of the BD notification laws, knowledge of breast cancer risk was also measured and was notably lower than awareness. 15,18
PCPs' attitudes toward BD and BD notification laws
There were a wide range of measures used to assess PCPs' attitudes toward BD notification law and the concept of BD generally. In two studies, 16,20 it was shown that PCPs had mixed feelings about BD notification laws. In the survey conducted in Massachusetts the year following BD notification enactment 16 it was found that only 38% of PCPs favored the legislation. The qualitative interview study 20 conducted in Massachusetts around the same time period found that there were mixed attitudes around the utility of BD laws for patients and PCPs. PCPs in this study had relatively positive attitudes about how legislation might affect patient engagement; however, PCPs also noted the lack of evidence informing next steps for screening patients with dense breasts and identified stress and anxiety as a possible negative consequence of informing patients.
In terms of level of comfort about discussing and answering questions about BD, again the findings were mixed. In two survey studies conducted at similar time points following enactments of BD notification, one study found only 6% of PCPs in California described themselves as being completely comfortable, 17 while the other study conducted in Massachusetts found that over 80% of PCPs indicated “some level of comfort” in having these discussions and in answering questions in relation to density. 15 In Maimone et al.'s survey, 18 conducted across three states (one prelegislation and two postlegislation), PCPs were also split in their level of “comfort” in answering questions and providing management advice for patients. In all three studies, PCPs highlighted the need for further education and training about BD and how to manage patients, with Brown et al.'s 15 finding that PCPs were more likely to report the need for more education about BD, relative to specialists (p < 0.0001).
Two studies 16,19 assessed whether PCPs felt a responsibility to counsel women about BD. In the survey study, 16 attitudes were split with less than half PCPs feeling it was their responsibility to counsel patients and around a quarter being neutral or unsure, believing it was the responsibility of radiologists or breast health providers. In the quasi-experimental study, 19 in the postintervention survey compared to the baseline survey, more PCPs and residents in the intervention group agreed or strongly agreed that it was their responsibility to counsel women about BD; however, this change was not significant.
Practice implications for PCPs in relation to BD notification
A number of different practice implications for PCPs in relation to BD notification were highlighted across studies. In the qualitative study, 20 it was found that PCPs felt that the legislation failed to contextualize BD into a broader conversation about risk factors for breast cancer, and PCPs were particularly interested in discussion about modifiable risk factors such as exercise and alcohol intake. PCPs in this study felt that radiologists should be the first point of information about BD followed by additional questions and contextualization of the results from PCPs. In the survey study by Khong et al., 17 about a quarter of PCPs discussed performing breast cancer risk assessments themselves, while the remainder referred women to a breast health clinic when they thought a risk assessment would be beneficial.
In two of the survey studies, 15,18 practice implications for PCPs mainly focused on the issue of discussing and recommending supplemental screening. In the study by Maimone et al., 18 there was large variability in whether PCPs indicated they offered supplemental screening to every patient with dense breasts and the choice of a particular supplemental screening modality also varied greatly, with most respondents initially choosing digital breast tomosynthesis. Cost to the individual patient and breast cancer risk model results were the most common factors that most heavily influenced PCPs' decisions to suggest supplemental imaging. In the study by Brown et al., 15 there was a mix of responses for how they would proceed with management with 49% respondents feeling it necessary to order supplemental ultrasound, 7% supplemental breast MRI, and the remaining 42% continuing routine screening or gave no clear recommendations. For the same women with heterogeneously dense breasts, the numbers followed a similar trend (59%, 3%, and 13%, respectively).
It was flagged in a number of studies 16 –18,20 that PCPs would value additional support and resources to help alleviate confusion and improve the process of counseling patients about BD and supplemental imaging, including additional data and literature for PCPs, and patient information videos or pamphlets.
Discussion
A small literature base exists from which to assess the impact of breast density information and notification on PCPs in clinical practice. Studies evaluating this issue are mostly low to moderate quality, with the majority being surveys with modest response rates conducted in the United States with convenience samples. All but one of the studies were conducted in their respective states in the postlegislation period, with the other study not describing differences between states in the results, despite being conducted across three states with varying prelegislation and postlegislation periods. Despite the small number of studies, findings from this systematic review highlight PCPs' overall lack of knowledge about BD. Although PCPs in states where BD legislation had been enacted the longest seemed to indicate greater awareness of BD and BD notification laws, there was still limited knowledge of breast cancer risk. Importantly, finding across the studies also highlighted the low level of comfort in discussing and managing patients in relation to dense breasts, and limited consensus on the most appropriate approach for managing women with dense breasts. This review points to the need for high-quality research to assess the impact of BD notification on PCPs and how best to discuss the implications of having dense breasts with women.
Uncertainty and variability on whether PCPs should discuss and recommend risk-based strategies or only offer supplemental screening was shown in this review. Since discussion about widespread BD legislation began over a decade ago in the United States, the core of the BD notification controversy has largely been focused on whether or not to offer supplemental screening, and if so, what type, to who, and what frequency. 21 Given the limited consensus in this area 11 and lack of guidelines, outside of obstetrician-gynecologists and radiologists, the ordering of supplemental screening modalities for women with dense breasts may be left up to the discretion of the PCP in individual consultations with their patients. Findings from the included studies highlight the need for the current uncertainty and variability around recommendations for supplemental screening to be factored into guidelines for PCPs. In settings where BD is not routinely notified, any contemplated change to potentially systematically notify women about their BD should engage PCPs, as well as obstetrician-gynecologists and radiologists, as key stakeholders in the decision about such notification. In two of the included studies, 16,20 PCPs were split in support for BD notification legislation, noting they were concerned about the current lack of evidence to inform decision-making for next steps and about providing BD information to patients without a clear course of action. This further highlights the need to involve PCPs in the initial decision-making process as well as the co-designing of future research in this area and management strategies.
Additional training opportunities for PCPs may also help to ensure they are provided with education and support for understanding BD, having discussions and managing women with dense breasts. Although countries outside of the United States do not currently have BD notification through population-based screening programs, many private screening services in these countries are notifying women about their BD. Furthermore, given the recent developments in the United States, there is now growing pressure from key breast cancer advocacy groups to inform women of their BD on a more wide-scale level. 22 Universally, PCPs will need to become more aware and receive training surrounding the issue of BD, the inconsistencies in current evidence, and the implications this has for women, to be able to have confidence in discussions around these topics. For now, PCPs' discussions and future research could be best directed toward discussion of women's individualized risk factors and the possible benefits and trade-off for women in regard to options for supplemental screening.
This review has important strengths and limitations. First and foremost, this is the first systematic review to synthesize the impact that BD notification and legislation has had specifically on PCPs. This timely contribution to the literature highlights the need for further research and support for PCPs as they have been shown to be a crucial source of information and support for women in this area. 20,23 The review has been reported in accordance with the criteria in the PRISMA statement for systematic reviews (Supplementary Table S3). Due to the variability of the measures used and reported outcomes in the included studies, authors were unable to conduct a meta-analysis and pool the effects of the data, and therefore the results are synthesized narratively. 14 Furthermore, the small number of studies assessed were at various time points in different locations across the United States, so all have different notification processes and information about BD that are provided to both women and PCPs. Finally, as all studies were conducted in the United States where BD is legislated, the findings may not be generalizable to other health care systems. Given the lack of widespread notification in other countries, it is likely that PCPs may have more limited knowledge and feel less comfortable with discussing BD and managing women with dense breasts.
Conclusions
Notwithstanding the limited literature base identified in this review, these studies highlight that PCPs are impacted by BD notification and they feel uncertain about their knowledge and how best to manage their patients. These findings highlight important gaps in current understanding, and identify the need to develop, in consultation with PCPs and other health care professional involved in BD discussions and management, evidence-based guidelines. Such guidelines and inclusion of this information in training programs will enable PCPs to be better informed and supported. How PCPs discuss and manage women in relation to the issue of BD moving forward will significantly impact the benefit-to-harm trade-off of notifying women. 22 This understanding and how to improve it are not only crucial to support the current care of women in countries that have already implemented BD notification but also future care of women in countries that may be considering implementing widespread BD notification.
Footnotes
Author Contribution Statement
B.N., K.M., and N.H. conceived the study. B.N. and T.C. screened title and abstracts. B.N. and T.C. completed the full text read and data extraction. B.N. completed the data synthesis with support from T.C., and N.H., B.N., and T.C. conducted the risk of bias assessment. B.N. wrote the article with input from T.C., M.B., R.F., K.M., and N.H.
Authors Disclosure Statement
No competing financial interests exist.
Funding Information
K.M. is supported by an NHMRC Principal Research Fellowship (1121110). NH is supported by an NHMRC Research Leader Fellowship (1194410). The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.