
Abstract
Cervical cancer can be prevented through routine screening and follow-up of abnormal results. Several guidelines have been published in the last 4 years from various medical societies and organizations. These guidelines aim to personalize screening and management, reducing unnecessary testing in low-risk patients and managing high-risk patients with more intensive follow-up. However, the resulting complexity can lead to confusion among providers. The CDC, NCI, and obstetrician-gynecologists involved in guideline development summarized current screening and management guidelines. For screening, guidelines for average-risk and high-risk populations are summarized and presented. For management, differences between the 2012 and 2019 consensus guidelines for managing abnormal cervical cancer screening tests and cancer precursors are summarized. Current screening guidelines for average-risk individuals have minor differences, but are evolving toward an HPV-based strategy. For management, HPV testing is preferred to cytology because it is a more sensitive test for cancer precursor detection and also allows for precise risk stratification. Current risk-based screening and management strategies can improve care by reducing unnecessary tests and procedures in low-risk patients and focusing resources on high-risk patients. Knowledge of screening and management guidelines is important to improve adherence and avoid both over- and under-use of screening and colposcopy.
Introduction
The incidence of cervical cancer in the United States decreased profoundly following the implementation of routine screening with Papanicolaou (Pap) testing (also called cervical cytology). 1 However, cervical cancer incidence has plateaued in the past decade; nearly 13,000 cancer cases are diagnosed every year, and one third of patients will die from their disease. 2 Nearly all cervical cancers are caused by persistent infection with high-risk human papillomavirus (HPV). 3 In the past several decades, increased understanding of the natural history of HPV infections has been applied to increase the efficacy and efficiency of cervical cancer prevention. 4,5
Most HPV infections are controlled by the cellular immune system quickly, but a minority persists overtly for more than 2 years after infection of the cervical epithelium. When HPV infections persist for several years, the risk of developing a cervical precancer increases. 6 A minority of cervical precancers will invade if left untreated after years or decades. This extended period between HPV infection and cervical cancer is the key to successful screening programs, allowing for cancer precursors to be treated in a timely manner to prevent the development of invasive cervical cancer.
HPV infections that may develop into cancer can often be detected earlier by screening using testing other than Pap testing. 7 Because HPV testing is very sensitive, patients are less likely to develop cervical cancer or precancer within 5 years after a negative HPV test than a negative Pap test (i.e., a Pap test result of negative for intraepithelial lesion or malignancy [NILM]). 8 HPV-negative patients should be screened at 5-year intervals to avoid detecting new HPV infections that are likely to regress spontaneously. 9,10 HPV testing also detects more glandular cervical lesions than Pap testing. 11 HPV testing may improve screening for adenocarcinoma of the cervix, a form of cervical precancer that is not sufficiently detected by Pap testing alone. 8,11 However, HPV-positive patients require additional testing or surveillance. 5 Improved understanding of HPV epidemiology and the natural history of infection has led to advances in screening and management, including the incorporation of HPV testing into recommendations and guidelines. 5,9,10
Screening
Participation in screening is a critical component of cancer prevention and control, as more than half of cervical cancers are diagnosed in patients who have not participated in regular screening. 12,13 Screening recommendations and guidelines have evolved from recommending annual cervical cytology (Papanicolaou or Pap tests) for all patients, to now including testing for oncogenic HPV types (HPV testing) and recommending screening less frequently. Screening recommendations and guidelines have been published by the American College of Obstetricians and Gynecologists (ACOG) in 2016, 14 U.S. Preventive Services Task Force (USPSTF) in 2018, 9 and American Cancer Society (ACS) in 2020. 10 The USPSTF recommendations are widely followed as they are linked to quality of care measures as well as reimbursement from Medicare and Medicaid. 15,16 All recommendations and guidelines recommend regular screening between the ages of 25 and 65 years with options, including HPV testing alone, Pap testing alone, and HPV and Pap testing together (cotesting). Screening also is recommended for older women who lack documentation of an adequate history of negative screening tests. 9 HPV testing alone and cotesting are recommended at 5-year intervals beginning at either age 25 or 30 years. Note that HPV tests must be used according to their regulatory approval, and not all are approved for primary testing. 5 Pap testing alone is recommended at 3-year intervals beginning at age 21 years. Initiation of screening with Pap testing alone between the ages of 21–24 is included in the USPSTF recommendations and ACOG guidelines, while the ACS guidelines recommend starting screening with HPV testing at age 25. The ACS raised the age to initiate screening based on new data demonstrating that HPV vaccination in adolescence correlates with a decreased incidence of invasive cancers in women younger than age 25. 17 Specific recommendations are detailed in Table 1.
Current Cervical Cancer Screening and Surveillance Recommendations: US Preventive Services Task Force (USPSTF, 2018), American College of Obstetricians and Gynecologists (ACOG, 2016), American Cancer Society (ACS, 2020) and ASCCP (2019)
Considered an alternative screening strategy by ACOG.
Based on recommendation by the Panel on Opportunistic Infections.
ACOG, American College of Obstetricians and Gynecologists; ACS, American Cancer Society; CIN, cervical intraepithelial neoplasia; HPV, high-risk human papillomavirus; HSIL, high-grade squamous intraepithelial lesion (either by cytology or by histology; includes a persistent cytologic diagnosis of atypical squamous cells cannot rule out HSIL); USPSTF, US Preventive Services Task Force.
Importantly, routine average-risk screening recommendations and guidelines apply only to patients who fulfill the following criteria: asymptomatic, not immune-compromised, not exposed to diethylstilbestrol (DES) in utero, not currently under surveillance for abnormal screening test results, and no history of high-grade abnormal results or treatment for cancer or precancer (Fig. 1). Note that recommendations and guidelines have increased the recommended length of follow-up after treatment for high-grade precancer based on newer data. 18,19 Guidelines now indicate that screening should continue for at least 25 years, and is acceptable as long as life expectancy is not limited. 5,20 Pap testing is an important part of the workup of abnormal uterine bleeding, as well as continued monitoring of DES-exposed patients, who are at risk for clear-cell adenocarcinomas of the vagina and cervix that are not related to HPV. 14,21

Details questions that health care providers can ask to determine whether a patient qualifies for routine screening.
Patients with HIV and severe immunocompromising conditions (e.g., after solid organ transplantation) are at increased risk for both persistent HPV infections and cervical cancer, thus screening guidelines are different. 22,23 Screening initiation is recommended within 1 year of onset of sexual activity and no later than age 21 years for those with HIV diagnosed before age 21 years, and should occur at the time of HIV diagnosis for those aged 21–29 years. Screening of HIV-positive patients aged <30 years should consist of annual Pap testing until three consecutive normal test results have been obtained, followed by continued testing at 3-year intervals. For patients aged ≥30 years, testing may consist of annual Pap testing alone with extension to testing every 3 years after three consecutive normal test results, or cotesting at 3-year intervals. HPV testing alone is currently not recommended. Lifelong screening is recommended in patients with HIV. 22,23
In the near future, cervical cancer screening in the United States may involve self-sampling for HPV. Currently, self-sampling is part of screening programs in several countries to extend screening to patients who do not participate in provider-based screening. 24 A meta-analysis of 56 studies and an randomized clinical trial (RCT) showed that HPV assays using polymerase chain reaction technology were equally sensitive for detection of precancer when comparing self-collected samples with clinician-collected samples. 25 Self-sampling has the potential to increase access to screening, both by reducing the need for clinic visits, and decreasing barriers to cervical cancer screening during clinic visits. Self-sampling can be performed at home and mailed to the laboratory, which can be helpful to reach populations with limited access to medical facilities. Self-sampling can also be collected by the patient during a clinic visit, obviating the need for a speculum examination, and, in some areas, a chaperone and/or separate consent form, all of which are barriers to cervical cancer screening among patients who are otherwise able to access medical care. 26,27 Currently, self-sampling products have not been implemented widely. Regulatory approval and guidelines for appropriate use by health care providers and robust system for follow-up of abnormal results, especially for those screened via mail, can help with widespread implementation.
Surveillance following abnormal test results
For patients with recent abnormal screening test results, repeat testing is recommended at shorter intervals than those used for screening. 5 The 2019 ASCCP Risk-Based Management Consensus Guidelines define a new paradigm for managing cervical cancer screening test abnormalities. 5 Previous management guidelines had begun to introduce the concept of incorporating past screening history into management. 28,29 The 2019 guidelines for the first time separated the subjective clinical decisions about risk-based management thresholds from the objective risk estimation based on test results, screening history, and age (Fig. 2). 5 In particular, several new concepts were introduced, which allow for a more personalized approach to each patient's care. Risk stratification now accounts for whether a patient has had abnormal results, which increase risk, or has documented negative HPV screening test results, which decrease risk. Accurate risk estimation requires testing with an U.S. Food and Drug Administration-approved HPV test, either in conjunction with a Pap (cotesting) or alone (primary HPV testing). 5 Prior results of Pap tests, HPV tests, and cervical biopsies factor into the estimated risk of precancer in the context of a patient's current test results. Obtaining medical records and documenting a patient's prior results is critical for accurately estimating risk and determining when and how often the patient will be followed or evaluated. 5
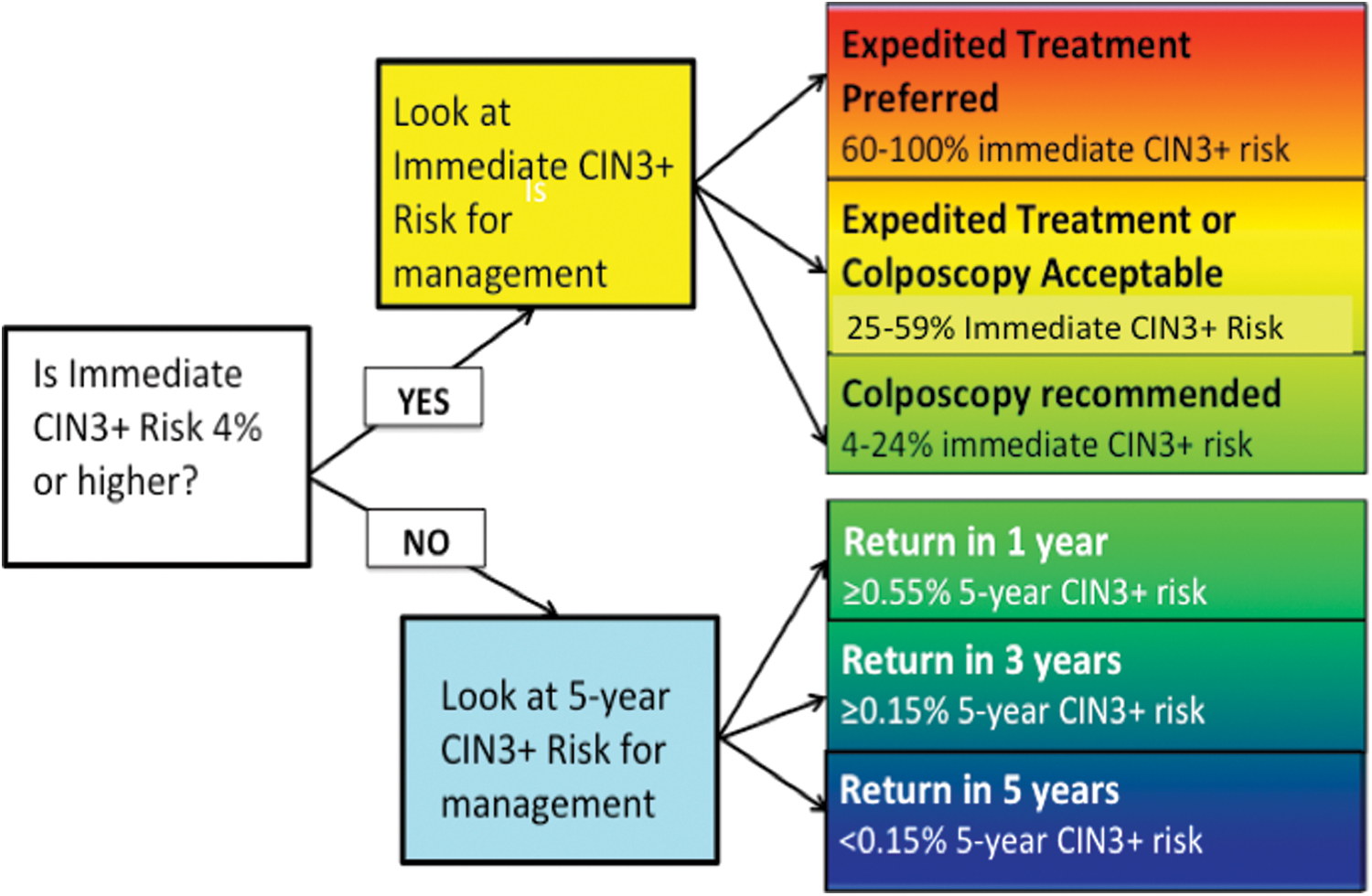
Summarizes the framework of the 2019 Risk-Based Management Consensus Guidelines. Color images are available online.
Colposcopy
Colposcopy with biopsy is performed to determine whether a patient with abnormal screening test results has a precancer or cancer. Colposcopy involves a close examination of the cervix using magnification and usually multiple biopsies of the cervical transformation zone. When a patient is referred for colposcopy, the ASCCP Colposcopy Standards guidelines should be followed to ensure that the colposcopic evaluation was adequate to exclude a high-grade lesion. 30 Colposcopy should include at least one biopsy of all acetowhite or suspicious areas. 30 If the entire transformation zone is visualized and no lesions are present, biopsies may be deferred in women with low prior risk (low-grade squamous intraepithelial lesion [LSIL], atypical squamous cells of undetermined significance [ASC-US] or NILM cytology, no HPV16). 30 Endocervical sampling is recommended in high-risk women without visible lesions and when the entire transformation zone cannot be visualized. 29 When acetowhitening is noted, 2–4 biopsies are considered the standard of care to exclude a high-grade lesion. High-grade lesions are defined in the Bethesda terminology as cervical intraepithelial neoplasia (CIN) grades 2 or 3 or in the LAST terminology as histologic high-grade squamous intraepithelial lesion (histologic HSIL). 31 Older terminology included the terms moderate or severe dysplasia.
Risk modifiers
A patient's estimated risk of currently having cervical precancer is substantially lowered if a patient has a history of normal screening results, with the most recent being a negative HPV test or cotest within the last 5 years. Estimated risk is also lowered if a low-grade abnormal Pap result (ASC-US, LSIL) is preceded by a prior colposcopy, in which no CIN2 was identified, as long as the colposcopy was performed according to the standards described above and occurred within approximately the past 1 year. Conversely, risks are higher when patients have a history of prior positive HPV tests, high-grade Pap tests, or high-grade cervical biopsy results. Other factors, including age, smoking, and use of hormonal contraception, do not typically alter risk after HPV test results and prior screening history are included in the risk estimation. Note that “unknown history” was used as a category when estimating risk. 32 Epidemiologic evidence suggests that increased body mass index may lead to false-negative test results, underscoring the importance of thorough sampling in obese patients. 33 Of note, pregnancy does not change the risk of precancer or its progression to cancer, and colposcopy is recommended during pregnancy if indicated by guidelines. 5 Unless cancer is suspected, however, biopsies may be deferred to the postpartum period. Endocervical sampling is contraindicated during pregnancy, and treatment should be deferred unless cancer is present. 5
Management Summary
Initial management
For most patients with abnormal results on Pap and/or HPV tests, management in 2020 is similar to 2012 guidelines. 5,29 Colposcopy is recommended for most patients with positive HPV tests and abnormal Pap tests. The circumstances, in which patients may either get more or less intensive immediate care than they would have using the 2012 guidelines, are described in Table 2.
Comparison of 2012 and 2019 Consensus Recommendations for Management of Common Abnormalities (ASCCP)
Bold indicates difference between 2012 and 2019 guidelines.
Note colposcopy may be warranted for patients with a history of high-grade lesions (CIN2, CIN3, histologic or cytologic HSIL, ASC-H, AGC, AIS).
Prior Pap results do not modify the recommendation; colposcopy is always recommended for two consecutive HPV-positive tests.
Negative HPV test or cotest (HPV plus Pap test) results only reduce risk sufficiently to defer colposcopy if performed for screening purposes within the last 5 years. Colposcopy is still warranted if negative HPV test or cotest results occurred in the context of surveillance for a prior abnormal result.
Expedited treatment is preferred for nonpregnant patients aged 25 and older. Colposcopy with biopsy is an acceptable option if desired by patient after shared decision-making.
AGC, atypical glandular cells; ASC-H, atypical squamous cells cannot exclude HSIL; ASC-US, atypical squamous cells of undetermined significance; LSIL, low-grade squamous intraepithelial lesion; NILM, negative for intraepithelial lesion or malignancy; Pap, Papanicolaou.
New data indicate that prior history is very important when considering management of common low-grade results: HPV-positive ASC-US or LSIL. When a patient with a history of normal screening results, whose most recent screening test result is a negative HPV test or cotest within a normal screening interval (∼5 years), a new result of HPV-positive ASC-US or LSIL does not indicate a high risk of a current a high-grade precancerous lesion (defined as CIN3 or higher). 32 Risk is low in this case because the infection is revealed to be new and therefore typically benign, regardless of patient age. Therefore, follow-up with HPV testing or cotesting in 1 year is recommended instead of colposcopy.
A colposcopy at which CIN2 was not found also lowers the risk that a patient will develop a cervical precancer within the next year. Specifically, many patients have persistent low-grade results (i.e., HPV-positive NILM, ASC-US, or LSIL), and under 2012 guidelines received colposcopy annually. 29 New risk estimations indicate that a colposcopy where CIN2 was not found, performed within the past year, substantially reduces the risk of developing a high-grade precancerous lesion within the next year. 32 Therefore colposcopy can be deferred in these patients, and follow-up in 1 year is recommended instead. Because persistent HPV infections are an important risk factor for developing cervical precancer, colposcopy is recommended if the patient remains HPV-positive at the 1-year follow-up. 5
For patients whose history is not known, not documented, or includes Pap testing only, management is based on the current Pap and HPV test results, and is largely the same as recommended in 2012. 32 Colposcopy is recommended for all patients with two consecutive positive HPV tests and normal (NILM) Pap test results, and all results of HPV-positive ASC-US or a more severe cytology interpretation. Patients with HPV-negative ASC-US can be followed in 3 years.
Partial HPV genotyping, which is available in several current PCR-based assays, affects risk assessment and management. HPV types 16 and 18 are together responsible for ∼70% of invasive cervical cancers, 34 so these results require particularly close follow-up. At minimum, all patients with HPV 16 and/or HPV 18 infections should undergo colposcopy, even if Pap test results are normal. 5 When HPV 18 is present, endocervical sampling or endocervical curettage (ECC) should be considered at the time of colposcopy due to the association of HPV 18 with adenocarcinomas, which arise from the endocervix. 35
Recognizing that colposcopy is imperfect and that patients may prefer treatment to observation, the 2019 management guidelines give the option of expedited treatment for result combinations where the risk of currently having a precancer (CIN3 or higher) exceeds 25%. Expedited treatment is defined as proceeding directly to an excisional treatment (e.g., loop electrosurgical excision procedure or [LEEP] or large loop excision of the transformation zone [LLETZ]) without requiring a confirmatory colposcopic biopsy. When considering expedited treatment, engaging in shared decision-making with the patient is crucial. Issues to consider include age, concerns about the potential effects of treatment on a future pregnancy, anxiety related to cancer, and desire/ability to undergo repeated colposcopy at 6- and 12-month intervals. 5
Expedited treatment is preferred for patients whose current test results are HPV16-positive HSIL because their current risk of having a CIN2 or higher lesion is 77%. 5 Expedited treatment is also preferred for HPV-positive HSIL regardless of HPV genotype for patients who have not been screened in more than 5 years. Expedited treatment is an option for patients with HPV-positive atypical squamous cells cannot exclude high grade (ASC-H) and for HSIL Pap test results, regardless of HPV status.
Surveillance following diagnostic testing or treatment
After treatment or diagnostic testing for abnormal results, patients are followed closely for several years prior to returning to recommended screening intervals. 5 Surveillance with HPV tests or cotests is preferred because they are more sensitive for detecting new or recurrent precancer (CIN3 or higher). 5 If Pap testing alone is used for surveillance, more frequent intervals are recommended. Specifically, Pap testing is recommended at 6-month intervals when HPV testing or cotesting is recommended annually, and Pap testing is recommended annually when HPV testing or cotesting is recommended at 3-year intervals. 5
Low-grade abnormalities
If a patient has been properly evaluated and there is no evidence of high-grade disease [cytologic HSIL on Pap test results or histologic HSIL (CIN2 or higher) on biopsy], follow-up is generally recommended in 1 year (Table 2). 5 If testing is negative at the 1-year follow-up, then the patient may continue testing with HPV testing or cotesting at 3-year intervals or with Pap testing annually. 5 Data will continue to be evaluated to determine when patients can safely resume regular screening intervals: every 5-years for HPV testing or cotesting and every 3 years for Pap testing. 5 With currently available data, only two scenarios show patients to be at sufficiently low risk to return to routine screening. The first is an HPV-negative ASC-US result followed by negative cotesting. 5 The second is a minimally abnormal result (HPV-positive ASC-US, LSIL, or NILM) followed by a colposcopy, in which CIN2 or higher was not found, followed by three consecutive negative HPV tests or cotests. 5 For all other combinations of results, the number of negative tests required has not yet been defined, so patients may continue with HPV testing or cotesting at 3-year intervals or with Pap testing annually. 5 Recommendations for when to return to routine screening will be updated as more data accrue.
High-grade abnormalities
Following treatment for or resolution of high-grade histologic abnormalities (CIN2, CIN3, HSIL) or high-grade cytologic abnormalities (AGC, ASC-H, HSIL), it is recommended that patients have three consecutive negative HPV tests or cotests before they can begin testing with HPV tests or cotests at 3-year intervals. 32 After the initial intensive surveillance period, patients should continue testing with HPV testing or cotesting at 3-year intervals for a minimum of 25 years. 5 Following conservative treatment of adenocarcinoma in situ (i.e., excisional treatment without hysterectomy) patients should undergo cotesting plus ECC every 6 months for 3 years, and then annually for 2 additional years (5 years total) prior to lengthening to 3-year intervals with HPV testing or cotesting among those with consistently negative test results. 35
Special situations
Management recommendations differ slightly for patients who are immunosuppressed, pregnant, or have undergone hysterectomy. 5 In addition, some situations, such as CIN1 diagnosed repeatedly for more than 2 years, may be managed based on patient preference rather than risk. Specifically, patients with CIN1 are at relatively low risk for precancerous lesions (CIN3 or higher), regardless of the length of time that CIN1 has been diagnosed on biopsy. Treatment is therefore not preferred. However, some patients who have been followed for more than 2 years with CIN1 may elect to undergo treatment. In addition, clinical judgment is important for situations in which prior management has not been consistent with guidelines. Generally, patients who have not been screened within the past 5 years are at higher risk. Prior negative results are not considered valid for risk estimation if a patient has not been screened in >5 years, or has not returned for postcolposcopy follow-up in >1 year. Finally, it is crucial to remember that all the above recommendations apply to asymptomatic patients. Pap testing, HPV testing, and colposcopic as well as endometrial biopsies may be needed to diagnose patients presenting with abnormal uterine bleeding. 21,36
Conclusion
Extensive knowledge about the natural history of HPV infections allows for effective and efficient prevention of invasive cervical cancer. 37 HPV vaccination has been recommended for females aged 9–26 for the prevention of cervical cancer since 2006, and is a crucial step in reducing cervical cancers in the future. 38 However, most adults did not have the opportunity to receive vaccination during adolescence. Therefore, a necessary step in cancer prevention is appropriately screening individuals with a cervix—this includes women and transgender men who have not undergone hysterectomy with removal of the cervix. A review of medical records would determine when screening or follow-up surveillance testing is due. For visits performed via telehealth, a patient could be informed of testing at a subsequent encounter.
A negative screening using HPV testing alone or cotesting is associated with a very low risk of developing CIN3 or higher within the next 5 years. This long-term reassurance can be beneficial in the occurrence of unforeseen disruptions in care, such as occurs following natural disasters, health care emergencies such as pandemics, or economic recessions leading to loss of health insurance. Following an HPV-positive abnormal Pap test result, most patients will undergo colposcopy, and those at very high risk of precancer are eligible for expedited excisional treatment (e.g., LEEP). Risk-based management guidelines are designed to focus resources on high-risk patients, while reducing unnecessary procedures in low-risk patients. Maximizing screening participation, ensuring adequate follow-up, and following risk-based approaches are the key steps to reduce incidence rates of invasive cervical cancer.
Footnotes
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the National Cancer Institute.
Author Disclosure Statement
R.B.P., Mona S., G.F.S., and S.F. have no conflicts of interest to disclose. Mark S. and N.W.: The National Cancer Institute has received cervical screening tests at reduced or no cost from Qiagen, Roche, BD, MobileODT, and Arbor Vita for independent evaluations of screening methods and strategies. R.L.G.: Inovio Pharmaceuticals DSMB, ASCCP Consultant.
Funding Information
The ASCCP guidelines effort received support from the National Cancer Institute and ASCCP. No support was solicited for the development of this article.