
Abstract

Case Report
* A 35-year-old right-hand-dominant gravida 1 para 1 female, 6 weeks postpartum and actively breastfeeding presents with exquisite tenderness over the right wrist when lifting her baby. She has no history of previous symptoms, hand trauma, or surgeries. On physical examination, her pain is recreated with ulnar deviation of the wrist over clasped thumb.
What is your next step in management?
A. Electrodiagnostic Studies
B. Surgery
C. Splinting and NSAIDs
D. Corticosteroid Injection
De Quervain's disease
De Quervain's disease, also known as de Quervain's tenosynovitis, is one of the most common tendinopathies of the wrist. It is defined as tendon entrapment of the first extensor tendon compartment of the wrist resulting in tenderness and pain over the dorsoradial aspect of the wrist. 1 The dorsum of the wrist has six separate compartments under the dorsal carpal ligament where the tendons of the forearm extensor muscles pass from the distal forearm to the fingers. These tunnels serve to keep extensor tendons close to the body and prevent from bowstringing. The first extensor compartment contains the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendon, which are responsible for abduction of the carpometacarpal joint and extension of the interphalangeal joint of the thumb, respectively (Fig. 1). The first compartment is a narrow osteoligamentous tunnel formed by a shallow groove of the radial styloid process and fibers of the dorsal ligament.
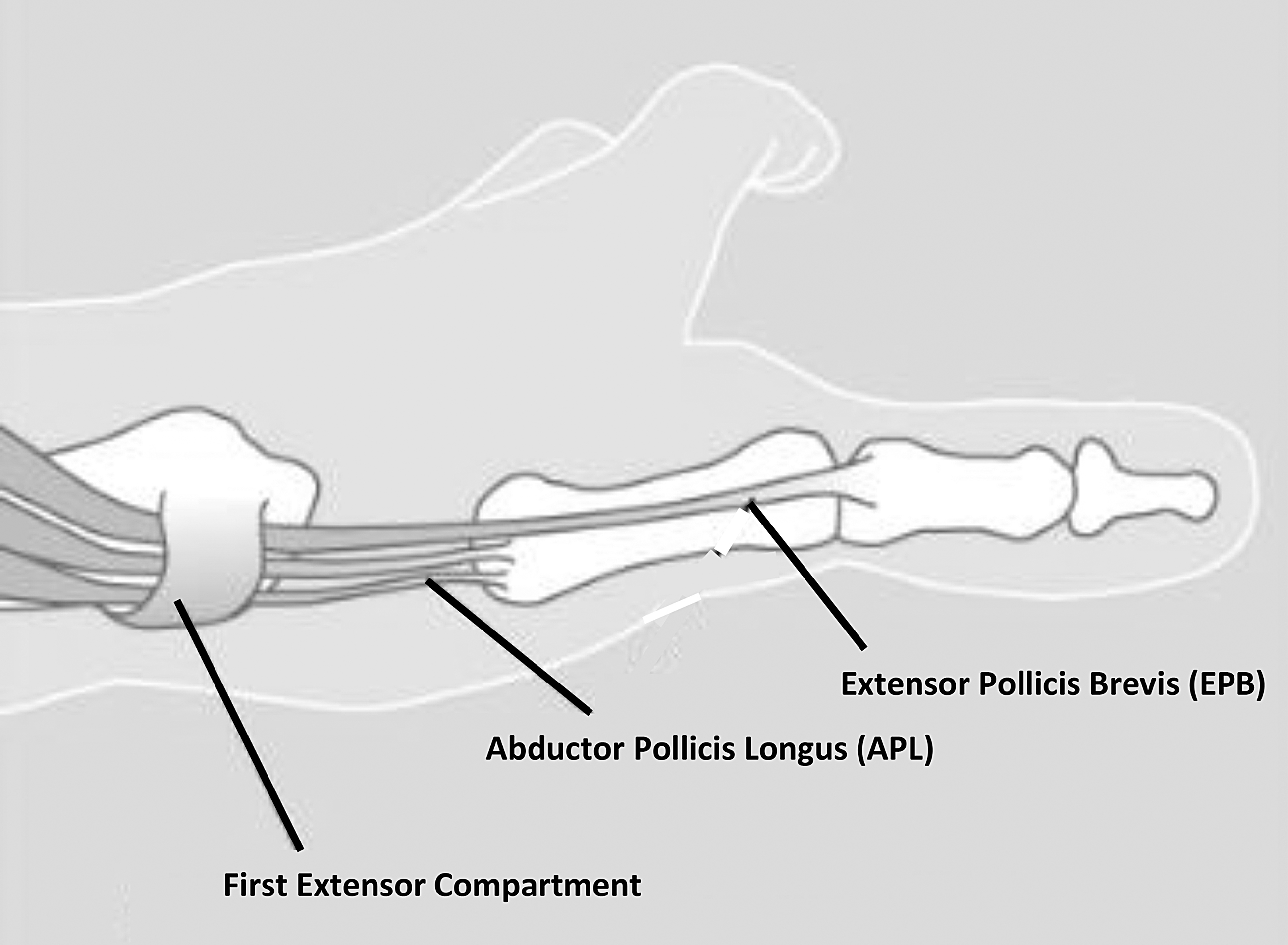
Anatomy of the first extensor compartment. Reprinted with permission from The American Society for Surgery of the Hand.
The etiology of de Quervain's disease is unknown. It is hypothesized that the osteoligamentous tunnel, a natural bottleneck in the wrist, becomes narrowed causing inflammation, further stenosis, and subsequent pain. Repetitive activities with frequent abduction and concurrent ulnar deviation of the wrist are thought to precipitate the condition. In addition, the extensors of the forearm have highly variable anatomy and are thought to contribute to increased susceptibility to the disease and failure of conservative treatment in some individuals. 2,3
The diagnosis is made through history and physical examination and it more commonly affects women than men. There is a bimodal patient distribution with the majority of patients in their 50s and 60s and in women who are postpartum or lactating. 1,4 –6 Patients typically present with radial sided pain and tenderness. The Finkelstein maneuver is the classic provocative test for de Quervain's disease. A Finkelstein maneuver is positive when significant pain occurs over the radial styloid when the thumb is placed in the palm and the wrist is ulnarly abducted (Fig. 2). 7 A positive Finkelstein maneuver is generally pathognomonic for disease; however, the differential diagnosis includes intersection syndrome, trigger thumb, and arthritis of the thumb carpometacarpal joint and scaphotrapezial-trapezoid joint. 1,2 If history and examination are classic for de Quervain's disease, radiographs are not absolutely necessary; however, there should be a low threshold for wrist radiographs to evaluate for other etiologies of radial sided wrist pain.

Finkelstein maneuver is the classic provocative test for de Quervain's disease. Pain over the radial styloid when the thumb is placed in the palm and the wrist is ulnarly abducted.
Treatment includes nonsurgical and surgical modalities. Nonsurgical modalities include avoidance of aggravating activities, nonsteroidal anti-inflammatory drugs (NSAIDs), splinting, and corticosteroid injection. 1,8,9 Activities that include repetitive thumb extension and abduction should be avoided. Splinting can be helpful for some patients as well as NSAIDs. 9 If these modalities fail to improve symptoms, corticosteroid injection of the first dorsal compartment is indicated. 8,9 Corticosteroid injection has been shown to improve symptoms 50%–80% with one or two injections. 9 Recent data suggest that if patients decide to undergo corticosteroid injection then splinting provides no additional benefit. 9,10
Surgery is indicated for continued pain after nonsurgical treatment. Likely failure of corticosteroid injection is due to variable anatomy, long-standing de Quervain's, or diabetes mellitus. 2,3,9 Surgery involves release of the first extensor compartment of the wrist. Surgery is typically outpatient and can be done with local anesthetic. A small incision is made ∼1 cm proximal to the radial styloid and extends the length of the extensor compartment, which is 2 cm. 1 The APL and EPB tendons are released and confirmed intraoperatively that they glide without restriction and any septum in the compartment is released. Postoperative management includes elevation, rest, and then gentle tendon gliding exercises. Typical recovery time is 4 weeks. Risks of the procedure include damage to the dorsal sensory branch of the radial nerve, incomplete release of all the septum of the compartment, subluxation of the tendons after release, bleeding, infection, and need for reoperation. Risks of complications are low, and patient satisfaction is high. 11,12
Answer: The Best Answer Is C
Originally described in the 1893 edition of Gray's anatomy, de Quervain's was named “washer-woman's sprain.” 1 It has subsequently been called many other colloquial names, including Blackberry thumb, texting thumb, gamer's thumb, designer's thumb, mother's wrist, and mommy thumb. As discussed earlier, the incidence is bimodal with the highest incidence in women in their 50s and 60s but also during the postpartum period. 1,4 –6 Studies find this typically presents 2–6 weeks after delivery. 6 Incidence and etiology are currently unknown. One hypothesis is that the repetitive thumb extension and abduction seen in new mothers when holding their newborn precipitates symptoms. Another hypothesis is hormonal changes that cause fluid retention narrows the tunnel causing inflammation and pain. 13
Treatment options are similar to de Quervain's disease outside of postpartum period, but typically postpartum and lactating women do well with nonsurgical treatment. 4,6 Surgery is rarely indicated. Nonsurgical modalities are similar to discussed earlier, including avoidance of provocative activities, splinting, NSAIDs, and corticosteroid injection. Splinting has shown minimal to modest improvement, and NSAIDs can have benefit and are safe in the postpartum period. 6,14 If these modalities fail, corticosteroid injection of the first dorsal compartment appears to work well and are safe for postpartum patients. 6,14
In general, de Quervain's disease in the postpartum and lactating female is self-limited. For our postpartum and lactating women, it is our practice to optimize nonsurgical treatment with avoidance of provocative activities, splinting, and NSAIDs (typically 800 mg of Ibuprofen every 8 hours). If these modalities fail or symptoms are severe, we recommend corticosteroid injection. The majority of patients' symptoms resolve after discontinuation of nursing period.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.