
Abstract
Background:
The Institute of Medicine (IOM) has provisional gestational weight gain (GWG) guidelines for women pregnant with twins due to limited data in this population. To better inform guidelines, the objective of this systematic review was to build on prior work and examine recent data on the associations of GWG with maternal and child health in twin pregnancies.
Materials and Methods:
In February 2021, Ovid MEDLINE, Embase, CINAHL, and Cochrane Library were searched. Observational studies were eligible if published from January 1, 2013 through February 23, 2021, and examined associations of GWG with maternal or child health outcomes after accounting for gestational age at delivery and pre-pregnancy body mass index. Heterogeneity across studies precluded the use of meta-analytic methods.
Results:
A total of 29 studies were included. For maternal outcomes, excessive GWG was associated with an increased risk of hypertensive disorders of pregnancy; whereas studies examining gestational diabetes and delivery method reported mixed findings. For child outcomes, inadequate GWG was associated with lower birthweight, small for gestational age, and preterm birth. Adequate or excessive GWG was associated with later gestational age at delivery.
Conclusions:
This study advances an earlier review by including a more diverse array of maternal and child outcomes. Many of the limitations noted in the original review persist; for example, no studies examined the associations of GWG and outcomes beyond birth. Although it appears that GWG within the IOM guidelines is associated with more optimal outcomes, additional methodologically rigorous studies are needed to better inform evidence-based guidelines.
Introduction
The rate of twin pregnancies in the United States has increased for three decades, accounting for nearly 1 in 30 births in 2009. 1 Compared with women with singleton pregnancies, women pregnant with twins are at greater risk for adverse maternal outcomes, including higher rates of gestational diabetes, hypertensive disorders, premature rupture of membranes, cesarean delivery, postpartum hemorrhage, and maternal mortality. 2 –6 Further, there is a greater risk of adverse neonatal outcomes in twin pregnancies, including intrauterine growth restriction, preterm birth, low birth weight, and perinatal mortality, compared with singleton pregnancies. 7 –9 One potentially modifiable factor that may exacerbate health risks in this already vulnerable population is inadequate or excessive gestational weight gain (GWG).
The Institute of Medicine (IOM) provides specific GWG guidelines for women with singleton pregnancies based on pre-pregnancy body mass index (BMI) category to optimize health outcomes for mother and baby. 10 However, the GWG guidelines for women with twin pregnancies are cited as provisional due to limited data in this population, and no GWG guidelines currently exist for women pregnant with twins with an underweight pre-pregnancy BMI (<18.5 kg/m2). There is an imperative need for additional research to examine the associations of GWG with maternal and child outcomes in twin pregnancies to provide evidence to support or revise the current provisional guidelines to improve health outcomes in this population.
A systematic review was published in 2014, and it examined the literature on GWG in twin pregnancies and implications for maternal and child outcomes. 11 In this article, Bodnar et al. identified 15 articles that met their inclusion criteria, reporting a consistent positive association between GWG and fetal growth. Data were inconsistent for preterm birth and pregnancy complications. The authors noted that the included studies failed to properly account for chorionicity as well as the correlation between length of gestation and GWG, and serious perinatal outcomes were not considered.
Since the publication of their systematic review, there has been a substantial increase in the number of publications examining the associations of GWG with maternal and child outcomes in twin pregnancies. Therefore, the objective of this article is to systematically review the literature published after the Bodnar et al. review to assess the associations of GWG with maternal and child outcomes in twin pregnancies using the most up-to-date knowledge in the field. This review does not include the 15 articles from the Bodnar et al. review due to the identified limitations in the previously published studies, and to show how the field has advanced by making a clear distinction between our systematic reviews.
Materials and Methods
A systematic review of the literature was performed to assess the association between GWG in twin pregnancies and maternal and child outcomes. The study was registered by The International Prospective Register of Systematic Reviews (PROSPERO; CRD42020206168) and followed the criteria outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 12,13 This study was exempt from Institutional Review Board review.
Information sources and search strategy
The searches were developed and conducted by a health sciences librarian who was trained in systematic review searching. Preliminary searching was conducted by using the strategy from Bodnar et al. using additional relevant subject headings and keywords to ensure that the first review had located the relevant studies published before 2013. Then, search strategies employing expanded sets of subject headings and keywords were created for Ovid MEDLINE [resource OvidMEDLINE(R) ALL], Embase (
The searches were conducted on November 22 of 2019 and updated on February 23 of 2021. The results in each database were limited to studies in English, and the dates included from 2013 up to the dates of searches. The search strategies are available in Supplementary Table S1. Database records were de-duplicated by using a systematic method. 14 The number of records retrieved for each database can be found in Figure 1. Reference lists of included articles were also screened.
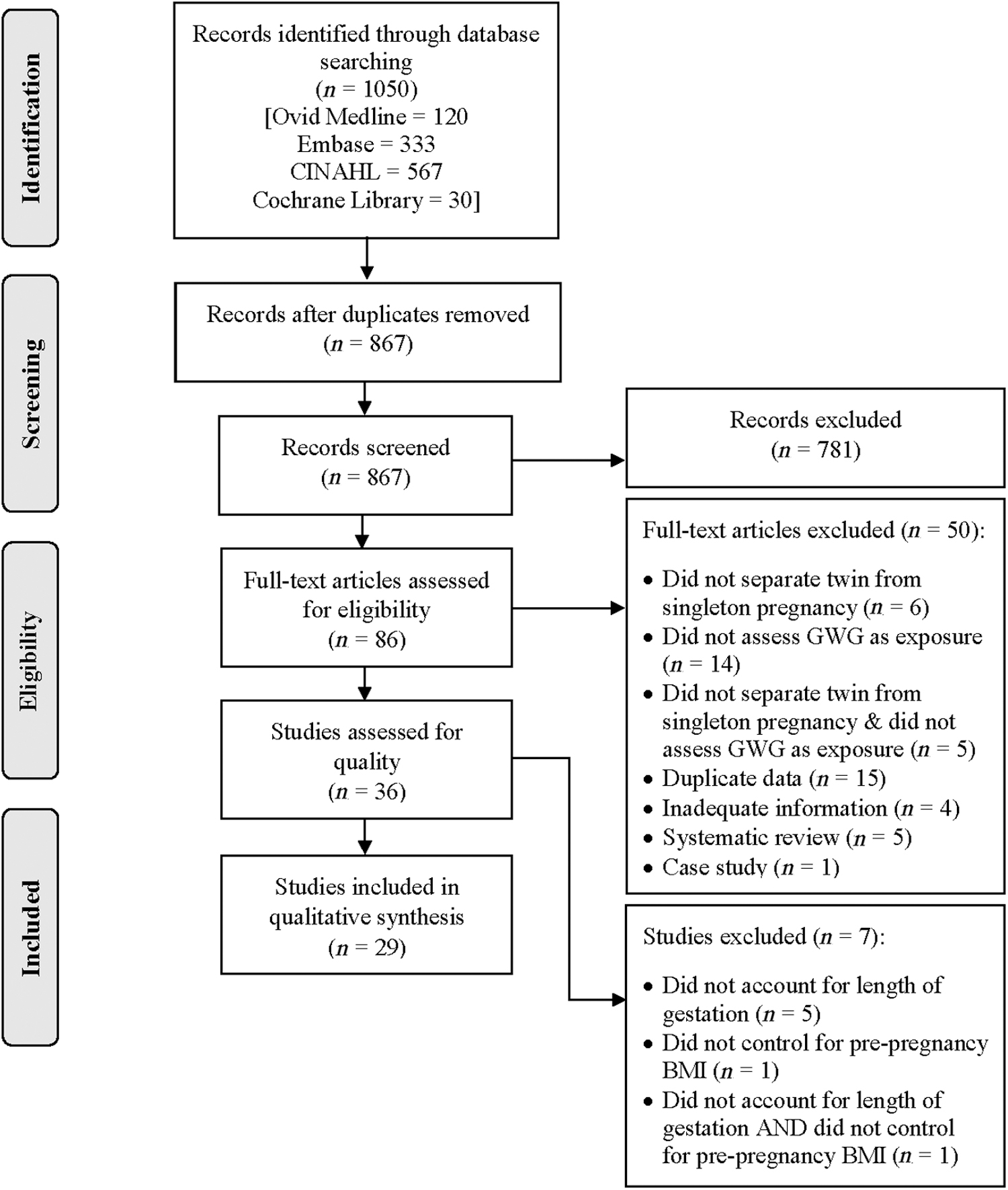
PRISMA flow diagram. BMI, body mass index; GWG, gestational weight gain; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Eligibility criteria
Studies were included if they studied GWG (exposure) in twin pregnancies and examined maternal and/or child health (outcome). The PICOS selection criteria (population, intervention or exposure, comparison, outcome, study design), were as follows: The population included women with twin pregnancies, the intervention/exposure was weight gain within the IOM provisional GWG guidelines for twin pregnancies, the comparison was weight gain below or above the IOM provisional GWG guidelines for twin pregnancies, the outcome was maternal and/or child outcomes, and the study design included cohort or case–control studies. We excluded case studies given the limited ability to generalize findings from one individual to the broader population, as well as systematic reviews.
Study selection
Two independent reviewers (C.B. and R.R.) screened the titles and abstracts yielded by the search against the inclusion criteria. Abstracts judged to have met the initial screening criteria were retrieved as full-text articles. The same two independent reviewers screened the full-text articles based on PICOS selection criteria for inclusion in the final review. Disagreement between the two reviewers was resolved by a third reviewer (K.M.W.), who had completed training in systematic literature reviews and meta-analytic methods. Reasons for exclusion were recorded. A similar review process has been previously used by this team of reviewers. 15
Fifteen studies were excluded due to duplicate data. 16 –30 Many were abstracts that included the same population as a full-text article. 16 –23,25 –29 An exception was made for two articles published by Pettit et al. 22,31 because, although they included the same population, the two articles reported different outcomes.
Data abstraction and synthesis
Data were extracted with the use of a predesigned template and included details of the study (e.g., year published, location, sample size) and data on study participants (e.g., age, race/ethnicity). In addition, several aspects of the study methods were extracted, including, but not limited to, GWG assessment methods and control variables. For the results, two reviewers (C.B. and R.R.) independently abstracted the percentage of women with GWG below, within, and above guidelines; maternal and child outcomes; and effect estimates. Disagreement between the two reviewers was resolved through discussion, with a third reviewer (K.M.W.) verifying all data abstraction.
If studies described GWG below, within, or above IOM guidelines for sub-groups (e.g., normal, overweight, and obese pre-pregnancy BMI groups), we calculated the percentage of women overall with GWG below, within, or above guidelines to enhance comparability across studies. 32 –36 To estimate the mean percentage of twin pregnancies with GWG classified as below, within, and above IOM guidelines, pooled averages were calculated by summing the mean values multiplied by the sample size and dividing this number by the sum of the sample sizes. Only studies that reported GWG for all categories (below, within, and above IOM guidelines) were included in these calculations. Three studies were not included, because they only reported the percentage of women gaining below or within IOM guidelines. 22,30,37 Formal meta-analytic methods were not used to estimate the effect of the exposure on the outcome because of heterogeneity in the included studies.
Assessment of study quality
The quality of each study was assessed by using existing criteria from the systematic review article by Bodnar et al. 11 First, studies were evaluated to see whether the measure of GWG accounted for length of gestation and whether they controlled for pre-pregnancy BMI. Seven studies were excluded that did not meet these initial criteria. 18,38 –43
The studies that did meet these criteria were then assessed by using the following metrics: (1) were results presented separately for women in each pre-pregnancy BMI category in relation to the outcomes; (2) was GWG based on self-reported or measured weight at delivery; (3) was the pattern of GWG studied in relation to the outcomes; (4) were chronicity and assisted reproductive technologies examined as confounders or effect modifiers; (5) did the study control for covariates other than gestational age and pre-pregnancy BMI that may confound the GWG-adverse outcome association; and (6) was gestational age confirmed by ultrasound.
Initially, two reviewers (C.B. and R.R.) independently rated the studies by using the unique criteria from the Bodnar et al. article, with ∼70% agreement. A third reviewer (K.M.W.) was consulted, and conversations were initiated that resulted in 100% agreement among all three reviewers.
Results
Assessment of study quality is reported in Table 1. Nine of the 29 included studies presented results separately for women in each pre-pregnancy BMI category. 31 –34,36,37,44 –46 If the GWG assessment method was reported, nearly all studies obtained GWG through chart abstraction or study measurement, with one study using self-reported GWG 37 and a second using a combination of self-reported and measured weight. 32
Assessment of Study Quality
1: Did the measure of GWG account for length of gestation? (Y/N). 2: Did the study control for pre-pregnancy BMI? (Y/N). 3: Were results presented separately for women in each pre-pregnancy BMI category in relation to the outcomes? (Y/N). 4: Was GWG based on self-reported or measured weight at delivery? (Self-report/Measured). 5: Was the pattern of GWG studied in relation to the outcomes? (Y/N). 6. Were chorionicity and assisted reproductive technologies examined as confounders or effect modifiers? (Y/N and specify separately for chorion. and ART). 7: Did the study control for covariates other than GA and pre-pregnancy BMI that may confound the GWG-adverse outcome association? Examples include maternal race/ethnicity, age, smoking, and socioeconomic status. (Y/N). 8: Was GA confirmed by ultrasound? (Y/N).
GWG based on medical record abstraction.
ART, Assisted Reproductive Technologies; BMI, body mass index; GA, gestational age; GWG, gestational weight gain; NA, not applicable; NS, not specified.
Eight studies reported information on patterns of GWG in relation to study outcomes. 30,35,47 –52 Thirteen studies reported examining chorionicity, 22,30,31,35,37,45 –47,50,53 –56 and 18 studies reported examining assisted reproductive technology 22,30 –32,35 –37,45,47 –49,52 –55,57 –59 as a confounder or effect modifier. All but seven studies 35,47,51,53,57,60,61 reported controlling for covariates other than gestational age and pre-pregnancy BMI, such as maternal age or race/ethnicity. Thirteen studies reported confirmation of gestational age via ultrasound. 30,32,35,44,45,47 –50,53,54,57,59
Table 2 depicts the characteristics of the included studies and populations. Of the 29 studies included in the review, all but 147 were cohort study designs. Five of the 29 studies were abstracts. 33,51,56,58,62 The 29 studies included for qualitative synthesis resulted in a final sample size of 224,383 women (range within studies of 20–167,121 women). Notably, the abstract by Ram et al. 51 did not report a sample size, stating that they included a “large cohort of twin pregnancies”; therefore, the total sample size can be inferred to be >224,383 women. The 13 studies that reported data on race/ethnicity included predominately (>50%) white participants. 22,30 –32,35 –37,45,47 –50,63
Study Characteristics
N = 224,383 women.
Not reported in the article but adequate details provided to calculate.
Study also included 6138 singleton pregnancies but reported the data separately for each population.
SD, standard deviation.
Twelve studies were conducted in the United States, 22,31,32,36,37,45,47 –49,58,62,63 four studies were conducted in China, 44,52,54,61 six did not specify a location, 30,33 –35,51,56 and the remainder were conducted in Italy, 53 Korea, 46 Poland, 57 Slovenia, 60 Canada, 50 France, 55 and Japan. 59
A summary of the GWG assessment method, IOM guideline adherence, and confounding variables for each of the included studies can be found in Table 3. Five studies utilized a measure of total GWG, 37,44,48,59,63 12 studies utilized a weekly rate of GWG, 22,31,34,35,45,46,50,54,55,57,58,61 and 2 studies utilized a combination of both total and rate of GWG. 36,53 A unique approach to GWG measure was used in seven studies (e.g., z-scores or weight gain over distinct time frames), 30,32,47,49,52,56,60 whereas three studies did not specify how GWG was assessed. 33,51,62
Summary of Findings on Gestational Weight Gain Assessment Methods, Institute of Medicine Guideline Adherence, and Control Variables
Not reported in the article but adequate details provided to calculate.
IOM guideline corrected for GA, a validated gestational week-specific guideline (Guideline A), and a GA-specific guideline that we developed consisting of the IOM singleton GWG recommendation plus the contribution of an additional fetal–placental unit, including the estimated amniotic fluid weight, placental weight, and the “ideal” fetal weight (Guideline BK).
IOM, Institute of Medicine; PTB, preterm birth.
To obtain either a rate or total for GWG, chart abstraction was used in 15 studies 22,30,31,34 –36,44,45,47,48,52 –54,60,63 whereas a mix of chart abstraction and self-report was used in 7 studies. 32,37,46,49,50,57,59 The abstraction method was not specified in the remaining seven studies. 33,51,55,56,58,61,62 Overall, 31.6% of women reported GWG below IOM guidelines, 43.5% of women reported GWG within IOM guidelines, and 24.9% of women reported GWG above IOM guidelines. Covariates most consistently adjusted for in analyses included maternal age, race/ethnicity, parity, pre-pregnancy BMI, and health conditions.
Maternal outcomes
As seen in Table 4, 22 studies reported findings on GWG and maternal outcomes. Twenty studies examined gestational hypertensive disorders. Excessive or higher GWG was associated with greater odds of gestational hypertensive disorders in 11 of the studies. 22,31,33,34,36,53 –55,58,59,63 In addition, six studies found that compared with adequate GWG, low GWG was associated with lower odds of gestational hypertensive disorders. 30,34,36,46,55,58 Seven studies found no association between GWG and gestational hypertensive disorders. 35,37,45,52,57,60,61
Summary of Findings on Gestational Weight Gain in Twin Pregnancies and Maternal Outcomes
AGWG, adequate gestational weight gain; aOR, adjusted odds ratio; CI, confidence interval; EGWG, excessive gestational weight gain; GDM, gestational diabetes mellitus; HELLP, Hemolysis, elevated liver enzymes, and low platelets; LGWG, low gestational weight gain; NW, normal weight; OB, obese; OR, odds ratio; OW, overweight; UW, underweight.
Fifteen studies examined gestational diabetes. Low or adequate GWG was associated with an increased risk of gestational diabetes in five of the studies. 34,36,46,54,60 Ten studies found no association between GWG and gestational diabetes. 22,30,31,35,37,52,53,55,57,61 Thirteen studies examined delivery method: 3 found a positive association between GWG and cesarean delivery, 32,58,63 and 10 studies found no association between GWG and delivery method. 22,31,35,37,50,54,55,57,59,61 In summary, the reviewed studies indicate that excessive GWG is associated with gestational hypertensive disorders, and there is limited evidence on the association of GWG with gestational diabetes or delivery method.
Child outcomes
All but one included study examined GWG and child outcomes. 60 As seen in Table 5, 10 studies examined the association between GWG and gestational age. The overall findings from seven of these studies indicated that adequate and excessive GWG were associated with a greater gestational age at delivery and a lower risk of delivering early, whereas low GWG was associated with a shorter gestational age at delivery. 30,31,34,37,45,53,63 One of these seven studies examined different time periods during pregnancy and found that low GWG from 24 weeks delivery was associated with shorter gestational age but GWG from 0 weeks delivery, 0–16 weeks, or 16–24 weeks was not associated with gestational age. 30 Two studies reported no association between GWG and gestational age, 35,50 and one study conversely found excessive GWG to be associated with shorter gestational age. 57
Summary of Findings on Gestational Weight Gain in Twin Pregnancies and Child Outcomes
HR, hazard ratio; IUGR, intrauterine growth restriction; LGA, large for gestational age; LGWG, low gestational weight gain; NICU, neonatal intensive care unit; PPROM, preterm premature rupture of membranes; PROM, premature rupture of membranes; SGA, small for gestational age; sPTB, spontaneous preterm birth; sVPTB, spontaneous very preterm birth; VPTB, very preterm birth.
Out of the 25 studies that reported associations of GWG with child size (birthweight, small for gestational age [SGA], and/or large for gestational age [LGA]), 13 studies found low GWG to be associated with lower birthweight 22,30,33 –35,48,50,53,55,58,59,61,64 and 7 studies found low GWG to be associated with SGA. 30,32,35,36,44,46,50
Three studies found excessive GWG to be associated with LGA, 32,36,54 and 10 studies found that excessive or higher GWG was associated with greater birthweight. 30,31,33 –35,48,53,54,58,64 Overall, adequate and excessive GWG were shown to be associated with higher birthweight and lower odds of delivering twins <2500 and <1500 g; only one study found excessive GWG to be associated with lower birthweight. 45 Hinkle et al. reported a pattern for GWG and child size, finding that GWG between 14–20 and 21–27 weeks was associated with higher estimated fetal weight the following week and higher twin birthweight in general. 49 Five studies found no association between GWG and SGA, 22,52,54,56,57 with two additional studies finding no association between GWG and SGA, <5th percentile specifically. 35,50
The association between preterm birth (definitions varied by study) and GWG was investigated in 20 studies. Fourteen studies found a significant association between low GWG and greater odds of preterm birth. 30 –32,36,37,45 –47,51,53 –55,58,62 Six studies found an association between excessive GWG and greater odds of preterm birth. 32,45,53,57,58,61 One study indicated that low GWG was associated with a lower incidence of preterm birth when compared with adequate and excessive GWG, but only simple bivariate analysis was performed. 35 Five studies found no association between GWG and preterm birth. 31,35,50,54,57
Other child outcomes beyond GA, infant size, and preterm birth were examined in 17 studies. Low GWG was overwhelmingly associated with adverse child outcomes when compared with adequate or excessive GWG. Women with low GWG were found to have children with an increased risk of death, 32 Neonatal Intensive Care Unit (NICU) admission, 33,37,46,58 longer length of NICU stay, 50 respiratory distress syndrome, 55 premature rupture of membranes, 35 and Apgar scores <7 at 5 minutes or low Apgar scores in general. 58 One study found that low GWG from 20 to 28 weeks' gestation was associated with intraventricular hemorrhage, necrotizing enterocolitis, hyperbilirubinemia, and a length of hospital stay >30 days. 22
Significant findings for excessive GWG included an association with higher risk of child death in women without obesity, 32 higher odds of Apgar scores <7 at 5 minutes, 55 and lower odds of needing neonatal antibiotics. 58 However, several studies found no association between GWG and adverse child outcomes such as 1- or 5-minute Apgar scores, 46,64 fat mass percentage, 48 mortality, 55,64 NICU admission, 50,54,55 respiratory distress syndrome, 50,54 intrauterine fetal demise, 35 hypoglycemia, 50 sepsis, 55 growth discordance, 56 intrauterine growth restriction, 45 and premature rupture of membranes. 45,46
Overall, low GWG is associated with greater odds of adverse child outcomes such as earlier gestational age at delivery, lower birthweight, SGA, and preterm birth; whereas adequate and excessive GWG are associated with more positive child outcomes, including later gestational age at delivery, lower risk of preterm birth, and higher birthweight.
Discussion
This systematic review summarized the existing literature on the associations of GWG and maternal and child outcomes among women pregnant with twins. We identified 29 studies that met our inclusion criteria that were published after the 2014 systematic review on this topic by Bodnar et al. 11
The majority of studies included in this review examined the associations of GWG with one or more maternal outcomes, and all but one study 60 examined associations with child outcomes. For maternal outcomes, the most consistent finding was that excessive GWG was associated with an increased risk of hypertensive disorders of pregnancy, whereas studies examining gestational diabetes and delivery method reported mixed findings. For child outcomes, the most consistent findings were that low GWG was associated with lower birthweight, SGA, and preterm birth. Further, adequate or high GWG was associated with later gestational age at delivery.
Compared with the review by Bodnar et al., our systematic review reports findings related to a more diverse array of maternal and child outcomes. For maternal outcomes, the original review only reported on hypertensive disorders and gestational diabetes, and data were limited due to both number (n = 3) and methodology of included studies. In the current review, the associations between GWG and hypertensive disorders were examined in 20 studies, gestational diabetes in 15 studies, and delivery method in 13 studies.
For child outcomes, Bodnar et al. discussed findings on fetal growth, preterm birth, and optimal neonatal outcomes. In the current review, we assessed gestational age, child size (including SGA, LGA, and birthweight), preterm birth, and several other adverse outcomes. Our findings on preterm birth, SGA, and birthweight are consistent with those reported by Bodnar et al. (e.g., low GWG associated with higher risk of these outcomes), providing additional evidence supporting these associations with a larger number of studies and also expanding into additional domains of child outcomes.
The number of studies examining the associations of GWG with maternal and child outcomes has increased rapidly. Many of the included studies in this review were large in sample size, thus allowing for stratification by pre-pregnancy BMI category, which is a notable advancement in the literature. Further, the current review also examined additional maternal and child outcomes, including delivery method and perinatal mortality, which were notably absent from the earlier review. The number of diverse, population-based cohorts used to examine GWG and adverse maternal/child outcomes is also growing.
Despite these strengths, there are several methodological concerns identified by Bodnar et al. that persist. For example, all studies were observational, and although the majority of articles controlled for confounders beyond pre-pregnancy BMI and gestational age, confounding bias or residual confounding is a concern. In addition, the majority of studies examined total GWG or weekly rate of weight gain, which does not adequately account for the correlation between gestational duration and total weight gain. 65 Although the rate of weight gain is an improvement over total GWG, this assumes that weight gain during pregnancy is linear over all pregnancy trimesters, when weight gain is typically higher in the second and third trimesters compared with the first trimester. One study included in the current review used maternal weight gain for gestational age z-scores, 32 which better addresses the correlation between gestational duration and GWG and should be considered in future studies.
Compared with the Bodnar review where only 20% of included studies accounted for chorionicity in analyses, nearly 50% of the studies included in this current systematic review examined chorionicity. Although it remains unclear whether GWG differs by chorionicity status, it is well known that women with monochorionic pregnancies are at higher risk for adverse outcomes compared with dichorionic pregnancies, 66 making this an important factor to consider.
An additional methodological issue that persisted in the current review is an inadequate consideration given to the timing of diagnosis for hypertensive disorders and gestational diabetes. The majority of these studies used total or rate of GWG, whereas a more appropriate approach examined GWG before diagnosis, given that the diagnosis of these conditions may alter total GWG.
For example, of the 15 studies included in the current review that examined GWG and gestational diabetes, 5 studies found an increased risk of gestational diabetes in women gaining below or at IOM guidelines, which seems counterintuitive. One potential explanation is that women who are diagnosed with gestational diabetes are more likely to receive intensive dietary recommendations that could have an impact on their GWG, unlike pregnant women who do not receive a gestational diabetes diagnosis and therefore do not receive this type of counseling. The subsequent lifestyle changes may reduce the total amount of weight that these women gain overall during their pregnancy.
Conclusions
Based on our review of the literature, weight gain within the 2009 IOM provisional GWG guidelines for twin pregnancies seems to confer optimal health outcomes for the mother and children. More specifically, the evidence suggests that excessive GWG in twin pregnancies may increase the risk of hypertensive disorders of pregnancy for the mother, whereas low GWG is associated with several increased risks for the children. No studies provided recommendations for optimal GWG ranges that fell outside the current ranges recommended by the IOM guidelines.
Moving forward, we have identified multiple areas that require further study on this topic. First, we did not identify any studies that examined GWG with longer-term outcomes, such as childhood obesity. Given the evidence indicating that excessive GWG is associated with increased risk of childhood obesity in singleton pregnancies, 67 –69 this is an important area of research for future work. Further, the optimal weight gain recommendations for women pregnant with twins in the extreme BMI categories, including underweight and extreme obesity, remain understudied. Given the growing evidence suggesting that gaining weight within the IOM provisional GWG guidelines for twins results in reduced risk of adverse outcomes for women and children, there is a clear need for randomized controlled trials of GWG interventions among twin mothers to improve health outcomes in this high-risk population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.