
Abstract
Background:
Chronic disease is associated with increased risk of postpartum mental illness, but the mechanisms underlying this association are unclear. Our aim was to explore the mediating role of perinatal complications in the association between chronic disease and postpartum mental illness.
Materials and Methods:
This was a population-based retrospective cohort study of all women in Ontario, Canada, from 2005 to 2015 with a singleton live birth and no recent history of mental illness during or 2 years before pregnancy. The outcome was mental illness diagnosis between delivery and 365 days postpartum, with perinatal complications, including pregnancy, delivery, and neonatal complications. Modified Poisson regression models were used to examine the association between chronic disease and perinatal mental illness, with generalized estimating equations for the calculation of total, direct, and indirect effects. All models were adjusted for sociodemographic characteristics and remote history of mental health care.
Results:
Of the 792,972 women, 21.1% had a chronic disease. Chronic disease was associated with an increased risk of postpartum mental illness (adjusted relative risk [aRR] 1.15 [95% confidence interval, CI 1.14–1.16]). There was no evidence of an indirect effect of chronic disease on postpartum mental illness via perinatal complications (aRR 1.003, 95% CI 1.002–1.003). Perinatal complications explained only 1.5% of the association between chronic disease and postpartum mental illness. Results were consistent by type of perinatal complication and chronic disease diagnosis.
Conclusion:
We observed no clinically meaningful mediating effect of perinatal complications in the association between chronic disease and postpartum mental illness. Future research should investigate alternative mechanisms explaining this association.
Introduction
One in 10 pregnant women has a chronic disease such as diabetes, heart disease, and asthma. 1,2 The rate of chronic disease in pregnancy is rising rapidly 1,2 due to the increasing prevalence of advanced maternal age 3 and maternal obesity. 4 As such, there has recently been a major research focus on the impact of chronic disease on pregnancy-related outcomes to inform development of appropriate services and interventions to reduce the risks of adverse perinatal outcomes among women with chronic disease. Chronic disease is a well-established risk factor for perinatal complications such as preeclampsia, eclampsia, Cesarean delivery, preterm birth, and low birthweight. 5 –7 Emerging evidence also suggests that chronic disease is associated with an increased likelihood of the development of postpartum mental illness, with a recent meta-analysis reporting a pooled odds ratio of 1.44 (95% confidence interval [CI]: 1.13–1.85). 8 This association has important public health implications since postpartum mental illness can have a negative impact on both maternal and child well-being. 9,10 Understanding factors explaining the association between chronic disease and postpartum mental illness could point to possible mechanisms and interventions.
The association between chronic disease and postpartum mental illness builds on literature in the general population demonstrating a link between chronic disease and mental illness, which is thought to be explained by the stress associated with chronic disease management or with common risk factors for both chronic disease and mental illness, including genetic factors, inflammation, and hypothalamic-pituitary-adrenal axis dysfunction. 11 –14
However, in obstetric populations, the potential role of perinatal complications in partially explaining the association between chronic disease and postpartum mental illness has not been explored. Such a mediating role is plausible, given the established relationship between chronic disease and perinatal complications 5 –7 and emerging evidence of an association between perinatal complications and postpartum mental illness. 15,16 For example, several meta-analyses have demonstrated an increased risk of postpartum depression, as well as more severe depression symptoms, associated with preeclampsia, 17 cesarean delivery, 18 and preterm birth, 19 with maternal stress resulting from these complications thought to explain this elevated risk. However, whether perinatal complications mediate the relationship between chronic disease and postpartum mental illness has not been examined.
As such, this study aimed to examine the mediating role of pregnancy, delivery, and neonatal complications in the association between chronic disease and postpartum mental illness.
Materials and Methods
Study design
This was a population-based retrospective cohort study that utilized Ontario, Canada, health administrative data. Ontario is the largest province in Canada, with 14.3 million residents, all of whom have access to essential health care services without any direct costs to the individual. These health care services include primary and acute health care, obstetrical care, and mental health care provided by physicians. The study population for the current study included all women with a singleton live birth conceived between April 1, 2005 and March 31, 2015, who were 15–49 years of age at conception and delivered in an Ontario hospital. Women with mental illness diagnosed during pregnancy or in the 2 years before conception were excluded to capture new episodes of mental illness in the postpartum period. Women were followed for 365 days postpartum, to a maximum date of December 31, 2016.
Ethics approval
The use of data for this study was authorized under section 45 of Ontario's Personal Health Information Protection Act and does not require research ethics board review.
Data sources
The administrative data used for this study were housed at ICES, a publicly funded, not-for-profit research institute that links various administrative datasets using a unique encoded identifier. The MOMBABY dataset was used to identify singleton live births. MOMBABY links maternal and newborn records for all Ontario hospital births (>98% of all births). Chronic disease and mental illness were determined from outpatient physician visits, emergency department visits, and hospitalizations. Outpatient physician visit data were retrieved from the Ontario Health Insurance Plan (OHIP) database. Emergency department visit data were retrieved from the National Ambulatory Care Reporting System (NACRS). Hospitalization data were retrieved from the Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD). We also utilized the Ontario Mental Health Reporting System (OMHRS) for psychiatric hospitalizations. Sociodemographic characteristics were retrieved from the Registered Persons Database and linked Census data.
The OHIP database uses physician billing codes, and hospital databases use the Canadian Coding Standards for the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10; CIHI-DAD and NACRS) or Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV; OMHRS). The information in these datasets has been found to be valid, complete, and reliable. 20
Exposure
The exposed group comprised women with one or more of the following chronic diseases, identified using validated algorithms in the 2 years before conception: asthma, 21 cardiovascular disease, 22 –25 chronic hypertension, 26 chronic kidney disease, 27 chronic migraine, 28 chronic obstructive pulmonary disease, 29 diabetes, 30 epilepsy, 31 inflammatory bowel disease, 32 systemic lupus erythematosus, 33 multiple sclerosis, 34 psoriasis, 35 rheumatoid arthritis, 36 and thyroid disease 37 (Supplementary Table S1). The chronic diseases included in this study capture commonly-diagnosed chronic diseases that are most likely to have an impact on pregnancy-related health. 38 To determine the conception date of each pregnancy, the recorded gestational age was subtracted from the date of birth. Gestational age was generally based on the first trimester ultrasound. 39 The unexposed group was composed of women with none of these chronic diseases during this time period.
Outcome
Postpartum mental illness was the outcome of interest, diagnosed between the date of delivery and up to 365 days postnatally. The outcome was defined using a previously published method as one or more diagnoses of a mood or anxiety disorder, psychotic disorder, substance use disorder, self-harm, or other mental illness by a family physician or psychiatrist, or in an emergency department visit or hospitalization (Supplementary Table S2). 40
Covariates
The mediator of interest was a composite measure of perinatal complications and was dichotomized as present or absent in pregnancy or within 42 days after birth. Perinatal complications included pregnancy complications (i.e., preeclampsia/eclampsia, severe obstetric morbidity [placental abruption, placental infarction, obstetric embolism, septic shock, uterine rupture], or systemic maternal complications [acute renal failure, acute respiratory distress syndrome, cardiomyopathy, cerebrovascular diseases, disseminated intravascular coagulation, hepatic failure, pulmonary/cardiac/nervous complications of anesthesia, status epilepticus]), delivery complications (i.e., cesarean section or peripartum hemorrhage), and neonatal complications (i.e., preterm birth at <37 weeks gestation, small for gestational age at <10th percentile for gestational age based on sex-specific birthweight distributions, and congenital anomalies).
Potential confounders were based on the literature 41 and included maternal age, parity, neighborhood income quintile, material deprivation quintile, rurality, and remote history of mental illness. Maternal age was categorized into three groups: 15–24, 25–34, and 35–49 years. Parity was characterized as primiparous or multiparous. Neighborhood income quintile was based on the average single-person income equivalent in each dissemination area in Ontario from the 2011 Census. The material deprivation quintile was derived from the Ontario Marginalization Index (ON-MARG), based on the following six indicators that examine proportions of the population that: (1) are aged 20 years or older without a high school diploma, (2) are lone parent families, (3) receive income from government transfer payments, (4) are unemployed, (5) are low income, and (6) are households living in dwellings requiring major repairs. 42 A rural community was defined as a community with <10,000 residents. Remote history of mental health care was defined as a mental illness diagnosis in ≥1 physician visits, emergency department visits, or hospitalizations more than 2 years before conception.
Statistical analyses
Percentages and frequencies were calculated for descriptive analyses. Standardized differences were used to assess differences across exposure groups. 43 Based on the Baron and Kenny method for examining mediation, 44 three regression models were conducted first to test for the association between: (1) chronic disease and postpartum mental illness, (2) chronic disease and perinatal complications, and (3) perinatal complications and postpartum mental illness. These models were built using modified Poisson regression. An advantage of modified Poisson regression over logistic regression is its ability to directly calculate robust relative risks (RRs) and their corresponding 95% CIs in the presence of common outcomes. 45 All models controlled for the confounders defined above.
To test mediation, a method which applies generalized estimating equations (GEE) to the modified Poisson model was then used to test the statistical significance of the indirect effect of chronic disease on postpartum mental illness risk, via perinatal complications. 46 Using this method, the total effect represented the association between chronic disease and postpartum mental illness, not adjusting for perinatal complications. The direct effect represented the association between chronic disease and postpartum mental illness, adjusting for perinatal complications. The difference in the coefficients between these two models represented the indirect effect of chronic disease on postpartum mental illness, via perinatal complications.
Additional analyses were performed to study the mediating effects of pregnancy, delivery, and neonatal complications separately and the mediating effect of perinatal complications on the association between individual chronic disease diagnoses and postpartum mental illness. We also repeated the mediation analysis after excluding women with a remote history of mental health care from the cohort, since prior psychiatric history is a major risk factor for postpartum mental illness 47 and therefore a strong confounder in these analyses.
All analyses were conducted in SAS 9.4 (Cary, NC).
Results
There were a total of 792,972 women included in the study, of whom 21.1% had a chronic disease (with this high rate driven by an asthma prevalence of 13.7%) (Supplementary Table S1). Women with a chronic disease were more likely to be aged 15–24 years (19.6% vs. 15.8%) and have a remote history of mental health care (57.3% vs. 44.2%) than unexposed women (Table 1). No other population characteristic had a standardized difference >0.10.
Baseline Characteristics of Women With and Without Chronic Disease
Standardized differences >0.10 are considered clinically different.
Remote history of mental illnesses included mood or anxiety disorders, psychotic disorders, substance use disorder, self-harm, and other mental illness diagnosed more than 2 years before conception.
About 13.0% of women with a chronic disease, compared to 9.7% of women without a chronic disease, were diagnosed with a postpartum mental illness, corresponding to an adjusted relative risk (aRR) of 1.15 (95% CI: 1.14–1.16). Of women with a chronic disease, ∼45.5% had a perinatal complication (i.e., 0.3% had pregnancy complications, 32.2% had delivery complications, and 20.3% had neonatal complications), compared to 42.2% of women without a chronic disease, corresponding to an aRR of 1.08 (95% CI: 1.07–1.09) (Table 2). In addition, 10.9% of women with perinatal complications, compared to 10.0% of women without perinatal complications, had postpartum mental illness, corresponding to an aRR of 1.09 (95% CI 1.08–1.11).
Unadjusted and Adjusted Relative Risks of the Associations Between the Exposure and Outcome (Chronic Disease and Postpartum Mental Illness), Exposure and Mediator (Chronic Disease and Perinatal Complications), and Mediator and Outcome (Perinatal Complications and Postpartum Mental Illness)
Models adjusted for age, parity, neighborhood income quintile, material deprivation index, rurality, and remote history of mental health care.
CI, confidence interval; RR, relative risk.
In mediation analyses, perinatal complications explained only 1.5% of the association between chronic disease and postpartum mental illness, corresponding to an indirect aRR of 1.003 (95% CI 1.002–1.003) (Table 3). The mediating effect of pregnancy, delivery, and neonatal complications individually was also small, with only 0.15%, 1.5%, and 0.5% of the association explained by the respective type of perinatal complication (Figure 1). Approximately 27.0% of women underwent a cesarean section, but excluding them from the perinatal complication definitions yielded no difference in results (data not shown).
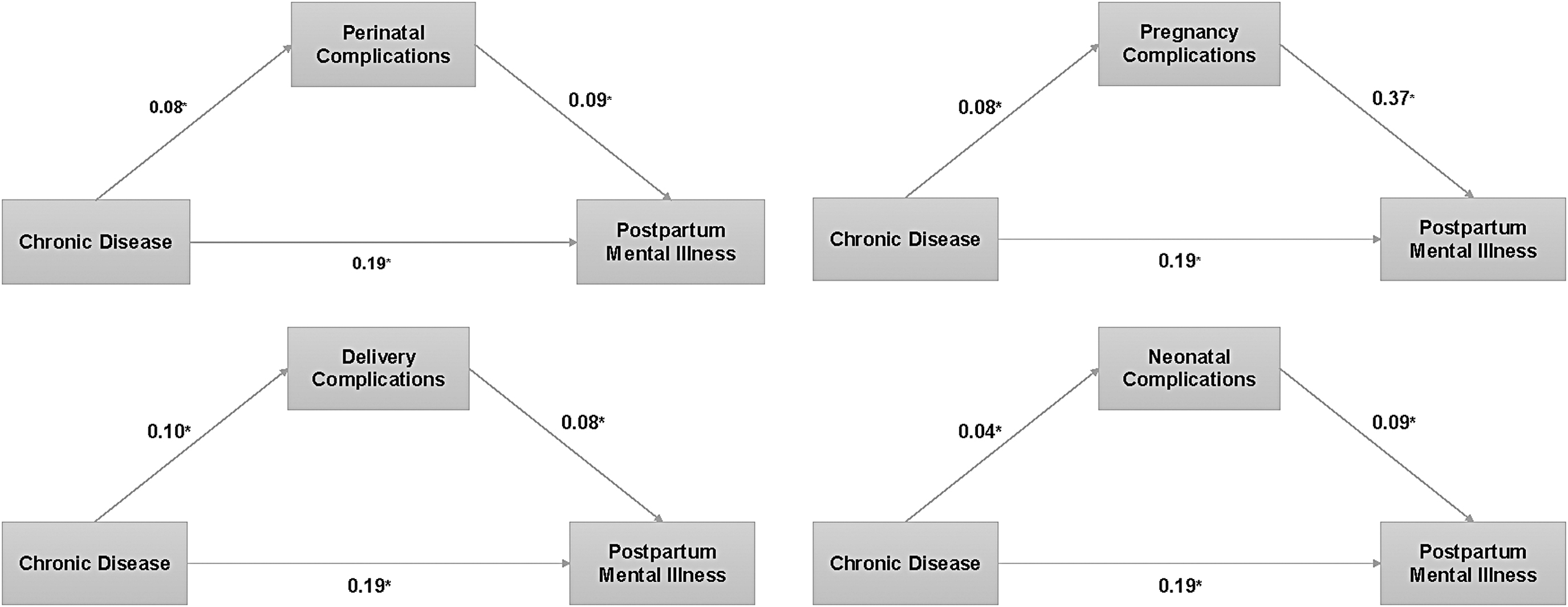
Direct and indirect pathways of the association between chronic disease and postpartum mental illness and their associated beta coefficients. Starred coefficients are statistically significant.
Mediating Effect of Perinatal Complications on the Association Between Chronic Disease and Postpartum Mental Illness
Models adjusted for age, parity, neighborhood income quintile, material deprivation index, rurality, and remote history of mental health care.
Additional analyses examined the mediating effect of perinatal complications for individual chronic disease diagnoses (Supplementary Table S3). Perinatal complications explained 7.1% of the association between chronic hypertension and postpartum mental illness and 14.2% of the association between type 1 or type 2 diabetes and postpartum mental illness; however, the indirect aRRs still approximated 1.00. No associations between cardiovascular disease, inflammatory bowel disease, kidney disease, or lupus and postpartum mental illness were observed; therefore, we did not examine mediation for these diagnoses.
When we repeated the mediation analysis after excluding women with a remote history of mental health care from the cohort, we found that perinatal complications still explained only 1.5% of the association between chronic disease and postpartum mental illness (Supplementary Table S4).
Discussion
This population-based study examined the mediating role of perinatal complications in the association between chronic disease and postpartum mental illness. While there was elevated risk of postpartum mental illness with both chronic disease and perinatal complications, perinatal complications did not mediate the relationship between chronic disease and postpartum mental illness. Similar results were observed when examining pregnancy, delivery, and neonatal complications and chronic disease diagnoses separately. Our study suggests that alternative mechanisms explain the increase in postpartum mental illness with chronic disease.
Our findings with respect to an increased risk of postpartum mental illness with chronic disease are in line with previous studies, 8,41,48 –51 with a prior meta-analysis reporting a pooled adjusted OR of 1.44 (95% CI 1.13–1.85). 8 Similarly, previous studies reported on an increased risk of perinatal complications related to chronic diseases 5 –7,52 –55 and an increased risk of postpartum mental illness related to perinatal complications. 15 –19,56 –58 Although we report positive associations between the exposure, mediator, and outcome, perinatal complications did not explain the increased risk of postpartum mental illness with exposure to chronic disease in this study, even after exclusion of women with any previous history of mental illness. This could be due to the small RRs we observed, particularly between exposure and mediator and mediator and outcome. We did observe some evidence of heterogeneity in our analyses examining the mediating effects of perinatal complications with individual chronic disease diagnoses. Perinatal complications appeared to be one possible pathway linking type 1 or type 2 diabetes and chronic hypertension with postpartum mental illness, but the indirect effects were still very small, and these results could have been a spurious finding due to multiple testing.
Our findings may indicate that chronic disease influences the risk of postpartum mental illness via other direct or indirect pathways. For example, evidence suggests that an inflammatory pathway may explain the relationship between asthma, depression, and anxiety 59 ; immunological changes could explain the relationship between cardiovascular disease and depression 60 ; and insulin resistance could explain the relationship between depression and type 2 diabetes. 61 Stress has also been associated with higher rates of chronic diseases, as well as mental illness, likely via neuroinflammatory responses. 62 –65 Administrative data do not capture stress-related factors effectively, but we recommend future study of alternative indirect pathways linking chronic disease to postpartum mental illness.
Strengths of this study include our use of population-based data, large sample size, and measurement of multiple chronic diseases and perinatal complications. We used administrative data; therefore, the definitions of chronic disease, perinatal complications, and mental illness were based on health care encounter data. Although we used validated algorithms for disease identification where possible, these may be subject to misclassification bias. We captured the most common chronic conditions experienced by women of childbearing age 1,2 ; while some conditions such as cancer were not captured, such conditions are likely not sufficiently common to impact results. Furthermore, our mental illness definition only captured diagnoses recorded in physician visits, emergency department visits, and hospitalizations and excluded visits with private providers such as psychologists and other types of therapists. We did not test the associations by type of mental illness nor could we tease apart the details of some of the perinatal complications such as emergency versus scheduled cesarean deliveries. These explorations could be an area for future research. Furthermore, we were only able to control for socioeconomic status using neighborhood-level data, and we had no information on other potentially important covariates such as relationship status, availability of caregivers for the infant other than the mother, and other sources of social and emotional support. This study excluded women with a recent history of mental illness to capture new episodes of mental illness in the postpartum period in relation to perinatal complications, which may exclude women more vulnerable to postpartum mental illness. Finally, our additional analyses may be subject to multiple testing errors, and our results should be interpreted with caution.
We observed an increased risk of postpartum mental illness in the presence of chronic disease. Notably, we observed a high prevalence of chronic diseases among younger women driven by a high prevalence of asthma. As asthma rates, and those of other chronic diseases, continue to rise, 66 it will be increasingly important to identify pregnant women with chronic diseases at risk of perinatal mental illness. Although it is difficult to predict who would develop a mental illness after pregnancy, preventative psychotherapeutic interventions have been shown to be effective in reducing postpartum mental illness incidence and symptomology in high-risk women. 67 Our results provide further evidence that women with chronic disease are also high risk and could benefit from such preventative strategies. As such, mental health support could be provided to these women to ensure that their risks for postpartum mental illness are minimized.
Contrary to our hypothesis, perinatal complications did not mediate the association between chronic disease and postpartum mental illness in this study. This could be a reassuring finding. Many perinatal complications are difficult to prevent, and if they are not responsible for the increased risk of postpartum mental illness in women with chronic disease, this could indicate that preventative measures aimed at chronic disease management and mental health will be effective. Future studies should explore alternative etiologies that link chronic disease to perinatal health, such as the mediating effect of stress.
Conclusion
Results from this study show no meaningful mediation by perinatal complications in the association between chronic disease and postpartum mental illness. Our results suggest that alternative mediators may be underlying this association.
Footnotes
Authors' Contributions
A.M.A. helped conceive the idea, conducted all analyses, and wrote the article. H.K.B. conceived the idea, supervised the project, and reviewed the article. S.N.V. and C.-L.D. reviewed the article and provided input on result interpretations.
Acknowledgments
Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are those of the author and not necessarily those of CIHI.
Author Disclosure Statement
S.N.V. receives royalties for authorship of materials related to depression and pregnancy from UpToDate, Inc. All other authors have no conflicts of interest.
Funding Information
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study also received funding from: Canadian Institutes of Health Research (Grant No. 376290 to H.K.B.). The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding; no endorsement is intended or should be inferred. The funding agency had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; or decision to submit the article for publication. This research was undertaken, in part, thanks to funding from the Canada Research Chairs Program to H.K.B.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.