
Abstract
Background:
Gender differences have been described in many fields of pain. However, research is inconclusive as to gender difference in pain management. Our study aimed to investigate gender differences in prescribing analgesics for low back pain.
Methods:
We designed a cross-sectional study based on data originated from computerized health records. We retrieved data on low back pain diagnosis, among patients aged 18–64 years during 2016. Visits due to trauma and fracture were excluded, as were visits of patients with known neoplasm, or neurological or congenital defects. Data included demographics and the analgesics prescribed.
Results:
The cohort comprised 45,479 patients; of them, 55% were women. The mean age was 42.9 ± 12.6 years. Analgesics were prescribed to 49% of the men and 47% of the women (odds ratio [OR] 1.07, 95% confidence interval [CI] 1.03–1.11). The distribution of analgesics was similar between the genders: overall, 73% nonsteroidal anti-inflammatory drugs, 23% opioids, 4% other analgesics, mainly paracetamol and dipyrone. A higher proportion of men were prescribed strong opioids than women: 17% versus 8% (OR 2.36, 95% CI 2.03–2.75).
Conclusion:
Men and women were similarly prescribed analgesics for low back pain. Men were more likely than women to be prescribed strong opioids. Further research is needed to evaluate the outcomes of this differential treatment.
Introduction
Gender differences have been described in many fields of pain. Many chronic pain syndromes are more prevalent among women. 1 –3 Moreover, pain perception is reportedly enhanced in women. 4,5 In an experimental setting, women compared with men who received pain stimulus (mainly to the skin) were found to have lower pain thresholds, higher ratings of pain, and less tolerance of stimuli. 2 Women reported higher levels of chronic pain in tertiary care than did men. 3 Women with pain were reported to seek medical services more frequently than men. 2 These findings are only partially explained by biological (sex) and psychosocial (gender) differences. 6
Awareness has grown to gender differences in the pain experience. 4 This has triggered a growing body of research regarding pain and gender. However, evidence regarding gender and analgesics for pain treatment remains sparse. Analgesic effectiveness has mostly been investigated in research on men. 7
Opioids constitute one of the main pharmacological treatments for pain. The available evidence is inconclusive as to the effectiveness of opioid analgesic by gender. In rodents, opioid analgesia was more effective and more potent in males. 8 In humans, one study reported greater opioid analgesia in women, yet another publication concluded that opioid analgesia was greater among women in experimental but not in clinical studies. 9 The authors of the latter called for caution in extrapolating from an experimental setup to clinical encounters.
Another study compared responses to opioids in women and men, both in analgesic effectiveness and in adverse effects, based on the rapidity of their metabolism. Among normal metabolizers (50% of the cohort), women reported twofold more adverse effects of opioids than men. 10 This finding could explain reports of lower doses of opioids self-administrated by women 9 as an attempt to avoid adverse effects, and not as a consequence of higher effectiveness, as was previously thought. The question of opioid effectiveness by gender thus remains unresolved. Differences in analgesic effectiveness themselves constitute a factor that affects not only the alleviation of present pain, but also the risk of developing chronic pain and disability. 11
Studies that have investigated gender differences in opioid prescribing have shown discrepant results. A few studies 12,13 in primary care settings have compared opioid prescribing between men and women, without specifying the indications for prescription. One of these showed that men were more likely to receive opioids 12 ; whereas another showed that women were more likely. 13 Among low-income populations, a greater proportion of women than men received an opioid prescription: 13.1% versus 10.9%. 14 Another setting for researching gender differences in opioid prescribing is the emergency room (ER). In that setting, differences were not found in analgesic or opioid prescribing between men and women, including low-intensity and high-intensity opioid prescribing. 15,16 The question arises as to whether physicians prescribe different treatment regimens according to patient gender in primary care.
We chose the area of back pain since it is commonly encountered in primary practice. Back pain was reported to be the third leading cause for prescribing opioids for pain management in the United States. 17 Clinical guidelines for analgesic treatment of low back pain, 18,19 including current Israeli guidelines, 20 do not differentiate between genders.
Our research aimed to explore analgesic prescribing by family physicians for acute low back pain according to gender. Our research is of clinical value given the high burden of low back pain. It is also valuable for policy making, especially with current concerns of excess opioid prescribing and underutilization of nonopioid pain management strategies.
Methods
Study setup
National health insurance is compulsory for all Israeli residents. 21 Residents have family physicians according to their affiliation with one of the four health care providers. Visits with family physicians are at no cost, and at any frequency. Medications are significantly subsidized. Clalit Health Services (CHS) is the largest health care provider in Israel, and provides services to more than 70% of the residents in Israel's northern region. 22 The salaries of the CHS family physicians are not affected by patient visits or prescribing medications. CHS operates an electronic medical and administrative file, based on the International Classification of Diseases, 9th Revision (ICD-9). Patient files can be accessed from the central register.
Study design
In a cross-sectional study, we examined visits with family physicians, of patients aged 18–64 years who consulted regarding acute low back pain, during the year 2016, in the northern region of CHS. We included visits with ICD-9 codes 7242–7245 and L02–L03, such as “Low back pain,” “Sciatica,” “Low back pain with radiation symptoms,” “Low back pain without radiation,” “Lumbago,” “Lumbosacral radiculitis,” and “Pain lumbar region.” We assumed that these diagnoses reflect physicians' working hypotheses for further management. An acute episode of low back pain was confirmed by its recording on a first visit, with no similar diagnosis in the previous 3 months, thereby excluding chronic low back pain.
We excluded low back pain that was due to trauma, neoplasm, a congenital condition, or a neurological defect.
Data
Patient demographic data included age, gender, ethnic origin, marital status, national security support, and pregnancy in the year of the study. For each visit, we recorded the pharmacological group of analgesics prescribed. Pharmacological groups of analgesics comprised nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, and others—mainly paracetamol and dipyrone. Opioids were categorized by strength as weak (including tramadol, codeine, and buprenorphine) and strong (including fentanyl, morphine, oxycodone, and pethidine). 23 Regarding buprenorphine, we included only the transdermal product (trade name Butrans), which is prescribed solely for pain relief. Information about medication prescribing was extracted from structured fields in the medical records.
The research protocol was approved by the institutional review board of CHS. The data were analyzed using SAS version 9.4 (SAS Institute, Cary, NC). p < 0.05 was considered significant. Categorical data were reported as numbers (%) and associations with gender were performed using the chi-square test. Age was reported as means ± standard deviation and comparisons between gender were performed using the t-test.
Results
Characteristics of the study cohort
The cohort comprised 45,479 patients, who visited a primary clinic due to low back pain in the year 2016. Patient characteristics are described in Table 1. The mean age was 42.9 ± 12.6 years; 55% of the patients were women, 53% were Jewish, and 67% were married. Sociodemographic parameters, including age, sector, marital status, and national security support, were similar between men and women.
Characteristics of the Study Sample by Sociodemographic Parameters
SD, standard deviation.
Analgesic prescriptions according to patient gender
Analgesics were prescribed to 48% of all the patients with an acute episode of low back pain. Among men, 49% were prescribed analgesics, and among women, 47% were prescribed analgesics; the odds ratio (OR) for men versus women was 1.07 (95% confidence interval [CI] 1.03–1.11, p-value 0.0007). Of those prescribed analgesics, 72% were prescribed a single analgesic, whereas 28% were prescribed more than one analgesic. Men and women were equally likely to receive more than one analgesic (men 28%, women 29%, OR men vs. women 0.97, 95% CI 0.91–1.02, p-value 0.2397).
The most frequently prescribed analgesics by the pharmacological group were NSAIDs (73%), followed by opioids (23%). The remaining 4% of analgesics comprised mainly prescribed over-the-counter analgesics such as paracetamol and dipyrone.
The distributions of analgesic prescriptions by the pharmacological group were similar in men and women (Fig. 1). This similarity remained in an analysis that excluded pregnant women (Supplementary Fig. S1).

Distribution of analgesics prescribed to the study sample by gender and pharmacological group.
Of the prescribed analgesics, 19% were of fixed dose combinations, which included mainly opioids with paracetamol. Men were prescribed fixed dose combinations less frequently than women: 17% versus 20% (OR men vs. women 0.81, 95% CI 0.76–0.86, p-value <0.0001). This difference remained unchanged in an analysis that excluded pregnant women.
The distribution of opioid prescriptions by strength differed significantly between male and female patients (Fig. 2). Men were prescribed stronger opioids than women; 17% of men were prescribed strong opioids, compared with 8% of women (OR men vs. women 2.36, 95% CI 2.03–2.75, p-value <0.0001). Excluding pregnant women did not change the results significantly: 17% of men and 8% women were prescribed strong opioids, OR men versus women 2.38, 95% CI 2.04–2.77, p-value <0.0001.
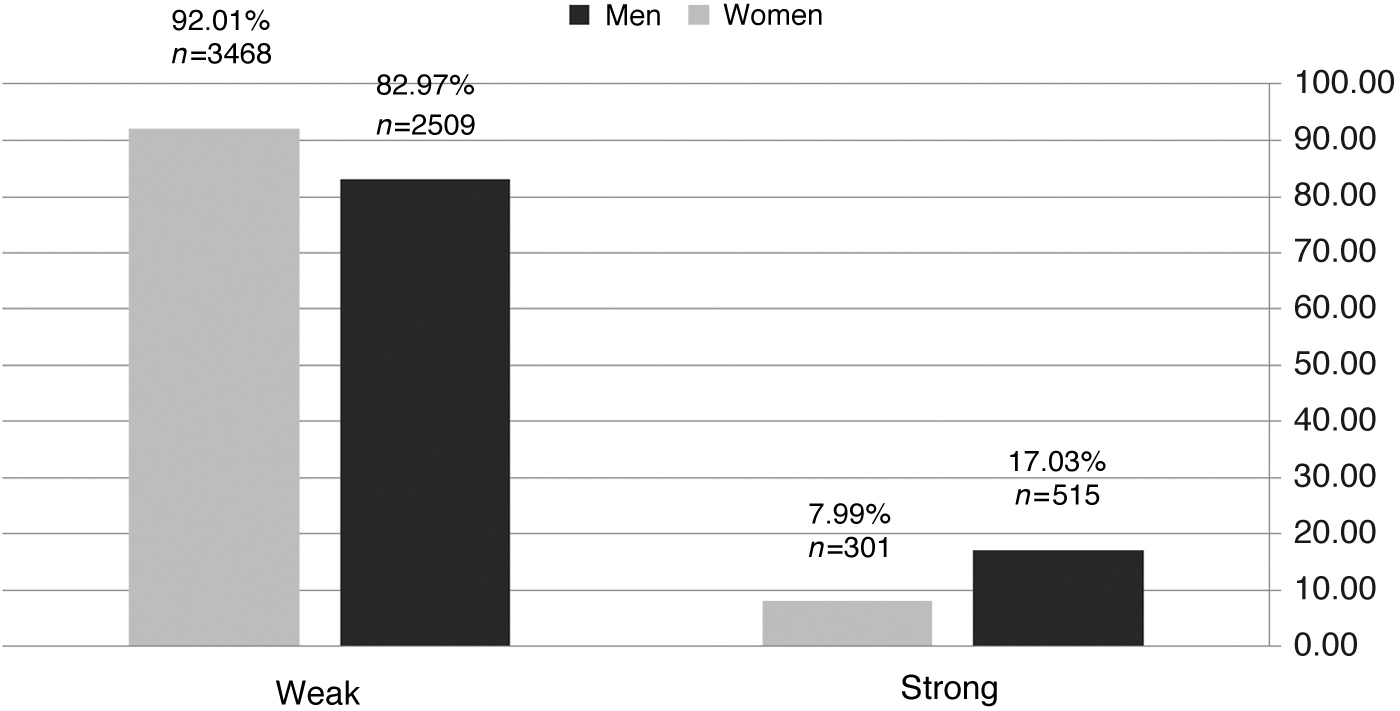
Distribution between genders of opioid prescriptions by strength. Men were prescribed strong opioids more frequently than women (p-value <0.0001).
Discussion
About half the patients in our cohort with complaints of acute low back pain were prescribed analgesics. Men and women were similarly prescribed analgesics, and no difference was found between men and women in the pharmacological groups of analgesics prescribed. A difference was observed in the prescriptions for opioids; stronger opioids were prescribed more frequently for men than for women.
Overall, for the year 2016, we report opioid prescribing to 15% of patients with low back pain at their first visit with this complaint. Of these, 12% were prescribed strong opioids. This is substantially lower than U.S. data for opioid prescription for this indication in the immediately preceding years: 27% in 2015, decreased from 35% in 2008. 24
Notably, the 2007 guidelines for treatment of acute low back pain of the American College of Physicians and the American Pain Society, which Israeli physicians are exposed to, recommended prescribing opioids for uncontrolled acute low back pain, or for back pain that seemed unlikely to be controlled with NSAIDs or with paracetamol. 25 However, Israeli guidelines from 2007 excluded opioids for this indication, and recommended paracetamol as first-line treatment, and NSAIDs as second-line treatment. 20 Our finding therefore exceeds recommended prescribing of opioids according to Israeli guidelines. In guidelines issued in 2017 by the American College of Physicians, and endorsed by the American Academy of Family Physicians, pharmacological treatment of acute low back pain was reduced considerably, and opioids were excluded from medications for acute low back pain. This was due to insufficient evidence for their effectiveness. 19 In a meta-analysis of studies from various countries, which reported opioid prescribing for adults with chronic noncancer pain, opioid prescribing rates were reported to be as high as 30.7%. Strong opioids were prescribed to 18.5% of the patients with chronic pain. Opioids for chronic low back pain were prescribed to 41.5% of the patients. 26 These prescription rates are considerably higher than those in our study. Notably, that meta-analysis included studies conducted in the primary care setting but also studies conducted in the hospital setting and pain clinics, both of which differ from primary care.
We found differential prescribing of stronger opioids according to gender. No clinical guidelines differentiate between men and women in analgesic treatment of low back pain. 18 –20 Thus, our research confirms differences between men and women in pain treatment, in a field in which no differences were to be expected, according to guidelines. Women have been documented to experience and report higher levels of clinical pain than men. 2,3 Therefore, differences in pain perception do not explain the lower prescribing of opioids for women.
Research studies on the association between analgesic prescribing and gender have shown mixed results. In some studies that were based on medical vignettes, physicians did not differ in their responses regarding prescriptions of analgesics for acute back pain to male and female patients. 8,9 This contrasts with gender differences that have been shown in vignette studies of analgesic prescribing of other clinical conditions (cervicalgia and renal colic). 27 –29
Studies performed in ER settings in the United States and Canada did not find differences in the prescribing of analgesics for male and female patients. 15,16 ER settings differ in a number of ways from community-based settings, including patient characteristics; pain level; pain mechanisms, specifically trauma-related pain; and in-built protocols for pain treatment. All these may result in differences between prescribing in the ER and in the primary care setting.
The novelty of our study is its description of real-world encounter outcomes, rather than hypothetical vignettes, and that it specified the strength of opioids prescribed. Strengths of our study include its large scale and its reflection of a diverse ambulatory patient population. Various ethnic groups were included. In addition, it was performed in a public health setting in which primary care visits are paid for by national insurance, and medications are subsidized.
Opioid prescribing policies have become more relevant in face of prescription opioid-related harms. According to U.S. CDC reports, opioid abuse has increased among both men and women over recent years, and the increase has been sharper among women than among men. 30 In a study that examined patient gender and the abuse of prescription opioids, 31 men were more likely than women to report abuse of stronger opioids, whereas women were more likely to report abuse of weaker opioids.
There are some limitations to our study. We found that only 48% of patients with complaints of lower back pain were prescribed analgesics in a primary care setting. This is a low percentage when considering current guidelines. One limitation of our research is the lack of data regarding nonprescribed over-the-counter analgesics such as paracetamol, dipyrone, and ibuprofen. Our findings apply only to prescription medications. Other limitations of our study are the lack of information regarding physician characteristics, pain severity, and outcomes of treatment. While addressing the topic of prescribing analgesics by gender, future research might better describe physicians' attitudes toward low back pain in men and women. Further research is also needed to evaluate the effect of analgesic prescribing on the course of disease and on opioid addiction in men and women, and thus to determine the appropriateness of choice of opioid.
Conclusion
In our study, the likelihood of prescribing analgesic treatment for low back pain was similar in men and women. No gender difference was found in the choice of pharmacological group. However, differences were found in the selection of strength of opioid, with men prescribed stronger opioids than women.
Footnotes
Acknowledgments
We thank Shiraz Vered for statistical analysis. We thank Hilla Kfir for her work as research assistant.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.