
Abstract
Background:
Many women with endometriosis experience chronic abdominal pain. Clinical guidelines recommend treatment with analgesics, contraceptive hormones, gonadotropin-releasing hormone analogs, and surgery. Treatment patterns in women with endometriosis are not well characterized.
Methods:
Data from the IBM® MarketScan® Commercial Database were accessed from 2009 to 2017. One-year baseline and follow-up periods were defined around the date of the first claim with a diagnosis of endometriosis (the index date). Women 18–49 years of age on the index date with a diagnosis of endometriosis, continuous enrollment during baseline and follow-up, and pharmacy benefits were included. The following outcomes were analyzed descriptively: baseline comorbidities; medication use and surgeries; and sequence of treatment utilization in the baseline and the follow-up period.
Results:
A total of 190,921 women were included. The mean ± (standard deviation) age was 39.0 ± (7.3), and abdominal/pelvic pain (36.0%) and excessive or frequent menstruation (32.0%) were the most prevalent comorbidities. In the baseline period, the utilization of pharmacological treatment was: estrogen/progestin 42.5%, opioids 41.5%, and nonsteroidal anti-inflammatory drugs (NSAIDs) 37.5%. In the follow-up period, utilization of opioids and NSAIDs increased to 68.9% and 51.1%, respectively, whereas the use of estrogen/progestin dropped to 23.8%. Surgeries were infrequent in the baseline period (6.3%). However, in the follow-up period, 27.9% of women underwent laparoscopy and 29.7% had a hysterectomy, with a total of 68.1% of the study population undergoing surgical treatment.
Conclusions:
A diagnosis of endometriosis is accompanied by an increase in the use of analgesics and surgical procedures. The diversity of treatments suggests a lack of clarity in management guidelines.
Introduction
Endometriosis is a chronic disease of uncertain pathogenesis defined by the presence of endometrial glands and stroma outside the uterus. 1 It commonly manifests as abdominopelvic pain and sometimes infertility. 2 A histologically confirmed diagnosis requires surgery, leading to years-long delays in diagnosis and underestimates of prevalence. 3,4 The commonly cited estimate of global prevalence is 10% among women of reproductive age. 5 A recent survey of over 50,000 women from the United States corroborates that estimate with a reported prevalence of 6.1% among women 18–49 years of age. 6
Women with endometriosis experience symptoms such as dysmenorrhea (pain with menstruation), dyspareunia (pain with sexual intercourse), and chronic abdominal pain unrelated to menstruation at a higher rate than women without endometriosis. 6,7 Clinical guidelines recommend treatment of endometriosis-related pain with analgesics, contraceptive hormones, gonadotropin-releasing hormone (GnRH) analogs, aromatase inhibitors, and, in instances of a histological/surgical diagnosis, with ablative or excisional surgery. 8 The success of these treatment strategies is variable, with limited clinical trial evidence to support the recommendations. 8,9
The burden of endometriosis and its treatment has been characterized in terms of health care resource use, 10 –14 health economics, 10,12,13,15,16 quality of life, 17 –20 and work productivity. 17,20 However, treatment patterns in women with endometriosis are not well described. The objective of this study was to characterize pharmacological and surgical treatment patterns in U.S. women newly diagnosed with endometriosis in clinical practice.
Methods
Study design and data source
This was a retrospective, observational cohort study of administrative claims from the IBM® MarketScan® Commercial Database, which includes data from more than 100 large employers and 12 unique health plans across the United States. The MarketScan® Commercial Database comprises medical and drug claims for ∼60 million unique individuals, as well as their spouses and dependents, who are covered by employer-sponsored private health insurance under a variety of fee-for-service, fully capitated, and partially capitated health plans. The claims are derived from inpatient, outpatient, and pharmacy services. Research using deidentified MarketScan® data is fully compliant with U.S. privacy laws and regulations, obviating the requirement for informed consent or Institutional Review Board approval under the U.S. Food & Drug Administration's Common Rule. 21
Data from the MarketScan® Commercial Database were accessed during a study period of January 1, 2009 to December 31, 2017. The index date was defined as the date of the first claim with a diagnosis of endometriosis during the study period, leaving room for a baseline period of 12 months before, and a follow-up period of 12 months after the index date. A separate sensitivity cohort was created by extending the baseline and follow-up periods to 3 years in an attempt to capture patients' longer endometriosis journey.
Study population
Women 18–49 years of age with (1) a claim, including a diagnosis of endometriosis, (2) continuous health plan coverage for 12 months before (baseline) and 12 months after (follow-up) the index date, and (3) pharmacy benefits were included in the analysis. Endometriosis was identified by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code 617.x, and ICD-10-CM code N80.x. Women in the sensitivity cohort were required to have at least two claims with a diagnosis of endometriosis on separate dates any time during the study period, as well as continuous coverage for 3 years before and after the index date. Exclusion criteria for both cohorts included a diagnosis of endometriosis or a diagnosis of a malignant neoplasm of the female genitourinary organs or a radical hysterectomy during the baseline period.
Study outcomes
Baseline characteristics, including age, urbanicity, geographic region (U.S. Census divisions), health plan type, and relevant comorbidities were measured on the index date and in the baseline period. Comorbidities were identified by ICD-9 and ICD-10 codes (Supplementary Table S1).
Pharmacological treatments that are commonly prescribed to help with endometriosis-related pain were classified as estrogen/progestin (including danazol, depot medroxyprogesterone, oral medroxyprogesterone acetate, levonorgestrel implants and intrauterine devices, megestrol acetate, and progestin-only, or other oral contraceptive pills), nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, and GnRH analogs (including leuprolide, histrelin, goserelin, nafarelin, triptorelin, ganirelix, degarelix, cetrorelix, and abarelix). Pharmacological agents were identified by National Drug Codes, as well as diagnosis and procedure codes (list available upon request).
Surgical treatments included laparoscopy (in which a surgeon accesses the abdomen and pelvis through small incisions in the skin), laparotomy (which involves a large incision through the abdominal wall to gain access into the abdominal cavity), other excision/ablation (uses heat to destroy abnormal cells where they reside), hysterectomy (removal of the uterus), and oophorectomy (removal of one or both ovaries). The first three were considered minor surgeries, and the last two as major surgeries. Surgeries were identified using procedure codes (list available upon request).
To look for treatment patterns across the endometriosis treatment journey, we assessed the sequence of treatments (among the above lists of included treatments) used by each patient, starting with the first treatment observed in each period (baseline and follow-up). If the first record of two or more distinct treatments occurred on the same date, the treatment order was assigned as follows: NSAIDs, opioids, estrogen/progestin, GnRH analogs, minor surgeries, and major surgeries.
To assess the possibility of use of NSAIDs and opioids for treatment of postoperative pain instead of for endometriosis-related pain, a “surgery window” was defined as the 30 days before and after the surgery date. For subjects with multiple surgery dates, only the first surgery was assessed.
Statistical analyses
All analyses were descriptive and no statistical tests were performed. All results are presented as numbers and/or percentages.
Results
Study population
A total of 190,921 women met the inclusion criteria (Fig. 1). The mean ± (standard deviation) age was 39.0 ± (7.3), with a median age of 40.0 years. Most women (83.0%) were from urban areas (Table 1). Abdominal/pelvic pain was the most frequent comorbidity in the baseline period (36.0%; Table 2). Excessive or frequent menstruation (32.0%) and dysmenorrhea (18.7%) were prevalent, as well as ovarian cysts (24.2%), uterine fibroids (21.6%), and unspecified symptoms of female genital organs (25.6%).

Patient flowchart.
Baseline Demographic Characteristics
Values are presented as n (%).
Patients with continuous enrollment for 3 years both pre- and post-index and with at least two diagnoses of endometriosis in the baseline period.
CDHP, consumer-driven health plan; EPO, exclusive provider organization; HDHP, high-deductible health plan; HMO, health maintenance organization; POS, point of service; PPO, preferred provider organization.
Baseline Comorbidities and Symptoms
Values are presented as n (%).
The following comorbidities/symptoms occurred in <1% of both cohorts: acute coronary syndrome, bladder pain, heart failure, and osteoporosis.
Patients with continuous enrollment for 3 years both pre- and post-index and with at least two diagnoses of endometriosis in the baseline period.
COPD, chronic obstructive pulmonary disease.
The sensitivity cohort (N = 24,010) was similar to the main cohort in terms of sociodemographic parameters (Table 1) and comorbidities (Table 2), with a few notable differences: greater prevalence of abdominal/pelvic pain (52.3%) and unspecified symptoms of female genital organs (44.2%), as well as vaginitis (19.6%) and upper respiratory infection (34.2%; Table 2).
Pharmacological treatment patterns
In the baseline period of the main cohort (Table 3), the utilization of pharmacological treatment was: estrogen/progestin 42.5%, opioids 41.5%, and NSAIDs 37.5%. GnRH analog use was low (4.3%), and 28.2% of patients were not receiving any of the drugs included in this analysis. In the follow-up period, rates of opioid and NSAID use increased to 68.9% and 51.1%, respectively, whereas use of estrogen/progestin dropped to 23.8% and GnRH use (4.9%) stayed about the same. Similar patterns were observed in the sensitivity cohort (Table 3), where opioid and NSAID use increased from baseline to follow-up; estrogen/progestin use stayed about the same, and GnRH analog use increased.
The Use of Pharmacological Agents and Surgical Treatment
Values presented as n (%), in descending order for the baseline period of the main cohort. Surgery categories are mutually exclusive, but medication categories are not.
Baseline and follow-up periods are 1 year pre- and post-index, respectively.
Baseline and follow-up periods are 3 years pre- and post-index, respectively.
GnRH, gonadotropin-releasing hormone; NSAID, nonsteroidal anti-inflammatory drug.
Surgical treatment patterns
Surgeries were infrequent in the baseline period of the main cohort (6.4% of the study population; Fig. 2), with laparoscopy being the most common (2.5%; Table 3). However, in the follow-up period, 27.9% of women underwent laparoscopy and 29.7% had a hysterectomy (Table 3). Most post-index surgeries occurred within 1 month of diagnosis (59.1% of the population), with a total of 68.1% of the study population undergoing surgical treatment by the end of the follow-up year (Fig. 2). Similar trends were observed in the sensitivity cohort (Table 3), with 79.9% of these patients undergoing surgery within 3 years after the diagnosis date (Fig. 2).
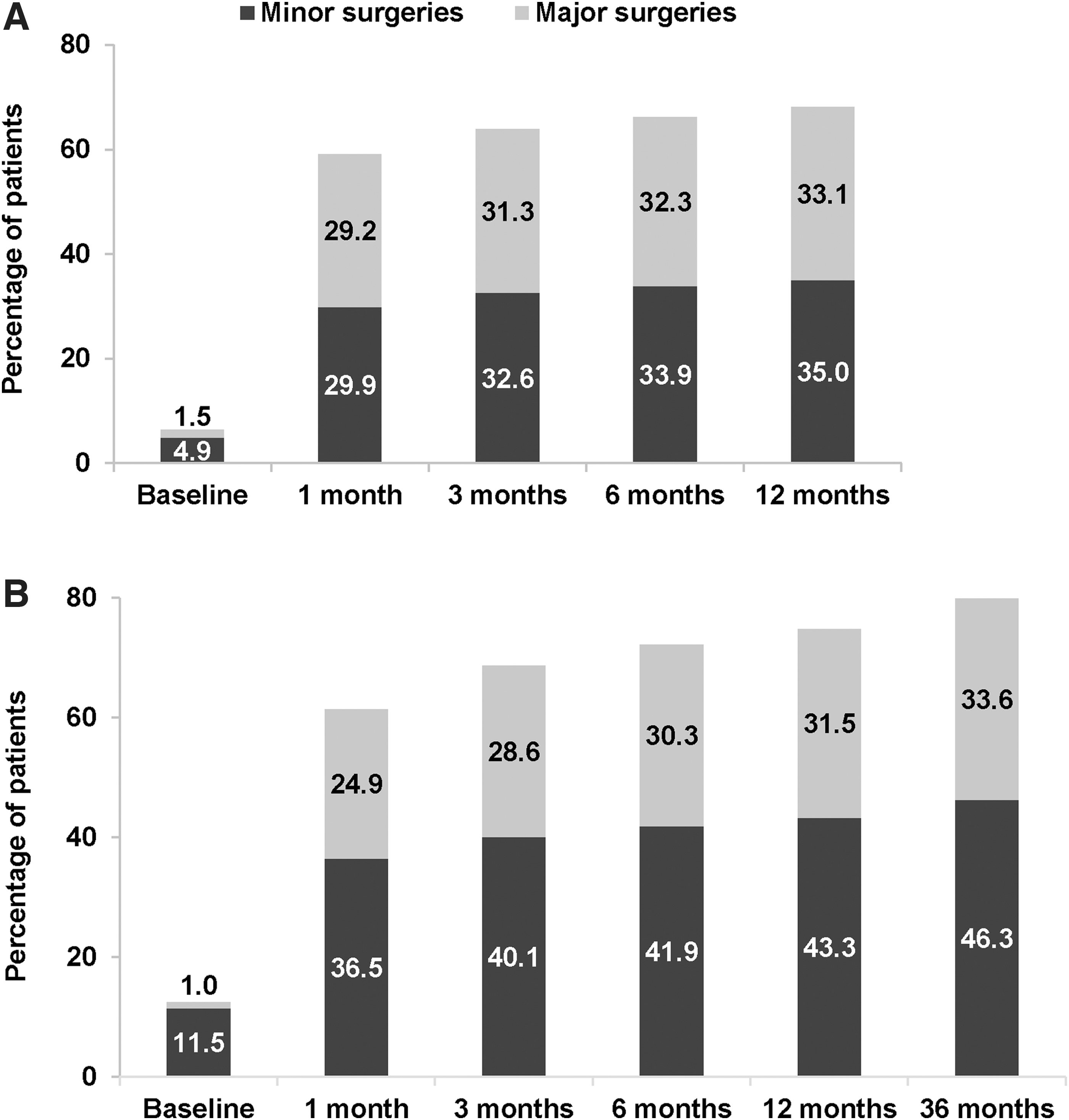
Surgery rates over time in the
Trends in treatment patterns
Examination of the most common sequences of treatment utilization in the baseline and follow-up periods showed that both cohorts exhibited a very diverse set of sequences (Fig. 3). For example, in the main cohort, there were 506 distinct treatment sequences in the baseline period and 775 during follow-up (350 and 995, respectively, for the sensitivity cohort). The top 10 treatment sequences represented 55.3% of women in the main cohort and 56.8% of women in the sensitivity cohort during the baseline period. Representativeness of the top 10 sequences decreased to 45.7% and 25.7%, respectively, during follow-up.

Treatment sequences in
To distinguish whether analgesics were being used for endometriosis-related surgery, we assessed analgesic medication use before, during, and after the prespecified surgery window (Fig. 4). This analysis showed that, as anticipated, in the main cohort, use of analgesics, and opioids in particular, escalated during the surgery window. However, substantial analgesic use was also observed outside the surgery window, especially the use of opioids. The same trend was observed in the 3-year follow-up sensitivity cohort, with higher numbers overall and particularly in the periods before and after surgery.
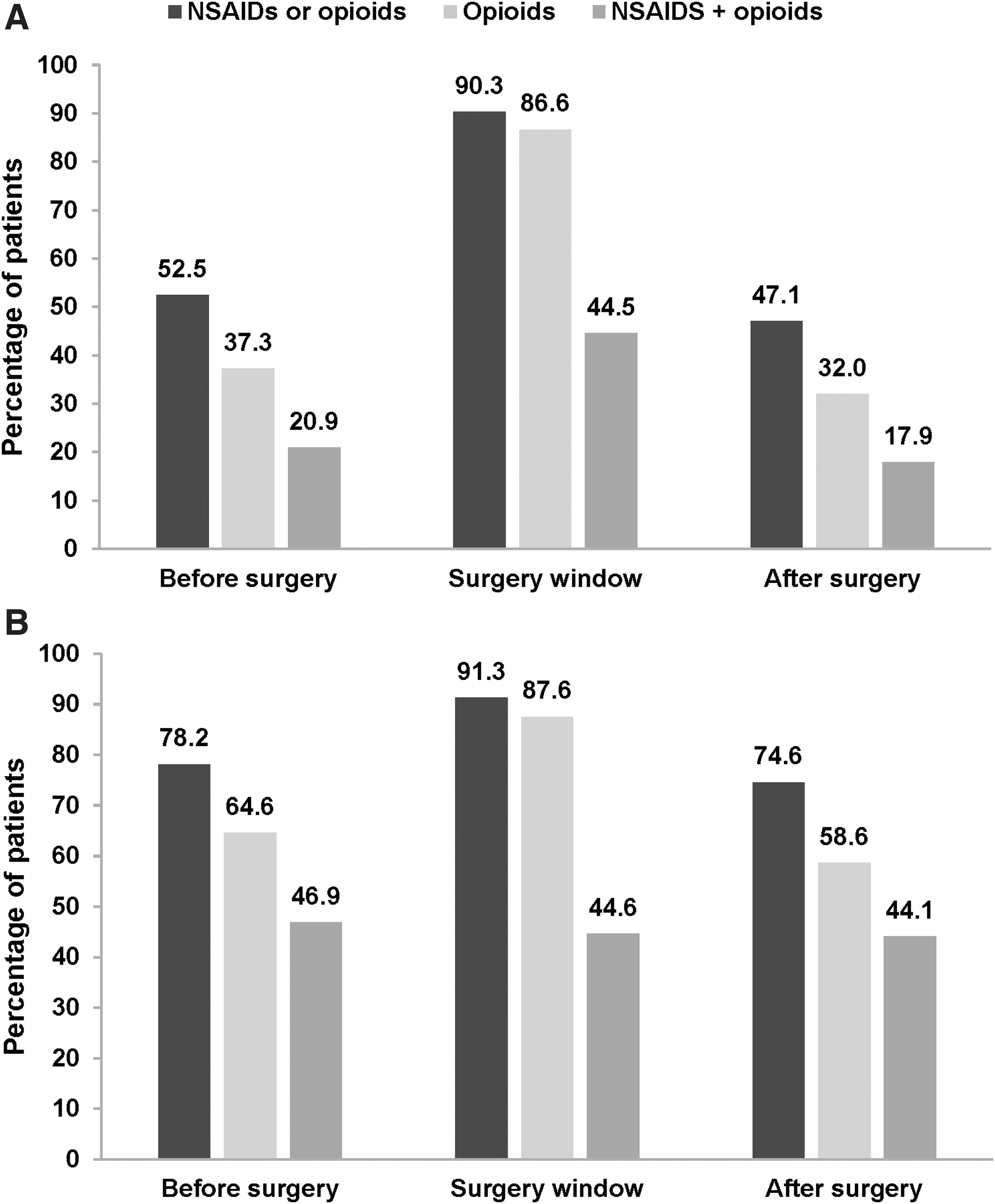
Analgesic medication use before, within, and after the surgery window in
Discussion
This study showed that, among commercially insured U.S. women, newly diagnosed with endometriosis, use of NSAIDs and opioids increased in the year after diagnosis, as did laparoscopies and hysterectomies. Treatment sequences were diverse and became more so after the index diagnosis, indicating the potential challenges of finding an effective treatment regimen for this patient population 22 and the lack of standardized guidelines for therapy. 23 The use of opioids was most frequent during the surgery window but remained prevalent outside this window, especially afterward, which suggests that surgery may not completely resolve endometriosis-related pain. Furthermore, the incorporation of a sensitivity cohort with longer preindex history and longer follow-up provided insight into the longer-term trends in the treatment journey of endometriosis patients.
Abdominal/pelvic pain was the most common comorbidity observed in our study population (36%). A similar frequency of abdominal/pelvic pain (25%) was observed in a previous claims analysis using a U.S. database, 16 although higher frequencies of pelvic pain (60%) were reported in two multinational surveys of women with endometriosis. 17,18 A higher percentage of patients with abdominal/pelvic pain was also observed in the sensitivity cohort of the current study (52%), indicating that, as time progresses, an increasing number of women experience this comorbidity. Other prominent symptoms in our study population were excessive or frequent menstruation, dysmenorrhea, and uterine fibroids. Each of these comorbidities was also observed, although at widely ranging levels, in previous studies of adult U.S. women with endometriosis. 6,24 –26
Pain-related comorbidities are invariably accompanied by the use of pain medication. From a baseline utilization rate of about 40%, we observed an increase in the use of analgesics after the index diagnosis (51% for NSAIDs and 69% for opioids). Conversely, hormonal agents exhibited a decrease in utilization rates postdiagnosis. GnRH analog use was low throughout the study period, but more than doubled from baseline to follow-up in the longer term sensitivity cohort, suggesting these agents may be used as second-line therapy.
In a recent claims analysis, Soliman et al. reported medication use rates of 89% for opioids, 74% for NSAIDs, and 45% for estrogen/progestin in the year before an endometriosis diagnosis in U.S. women 18–49 years of age. 16 Overall, estrogen/progestin use in the baseline period for the current study population was comparable, but NSAID (38%) and opioid (42%) use was much lower.
In the current study, opioids were the most frequently used drug class in the follow-up period (69%) and exhibited the largest change from baseline to follow-up. This is consistent with the rate of opioid use reported by As-Sanie et al. using a similar study design. 27 They found that in the year after diagnosis of endometriosis, 62% of women received a prescription for an opioid. Opioid consumption was highest in the first 3 months after the index date, followed by a decrease and stabilization of opioid consumption in the subsequent 9 months.
The current study also confirmed a surge in opioid use during the surgery window. A similarly high rate of opioid use was observed in 125 women undergoing laparoscopic hysterectomy for benign indications (21% with a history of endometriosis) at two U.S. teaching hospitals, where 98% were prescribed an opioid for acute postoperative pain. 28 In this study, a history of chronic pelvic pain or endometriosis and preoperative opioid use were among the patient characteristics most strongly correlated with postoperative opioid use. This is consistent with the finding of As-Sanie et al. that all other medications (NSAIDs, GnRH agonists, and contraceptive hormones) were used more frequently in women using opioids. 27 Together with these previous studies, our findings on opioid use outside the surgery window suggest that many women cannot fully control their pain even after surgery. However, whether the use of opioids after surgery is because of endometriosis-related or other types of pain needs to be further investigated.
Opioids are not among the guideline-recommended treatments for endometriosis, and both As-Sanie et al. 27 and Wong et al. 28 point out some of the pitfalls associated with their use. These include initial overprescription by physicians leading to possible dependency, and dose escalation by patients. Our data on the trends in opioid use indicate that many women use them primarily for surgery-related pain and that overall use of opioids decreases after a surgery. The postsurgery utilization rate of opioids that we observed (32%; Fig. 4) was higher than the rate reported for women in the general U.S. population in 2018 (22%), 29 but was within the range reported for patients with a variety of chronic diseases (24%–37%; male and female). 30,31
The post-index surgery rate observed in the current analysis (68%) was similar to the results of prior analyses of U.S. claims in women with endometriosis (66% 32 and 67% 16 ). We found that most patients had surgery within 1 month of the index date. This time trend is consistent with the surge in hospitalizations and cost observed in the 1st year after diagnosis in a 10-year medical claims database analysis. 10 Another assessment of trends in hospitalizations and surgeries from 2006 to 2015 showed that the prevalence of major surgeries for endometriosis (hysterectomy and oophorectomy) decreased, whereas that of minor surgeries (laparoscopy, laparotomy, other excision/ablation) increased during the current study period. 11 At least some of the surgeries during follow-up likely occurred on the index date.
This presumption is based on the finding of Fuldeore et al. that 49% of women classified as having post-index surgery had surgery on the index date 32 and the finding of Soliman et al. that 49% of diagnoses were surgical as opposed to clinical. 26 The difficulty of diagnosis and treatment of endometriosis by surgical means is illustrated by Wong et al., in whose study population 37% of women underwent hysterectomy for “pelvic pain or endometriosis” and 10% underwent resection of endometriosis, despite only 21% having a documented history of endometriosis; endometriosis was confirmed pathologically in just 16% of these women. 28 The procedure codes used to identify surgeries in the present analysis were not unique to endometriosis.
Limitations
This study has several limitations related to the use of administrative claims databases. First, with regard to identification of the population with endometriosis, diagnosis codes may not have been accurately coded or may not have represented the occurrence of actual disease (e.g., they were intended as a rule-out diagnosis). To address this limitation, we required at least two endometriosis diagnoses on different dates to ensure accurate capture of women with endometriosis in our sensitivity analysis. Even so, our diagnosis criteria were not required to be validated/confirmed by ultrasound exam as in Eisenberg et al. 33
In addition, the claims data were designed for health care billing and reimbursement and not for diagnostics. The diagnosis codes cannot be validated without individual medical records, and, therefore, it is possible that the results presented in this study are either over- or under-reported.
Furthermore, there can be difficulties obtaining a sample of women in the 18–26 years age range with continuous enrollment, since they may be transitioning on and off their parents' insurance. This may explain why the average age of our population (39 years) was higher than expected based on the results of Fuldeore et al., whose survey of U.S. women 18–49 years of age found that 53% of those with endometriosis were diagnosed between ages 18 and 29 years. 6 The underrepresentation of younger women in claims data may affect the generalizability of our findings.
Second, with regard to study variables, pain was assumed based on medication use, but its source and severity were not confirmed. For example, the high rates of opioid use outside the surgery window may suggest possible nonendometriosis-related sources of pain. As noted above, surgeries may have actually occurred on the index date, making temporal relationships between diagnosis and surgery difficult to establish. Contraceptives and GnRH analogs are often used for purposes other than treatment of endometriosis, and claims data do not differentiate the reasons for their use. Only prescription drugs were captured, which omits over-the-counter medications and other forms of self-management. Third, the present study included a 12-month baseline and follow-up period, which is a relatively short period of time, given that women with endometriosis have an average of 4.4–6.7 years' diagnostic delay. 17,26 It is possible that the relatively short baseline and follow-up period resulted in a low frequency of first-line therapies.
However, similar trends in pharmacological treatment patterns, surgical treatment patterns, and general treatment patterns were observed between the main and sensitivity cohorts. Finally, analyses of pharmacological and surgical treatment patterns were not stratified by demographic or clinical characteristics, so there is no insight into possible confounders of treatment. Future studies would benefit from statistical adjustment for demographic and clinical characteristics so that correlates of specific treatment patterns will be revealed.
The study design incorporated a relatively short baseline period that did not take into account possible delays in diagnosis. It has been shown that prediagnosis resource use and costs vary according to the length of time between symptom onset and clinical diagnosis, 34 so our main analysis did not capture any of this variation. However, our sensitivity cohort, which had 3 years of data collection before the index date, exhibited trends in treatment patterns similar to the main cohort.
With regard to the study results, subjects with multiple surgeries may have had another peak in opioid use, which would confound the findings on medication use within and outside the surgery window. Also, because the data were limited to individuals enrolled in a commercial health plan, the results are not generalizable to the broader U.S. population, that is, the uninsured or those on Medicaid.
Conclusions
In summary, this study demonstrates that NSAIDs and opioids are the most common pharmacological treatments used by women with endometriosis before and after diagnosis. Both major and minor surgeries were undertaken by a majority of women once diagnosed, usually within a month. Treatment patterns were diverse and not well aligned with published guidelines, suggesting the unmet need for earlier diagnosis and effective treatment alternatives for endometriosis.
Footnotes
Acknowledgments
The authors thank Melissa Stauffer, PhD, in collaboration with ScribCo, for medical writing assistance.
Author Disclosure Statement
J.W. and Z.L. are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA and may hold stock in Merck & Co., Inc., Kenilworth, NJ, USA. S.C. and K.M. are employees of Complete HEOR Solutions, North Wales, PA, USA and received financial compensation for their participation in the study analysis.
Funding Information
Funding was provided by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.