
Abstract
Background:
Women with human immunodeficiency virus (HIV) often have bacterial vaginosis (BV). The goal of this analysis was to assess how BV prevalence changed over time and across U.S. regions in enrollment cohorts of the Women's Interagency HIV Study.
Methods:
In a multisite study, BV was diagnosed retrospectively when pH and two of three other Amsel criteria were met. Prevalence was determined across four recruitment waves: 1994–5, 2001–2, 2011–2, and 2013–5. Generalized estimating equation multivariable logistic regression models assessed changes in visit prevalence across waves after controlling for HIV disease severity and other risks.
Results:
Among 4,790 women (3,539 with HIV and 1,251 without HIV), BV was diagnosed at 7,870 (12%) of 64,444 visits. Baseline prevalence across enrollment waves was 15.0%–19.2%, but declined in all cohorts, with prevalence in the initial cohort falling to 3.9% in the 1994–5 cohort after up to 21 years of continuous observation. Prevalence varied within U.S. regions. HIV status was not associated with BV.
Conclusion:
BV prevalence decreased with time in study. Prevalence varied across sites, but was not uniformly increased or decreased in any U.S. region. Clinical
Introduction
Bacterial vaginosis (BV) is a disorder reflecting vaginal microbiota alterations, with loss of lactobacilli and an increase in vaginal pH, discharge, and odor. 1 BV may impair quality of life and sexuality. 1 It predisposes to adverse pregnancy outcomes, pelvic infections, and infection with HIV. 1 The cause of BV is unknown, but it has been linked to sexual practices, Black or Hispanic ethnicity, smoking, and other factors. 1
Although HIV infection does not predispose to BV, BV is prevalent among women living with HIV (WLWH). For this reason, BV has been a research focus of the U.S. national cohort study of HIV in women, the Women's Interagency HIV Study (WIHS). Previous work from our group found that the cumulative incidence of BV approached 50% in WLWH, but actually was higher in HIV-negative women than in WLWH. 2,3 This finding was in contrast to that reached in the HIV Epidemiology Research Study, which found that HIV was associated with prevalent BV, especially among women with lowest CD4+ T cell counts. 4
The U.S. HIV epidemic has evolved over the past quarter century, not least since the development of potent antiretroviral therapies and shifts in the demographic characteristics of newly diagnosed women. These changes may alter the prevalence of disorders among WLWH, including BV. To account for this, the WIHS has conducted four waves of recruitment, including one targeted to integrate Southern U.S. women. This has allowed us to show that the prevalence of cervical cytologic lesions at study enrollment fell by half over successive recruitment waves. 5 A gradual decline in BV risk has occurred in WIHS, 2,3 with a WIHS substudy showing that with, microbiota profiles among WLWH showed an increase in the proportion with Lactobacilli, 6 but whether BV prevalence has fallen in enrollment cohorts in a way that might reflect national changes in BV risk is unknown.
The HIV epidemic in the Southern United States has unique characteristics, including a higher proportion of women than in other U.S. regions, disproportionate involvement of nonurban populations, and a disproportionate impact on African-American women. 7 Differences in BV risk factors may exist across U.S. regions, but whether regional differences in BV prevalence exist has not been explored. We set out to re-examine patterns of BV diagnosis in WIHS across time with a particular focus on the impact of enrollment wave and geographic region.
Methods
This investigation was part of the WIHS, an ongoing U.S. multicenter prospective cohort investigation of HIV and related health conditions among WLWH and demographically similar HIV-uninfected comparison women. The protocols, recruitment processes, procedures, and baseline results of the WIHS have been described. 8 –10 Enrollment began before the widespread introduction of combination antiretroviral therapy (cART) with 2,623 women (2,054 with HIV and 569 without) in 1994–5 at six study consortia (Bronx, Brooklyn, Chicago, Los Angeles, San Francisco, and Washington, DC). The cohort was expanded by an additional 1,143 women (737 with HIV and 406 without) during 2001–2002. The WIHS was augmented in 2011–12 by 371 additional women (276 with HIV and 95 without) to account for attrition, and most recently by 845 women (611 with HIV and 234 without) from newly funded study sites in the Southern U.S. (Chapel Hill, Miami, Atlanta, Jackson and Birmingham) in 2013–15. As of late 2016, 1,268 women had died, 130 had withdrawn from study, 806 had been discontinued for administrative/funding reasons, 415 had been lost to follow-up, and 2,363 were being actively followed.
Local human subject committees approved study protocols, and written informed consent was obtained from all participants. At entry and semiannually, questionnaires assessed demographic and medical history, and examinations were performed, including pelvic examinations with cervicovaginal specimen collection for wet mount examination, pH testing, and potassium hydroxide (KOH) whiff testing. Information about diagnosis and treatment of gynecologic conditions occurring between visits was not reliably collected. HIV serostatus was determined by enzyme-linked immunosorbent assay (ELISA) with confirmatory testing at study entry for all participants and semiannually thereafter for those initially seronegative.
Although follow-up continues, data from participant visits spanning the interval from October 1, 1994, through September 30, 2016, were included in this analysis. Participant visits were included in the analyses if they had available data on BV and the covariates of interest. Visits in which the participant reported pregnancy, breastfeeding, or was less than 12 weeks postpartum were excluded from analyses, as were visits at which participants reported use of vaginal medications within 48 hours before the visit. Because of the lower sensitivity of BV diagnosis using Amsel criteria among women with trichomonas co-infection, 11 visits also were excluded when trichomonas was identified through wet prep.
At each visit, specimens of vaginal secretions were collected. For all visits, BV was diagnosed for this study when vaginal pH >4.5 and two of three other Amsel criteria were met. 12 These included a finding of clue cells on wet mount, positive amine odor after KOH application to discharge, and a characteristic appearance to discharge. For Visits 1–8, characteristic discharge was considered present when recorded as any volume greater than none with a white or clear color. For Visits 9 and following, characteristic discharge was considered present when vaginal discharge was present and was milky/creamy/nonfloccular; other Amsel criteria were consistently defined throughout the 25 years of data collection. Clinicians were trained centrally in Amsel scoring before study initiation; new clinicians were directed to a PowerPoint training presentation that was available through the study's website to promote consistency in identification of Amsel criteria, including microscopic slides for presence and percent of clue cells. We did not consistently collect information about treatment after testing for women positive for BV by Amsel criteria.
Covariates of interest included recruitment wave, HIV serostatus, age at visit, self-reported race/ethnicity, household income, educational attainment, alcoholic drinks per week, smoking status, depressive symptoms (Centers for Epidemiological Studies-Depression [CES-D]), reported sexual activity and condom use (composite variable), hormonal contraceptive use, menopausal status, and enrollment WIHS site/location. Among analyses limited to WLWH, additional variables included CD4 nadir (lowest CD4 count at or pre-HAART initiation or, if no prior HAART initiation, lowest CD4 within WIHS), HIV viral load detection at visit, and cART use at visit. Women were considered menopausal if 50 years of age or older, had >12 months amenorrhea, and no later resumption of menses; premenopausal women had self-reported regular menstrual cycles.
Bivariate analyses used chi-square tests to assess the relationship between BV at a visit and sociodemographic and clinical variables. To control for repeat measures within participants, generalized estimating equations (GEEs), adjusted odds ratios (ORs), and 95% confidence intervals (CIs) were calculated to determine predictors of BV. In multivariable (GEE) logistic regression models, overall and stratified by HIV status, all variables associated with BV in the univariate adjusted models and selected from previous literature were included with the exception of enrollment site, due to collinearity with wave—since all participants in the 2013–5 enrollment were from southern sites and all southern sites' participants included only women in that wave. The proportions of women with BV at each visit, stratified by WIHS enrollment wave, were also assessed. All analyses were performed using SAS software, version 9.4 (SAS Institute, Inc., Cary, NC).
Results
After exclusions, 4,790 women (3,539 HIV+ and 1,251 HIV−) were identified, contributing 64,444 visits, with BV diagnosed at 7,870 (12%) of visits. Demographic, geographic, behavioral, and clinical characteristics of these women across visits are shown in Table 1 according to whether BV was present or absent. HIV serostatus was not associated with BV in GEE-adjusted analysis.
Characteristics of Women Assessed for Bacterial Vaginosis a Across Visits
n = 64,444.
Values in bold are statistically significant p < 0.05.
Bacterial Vaginosis determined using Amsel Criteria. Vaginal pH >4.5 and at least two out of three of the following positive: characteristic discharge, KOH odor, and presentation clue cells.
p-Values obtained from Chi-square tests.
Results are from the adjusted GEE model to control for repeat measures.
Results are from the adjusted multivariable GEE model. All variables listed were included in the model with the exception of enrollment site/location.
Not included in multivariable model due to collinearity.
CES-D, Centers for Epidemiological Studies-Depression; CI, confidence interval; GEE, generalized estimating equation; KOH, potassium hydroxide; OR, odds ratio.
Associations with BV that remained significant in a further multivariable adjusted analysis included younger age, nonwhite ethnicity, lower household income, alcohol and cigarette use, self-report of depressive symptoms, and vaginal sex, especially without condom use and with multiple partners. In a separate multivariable analysis restricted to WLWH, BV was associated with detectable HIV RNA level (adjusted OR 1.21, 95% CI 1.11–1.32), not using cART (adjusted OR 1.44, 95% CI 1.32–1.58). When compared to CD4 nadir ≥500 cells/μL, BV was associated with CD4 nadir below 200 cells/μL (adjusted OR 1.19, 95% CI 1.00–1.41), but not with CD4 nadir between 200 and 499 cells/μL (adjusted OR 1.13, 95% CI 0.97–1.33).
We further explored how BV prevalence changed across time among the four enrollment waves. Figure 1 graphically presents the prevalence of BV across semiannual follow-up visits. BV prevalence at the intake visit was similar across enrollment waves (Wave 1 18.1%, Wave 2 15.0%, Wave 3 19.2%, and Wave 4 17.2%, p = 0.16). With the exception of Wave 2, BV visit prevalence fell from the baseline visit to the first follow-up visit. All enrollment cohorts showed a decline in BV prevalence across time. The most recent cohort (Wave 4) reached 11.1% after only 2 years of observation, while long-term continuous cohort participants achieved a BV prevalence of 3.9% after 21 years of observation (prevalence at final visit among all Wave 1 participants accounting for missed visits was 5.0%).
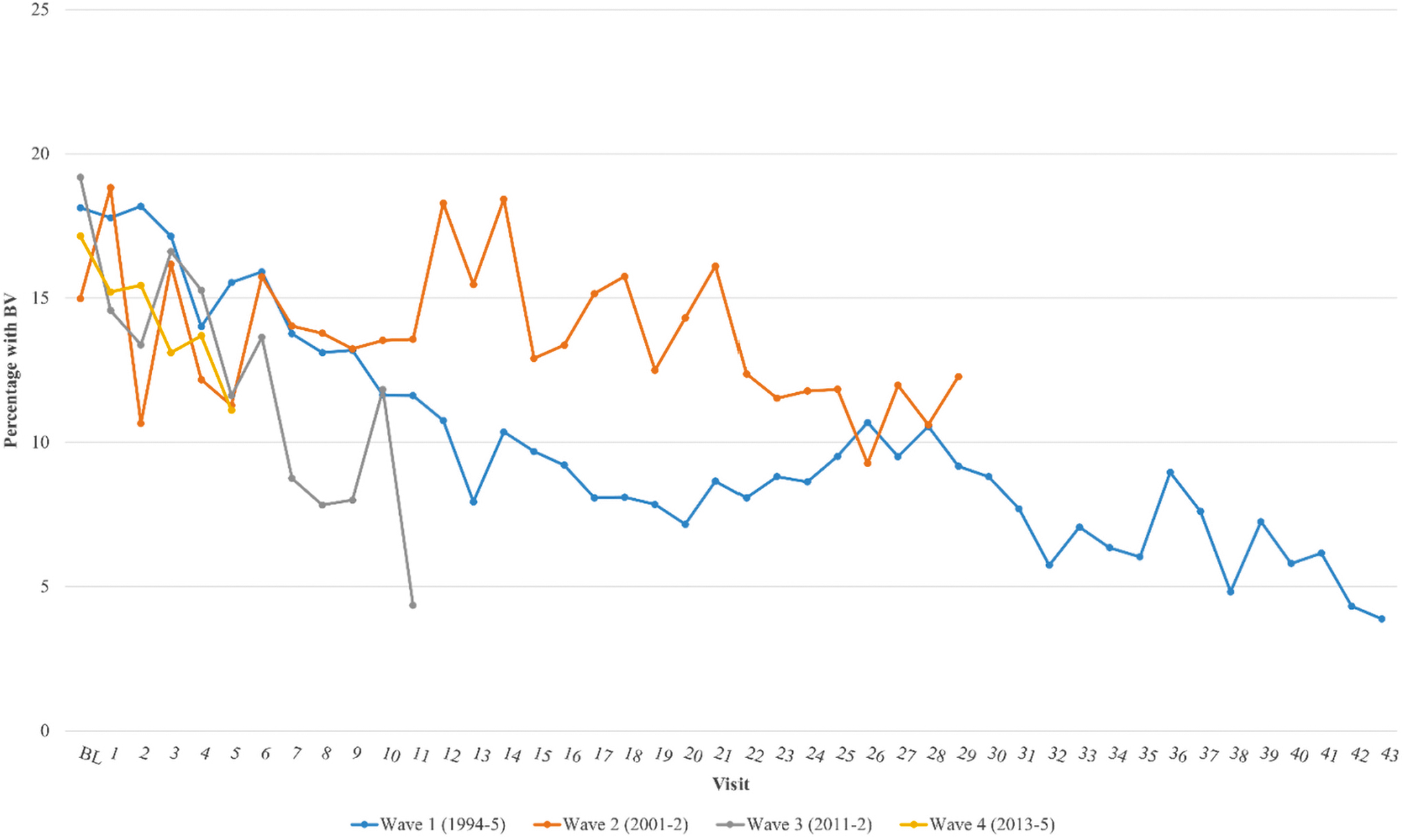
Proportion of women diagnosed with bacterial vaginosis across all four enrollment waves of the Women's Interagency HIV Study (1994–5, 2001–2, 2011–2, and 2013–5). Visit number reflects the number of visits attended by individuals in each enrollment wave; missed visits are not included. (p-trend: Wave 1 < 0.0001, Wave 2 0.008, Wave 3 < 0.0001, and Wave 4 0.017).
We combined sites in an effort to evaluate differences in BV prevalence across U.S. regions, such that Brooklyn/Bronx/DC sites composed an Eastern group, Chapel Hill/Atlanta/Miami/Birmingham/Jackson a Southern group, and Los Angeles/San Francisco a Western group, with Chicago as the sole Midwestern site. Compared to the Eastern group, the GEE-adjusted ORs were Midwestern 0.98 (95% CI 0.82–1.16), Western 0.59 (95% CI 0.50–0.68), and Southern 0.89 (95% CI 0.77–1.01). However, generalizations about regional differences must be limited by substantial differences in BV prevalence within regions. For example, although prevalence in Western sites was lower and in Southern sites was higher, as shown in Table 1, compared to BV prevalence in the Bronx, prevalence in San Francisco was lower and in Los Angeles was higher. Similarly, risk was increased relative to the Bronx site in Atlanta and Miami, but not in Jackson or Birmingham, and in fact was lower in Chapel Hill.
Discussion
Among women recruited to WIHS across two decades, baseline BV prevalence ranged from 15% to 19% and fell across time, to a low of 4% in the cohort of women followed for up to 21 years. Reasons for the decline may include aging of the cohort, case-finding and treatment, declines in sexual frequency and number of partners, 13 a reduction in smoking with time on study, 14 changes in contraceptive use with time, 15 and possibly other factors. We were not able to tease out the individual impact of these potential contributors. Nevertheless, women with BV can be reassured that BV risk declines with time.
As we and others have shown, HIV seropositivity was not independently associated with BV, and we did not identify geographic regions of the United States with uniformly higher or lower BV prevalence across component sites. Rather, BV was linked to African-American race, younger age, lower household income, sexual and contraceptive practices, and smoking. Prevalence varied across sites without a regional trend. These factors remained associated with BV prevalence after controlling for cohort enrollment wave across two decades. Appreciation of those risks may allow clinicians to target BV assessment and therapy to women with risk factors. Our findings mirror those reported for the general population, in whom BV has been associated with sexual practices, including condom use and multiple partners, hormonal contraception, African or African-American race, douching, smoking, poverty, dietary factors, including low vitamin D levels, and chronic stress. 16 Clinicians caring for women with BV should query WLWH about vaginal symptoms and incorporate Amsel scoring of vaginal discharge into routine care. Repeated treatments may be needed to suppress BV, and innovative treatments such as microbiome transplant may be useful in further driving down BV risk in cohorts like ours.
Despite substantial declines in prevalence across time, BV persisted in our cohorts. We were unable to determine whether women with BV across visits were a constant cohort of women who were not treated, declined treatment, or failed to respond to acute or suppressive therapy, or whether a larger number women cycled between normal and abnormal microbiota with a slowly declining proportion testing positive at each visit. Future studies should incorporate treatment information to distinguish among these possibilities; doing so may allow assessment of the comparative effectiveness of varying therapies on high-risk women. BV diagnosis using alternate diagnostic strategies, such as Gram stain or nucleic acid amplification testing, may provide additional insights.
The cause of the microbiome changes characteristic of BV is unclear, but BV may result from sexual transmission of bacterial species that create a pathogenic microbiome and vaginal biofilm. 17 We found that HIV was not associated with a BV diagnosis after adjusting for other sociodemographic factors, and among WLWH, BV was associated with low CD4 nadir (<200 cells/μL) and it was marginally more common among women with detectable HIV and among those not on cART. This suggests that BV is not an opportunistic infection, but a microbiome alteration common among younger, lower-income African-American women, especially those with multiple vaginal sex partners. We found depressive symptoms to be associated with BV, and this may reflect the impact of stressors on vaginal flora, 18 although chronic symptomatic BV may contribute to depression as recurrent BV has been shown to impair quality of life. 19 Since it might have changed vaginal pH and wet mount findings, we excluded women who reported douching, so we cannot assess the impact of vaginal hygiene practices on BV. Despite these areas of uncertainty, clinicians caring for WLWH and women with similar BV risk profiles should be familiar with diagnostic and treatment protocols, including long-term suppressive therapy for this frequently recurring disorder.
BV is one extreme in a continuum of changes in vaginal flora that may not produce symptoms or signs. Clinically apparent discharge was not present in 26% of those diagnosed with BV. How clinically apparent and subclinical BV may differentially impact quality of life, medical complications, and HIV transmission among women with and at risk for HIV remain an area for further research. The effectiveness of both acute and suppressive treatments for BV with and without clinical discharge should be studied in greater detail in WLWH.
Several aspects of cohort study design limit the insights that can be drawn. We cannot entirely exclude the possibility from our finding that BV prevalence falls across time, and may be an artifact of survival and participation bias, whereby women at highest risk for BV died or dropped out of study. Previous WIHS work has shown that mortality in WIHS has been linked to nonwhite race, depression, smoking, alcohol use, and low income. However, these factors, except depression, lost significance in a recent multivariable analysis. 2 It is unlikely that survival and participation bias fully explain the long-term decline in BV risk that we observed.
Although some women enrolled in WIHS had Gram stain specimens collected at some visits to allow BV scoring by Nugent criteria and some even had microbiome assessment, only Amsel criteria were broadly available for all participants at all visits. Amsel criteria are subjective and include scoring for the presence of a visible vaginal discharge, while the more sensitive Nugent criteria do not. 20 However, the interobserver reliability of Amsel scoring appears good, 21 clinician staffing was relatively stable, and declines in BV prevalence across time were unlikely to be due to inability to diagnose BV. Amsel scoring is recommended for BV diagnosis by the American College of Obstetricians and Gynecologists because of its practicality. 22 HIV does not complicate the diagnosis of BV. 23 More sensitive Nugent testing might uncover additional risk factors we could not identify. Amsel criteria include presence of a discharge, while Nugent scoring focuses on microbiologic changes apparent on Gram stain. It remains to be determined whether among WLWH case-finding evaluation of BV-related microbiome changes using Nugent or microbiologic assessment might lead to better quality of life or other clinical outcomes over focused assessment of women with symptomatic discharge.
We found substantial variation by site in BV diagnosis rates, variation that remained significant after adjustment for other known risk factors, and this may reflect variation in clinicians' skills in BV diagnosis by Amsel criteria. Future studies should include interval training and clinician assessment, which now can be conducted virtually. We did not assess how BV diagnosis or therapy impacted women's quality of life, but some women—especially those without clinically apparent discharge—were asymptomatic; future studies should explore how BV affects women and how treatment ameliorates negative impacts.
Conclusion
This large longitudinal study showed that among at-risk U.S. women, including WLWH, BV prevalence has remained relatively steady across the past two decades, as reflected in similar baseline BV prevalence among serial enrollment waves recruited up to two decades apart. Although BV remains a serious problem for a substantial minority of women, time on study was associated with a decline in BV prevalence from intake in all recruitment cohorts. Women with BV should be encouraged to recognize that, although BV may be difficult to treat and slow to resolve, long-term improvements in BV prevalence can follow from careful serial assessment.
Footnotes
Author Disclosure Statement
Dr. Adimora reports receiving consulting fees from Merck, Viiv, and Gilead; Gilead and Merck have provided her institution with research funding. The other authors report no conflict of interests relevant to the work.
Funding Information
The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). MWCCS (Principal Investigators): Atlanta CRS (Ighovwerha Ofotokun, Anandi Sheth, and Gina Wingood), U01-HL146241; Baltimore CRS (Todd Brown and Joseph Margolick) and U01-HL146201; Bronx CRS (Kathryn Anastos and Anjali Sharma), U01-HL146204; Brooklyn CRS (Deborah Gustafson and Tracey Wilson), U01-HL146202; Data Analysis and Coordination Center (Gypsyamber D'Souza, Stephen Gange and Elizabeth Golub), U01-HL146193; Chicago-Cook County CRS (Mardge Cohen and Audrey French), U01-HL146245; Chicago-Northwestern CRS (Steven Wolinsky), U01-HL146240; Northern California CRS (Bradley Aouizerat, Jennifer Price, and Phyllis Tien), U01-HL146242; Los Angeles CRS (Roger Detels), U01-HL146333; Metropolitan Washington CRS (Seble Kassaye and Daniel Merenstein), U01-HL146205; Miami CRS (Maria Alcaide, Margaret Fischl, and Deborah Jones), U01-HL146203; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01-HL146208; UAB-MS CRS (Mirjam-Colette Kempf, Jodie Dionne-Odom, and Deborah Konkle-Parker), U01-HL146192; and UNC CRS (Adaora Adimora), U01-HL146194. The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional co-funding from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD), National Institute on Aging (NIA), National Institute of Dental & Craniofacial Research (NIDCR), National Institute of Allergy and Infectious Diseases (NIAID), National Institute of Neurological Disorders and Stroke (NINDS), National Institute of Mental Health (NIMH), National Institute on Drug Abuse (NIDA), National Institute of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), and National Institute on Minority Health and Health Disparities (NIMHD), and in coordination and alignment with the research priorities of the National Institutes of Health, Office of AIDS Research (OAR). MWCCS data collection is also supported by UL1-TR000004 (UCSF CTSA), P30-AI-050409 (Atlanta CFAR), P30-AI-050410 (UNC CFAR), and P30-AI-027767 (UAB CFAR).