
Abstract
Background:
Hirsutism is the most common clinical symptom of hyperandrogenism, but racial and ethnic-specific thresholds have not been established. Our objective was to characterize hirsutism using self-report of hair growth in a large sample of African American women.
Materials and Methods:
The Study of Environment, Lifestyle, and Fibroids is a prospective community-based cohort study of African American women (23–34 at recruitment). A total of 1568 participants received the modified Ferriman–Gallwey (mFG) pictorial assessment and were asked if they were ever bothered by excess hair. We estimated the prevalence of hirsutism (mFG score ≥8) and associations of acne, polycystic ovary syndrome (PCOS), and menstrual cycle characteristics with hirsutism. We also explored hirsutism defined by the 95th percentile of scores in our cohort (mFG = 11) and a newly recommended criterion, mFG = 4.
Results:
We could determine hirsutism status in 1556 women. Thirty-seven percent reported being bothered by excess hair, and 10% met the mFG criterion for hirsutism. History of severe facial acne was positively associated with hirsutism (prevalence ratio: 1.90; 95% confidence interval [CI]: 1.30–2.76), as was physician-diagnosed PCOS (2.22, 95% CI: 1.30–3.81). Women with irregular menstrual cycles were also more likely to report hirsutism (1.78, 95% CI: 1.00–3.18). Results were similar using mFG ≥11 and attenuated using mFG ≥4.
Conclusions:
Hirsutism prevalence was 10% in this community sample of African American women and was associated with PCOS, severe acne, and irregular menstrual cycles suggesting this represented hirsutism caused by hyperandrogenism. Ethnically diverse, population-based studies assessing the association between mFG score and androgen levels are needed to better understand the hirsutism threshold as a clinical marker of hyperandrogenism.
Introduction
Hirsutism is the presence of excess terminal hair growth in androgen-dependent areas of the body. 1 It is the most common clinical symptom of hyperandrogenism, or elevated androgen levels. 2 Other symptoms of hyperandrogenism such as severe facial acne and conditions related to androgen excess such as polycystic ovary syndrome (PCOS) and irregular menstrual cycles are associated with the presence of hirsutism, 2 –4 as are less common but more serious etiologies, including congenital adrenal hyperplasia and androgen-secreting tumors. 1,5
Ferriman and Gallwey proposed a scale in 1961 to clinically assess body hair in women by using illustrations depicting varying degrees of dark hair growth. 6 This scale was adapted in 1981 by Hatch et al., 7 focusing on nine androgen-sensitive areas of the body (upper lip, lower face and chin, chest, stomach, below the belly button, upper arms, inner thighs, back and shoulders, and lower back). This modified Ferriman–Gallwey (mFG), ranges from 0 to 36 and assigns a cutoff of 8 to define hirsutism. Eight represents the 95th percentile in the original cohort of 161 predominantly white women ages 18–386 and continues to be used as the clinical standard to diagnose hirsutism.
Although the scale was established decades ago, the prevalence of hirsutism in the general population and in racially and ethnically diverse groups has not been well studied, and it is not yet clear whether a cutoff of 8 on the mFG scale is appropriate in all populations. 8 The prevalence of hirsutism has been estimated in numerous studies in combination with estimating the prevalence of PCOS, 9 –15 but the resulting data have limitations. Even in cohorts recruited from the general population, most studies were relatively small and did not exclude women on medications that could alter the appearance of terminal hair growth. However, altogether, these studies suggest that the prevalence of hirsutism using the standard mFG cutoff of ≥8, varies across racial and ethnic groups with the highest prevalence reported in women of Mediterranean decent 16,17 and the lowest in East Asian populations. 18 –20 For these reasons, the Androgen Excess and PCOS Society Task Force highlighted the need for large population-based studies of unselected women to establish racial and ethnic-specific cutoff values for hirsutism 8 and population-specific normative ranges for the clinical features of PCOS. 21
The objective of this article is, therefore, to characterize hair growth in a large sample of young African American women with the goal of providing hirsutism data for this understudied group. We examine the prevalence of hirsutism based on participants' self-assessment of hair growth and assess whether women with other conditions associated with hyperandrogenism were more likely to report hirsutism. As clinical treatment for excess hair growth depends on patient perception, not mFG score, 1 we also compare mFG scores to women's report of being bothered by excess hair.
Materials and Methods
Study population
The Study of Environment, Lifestyle, and Fibroids (SELF) is a community-based prospective cohort study of 1693 African American women with the objective of estimating fibroid incidence and growth. The baseline study visit occurred in 2010–2012, and three subsequent visits have been conducted at ∼20-month intervals. Given the objective of the parent study, clinic visits were focused on ultrasound screening to detect new fibroid development. Detailed study methods have been described previously. 22 Briefly, self-identified African American women 23–34 years of age were recruited from the Detroit, Michigan area. Participants were eligible if they had an intact uterus and no previous clinical diagnosis of fibroids. This study was approved by the Institutional Review Boards of the National Institute of Environmental Health Sciences and Henry Ford Health Systems. All participants provided informed consent.
Assessment of hair growth
Participants who attended the third study visit (June 2014 to May 2016) were given a questionnaire about hair growth patterns (n = 1438). Women who missed the third visit completed the questionnaire at the fourth study visit (May 2016 to August 2018; n = 130). Women were asked if they were bothered by excess hair growth and then given a checklist of the nine androgen-sensitive areas and asked to indicate on which they had any “darker, thicker hairs” (Supplementary Appendix SA1). Then they completed the mFG assessment using illustrated depictions of increasing degrees of dark hair growth on each of the nine androgen-sensitive areas (Supplementary Appendix SA2). Women selected the picture that best represented the amount of darker colored hair they had before using any hair removal method.
We used ≥8 as the current clinical standard for assessing hirsutism. 6,7 To calculate the score participants' responses were recorded on a scale from 0 (picture with no dark hair growth) to 4 (picture with the most excessive dark hair growth) for each body part. The scores from the nine individual body parts were summed to calculate the mFG score (range from 0 to 36).
Assessment of descriptive characteristics for participant
Participant demographic, reproductive, and behavioral characteristics reported at the study visit when hair growth patterns were assessed were used in the analysis. Age at menarche, however, was assessed at the baseline visit for all participants.
Assessment of PCOS, acne, menstrual cycle length, and medications for hirsutism
Information on physician-diagnosed PCOS was obtained from participants at baseline and at each follow-up visit. Physician-diagnosed PCOS may include clinical/biochemical hyperandrogenism and irregular menstrual cycles (NIH criteria), 23 at least two of the three following characteristics: irregular menstrual cycles, clinical/biochemical hyperandrogenism, and polycystic ovary morphology (Rotterdam criteria), 4 or clinical/biochemical hyperandrogenism in addition to polycystic ovary morphology or irregular cycles (Androgen Excess Society criteria). 24 History of severe facial acne (a symptom of hyperandrogenism) 2 was assessed by showing participants a photo of an African American woman with severe facial acne and asking them to compare it to their own experience (Supplementary Appendix SA3). Participants who ever had acne that was more severe, about the same, and somewhat less severe were classified as having a history of severe facial acne. To address recent facial acne, women were asked to report the number of (1) blackheads and whiteheads, (2) pimples and papules, and (3) nodules and cysts on their face and neck in the past 12 months (Supplementary Appendix SA4). For each type of acne, women were given the option to choose none, 1–5, 6–10, 11–15, 16–20, and >20. Severe adult acne was defined as responding in the top two categories of the scale (≥16) for any type of acne. Usual cycle length was ascertained from participants' report of their typical menstrual cycle length over the past year. Those data were categorized as short (≤26 days), normal (27–34 days), long (≥35 days), and irregular (women who reported their cycle was too irregular to estimate).
Medications that could affect excess hair growth include hormonal contraceptives and antiandrogens such as spironolactone, drospirenone, and metformin. 25 Participants who reported taking any of these medications in the 24 hours before the study visit at which they completed the hirsutism questionnaire were classified as current medication users. We also considered women who reported hormonal contraceptive use in the past 4 weeks and those who reported taking a long-acting hormonal contraceptive that would still be active at the time of the study visit as current medication users.
Statistical analyses
We included participants who answered enough questions on the mFG assessment to determine their hirsutism status. Descriptive statistics were calculated for participant characteristics, stratified by hirsutism status (mFG ≥8 vs. mFG <8). To assess the body parts, women most commonly reported having dark hair growth, we calculated the percent of women choosing an illustration corresponding to a score of 1 or greater for each body part by hirsutism status. In addition, we compared hirsutism with women's feelings about being bothered by excess hair.
We performed log-binomial regression to estimate prevalence ratios (PRs) and 95% confidence intervals (CIs) for the association of: history of severe facial acne, physician-diagnosed PCOS, and menstrual cycle length with hirsutism. For these analyses, women who were taking a medication that could reduce hair growth (hormonal contraceptives, spironolactone, drospirenone, or metformin) were excluded because of the potential for bias due to underreporting of excess hair. This analytic sample was similar to the full cohort with regard to the range of mFG scores and proportion of women with hirsutism. All models were adjusted for age in 5-year categories (27–31, 32–36, 37–41 years). Models for menstrual cycle length were additionally adjusted for body mass index (BMI) categories (underweight, normal weight, overweight, obese class I, and obese class II and III), 26 because BMI can alter cycle length. The models for menstrual cycle length also excluded an additional 54 participants who reported that they took a medication that stopped or affected the frequency of their menstrual cycles for the entire year before the study visit (n = 24) or that they had ≤1 menstrual cycle in the prior year (n = 30).
We performed three sensitivity analyses. (1) To evaluate adult acne, we assessed the association between severe adult acne (created from report of the quantity of acne in the past 12 months) and hirsutism. (2) To evaluate whether associations of PCOS, acne, and menstrual cycle length were consistent when we included women who were taking medications that could reduce hair growth (because these medications may have been taken for reasons unrelated to excess hair growth), we reran these analyses, including all women in the cohort. (3) To evaluate the original mFG criteria for hirsutism in our cohort, we categorized women as having hirsutism if they had a score in the 95th percentile or greater and assessed associations of PCOS, acne, and menstrual cycle length with this more restrictive definition of hirsutism. We also applied a less restrictive hirsutism definition based on a recent international guideline for assessing PCOS that recommends an mFG ≥4 to indicate hirsutism 27 and assessed the same associations to evaluate the potential for hyperandrogenism at lower mFG scores.
To assess whether the initial checklist question about dark body hair might be used in future research as a screening question to identify women with an mFG score of 0 (thus allowing them to skip the mFG assessment), we descriptively compared responses to these questions with their answers to the mFG. Using the mFG score as the gold standard, we calculated the negative predictive value (NPV), the proportion of women who responded “none of the above” to the dark hair checklist question who had an mFG score of 0, and specificity, the proportion of those with an mFG score of 0 that answered “none of the above.”
All statistical analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC).
Results
Of the 1556 women included in this study (Supplementary Fig. S1), 10% had hirsutism (mFG score ≥8). mFG scores ranged from 0 to 36 (Fig. 1); median: 2 (interquartile range 0–4). Women across the range of mFG scores reported being bothered by excess hair, including 12% who reported an mFG score of 0 (Fig. 2). Thirty-seven percent of participants were bothered by excess hair, the majority of whom did not meet mFG criteria for hirsutism or had not been diagnosed with PCOS (Fig. 3). Among participants with hirsutism, the most common areas of the body for reported dark hair growth were the upper lip, chin and lower face, stomach, below the belly button, and inner thighs (Supplementary Table S1; >80% of women with hirsutism reported excess hair at these five sites). Most participant characteristics did not vary by hirsutism status (Table 1). The major exception was BMI (a higher proportion of women with BMI ≥35 had hirsutism). Current antiandrogenic medication use was also more common in women with hirsutism.
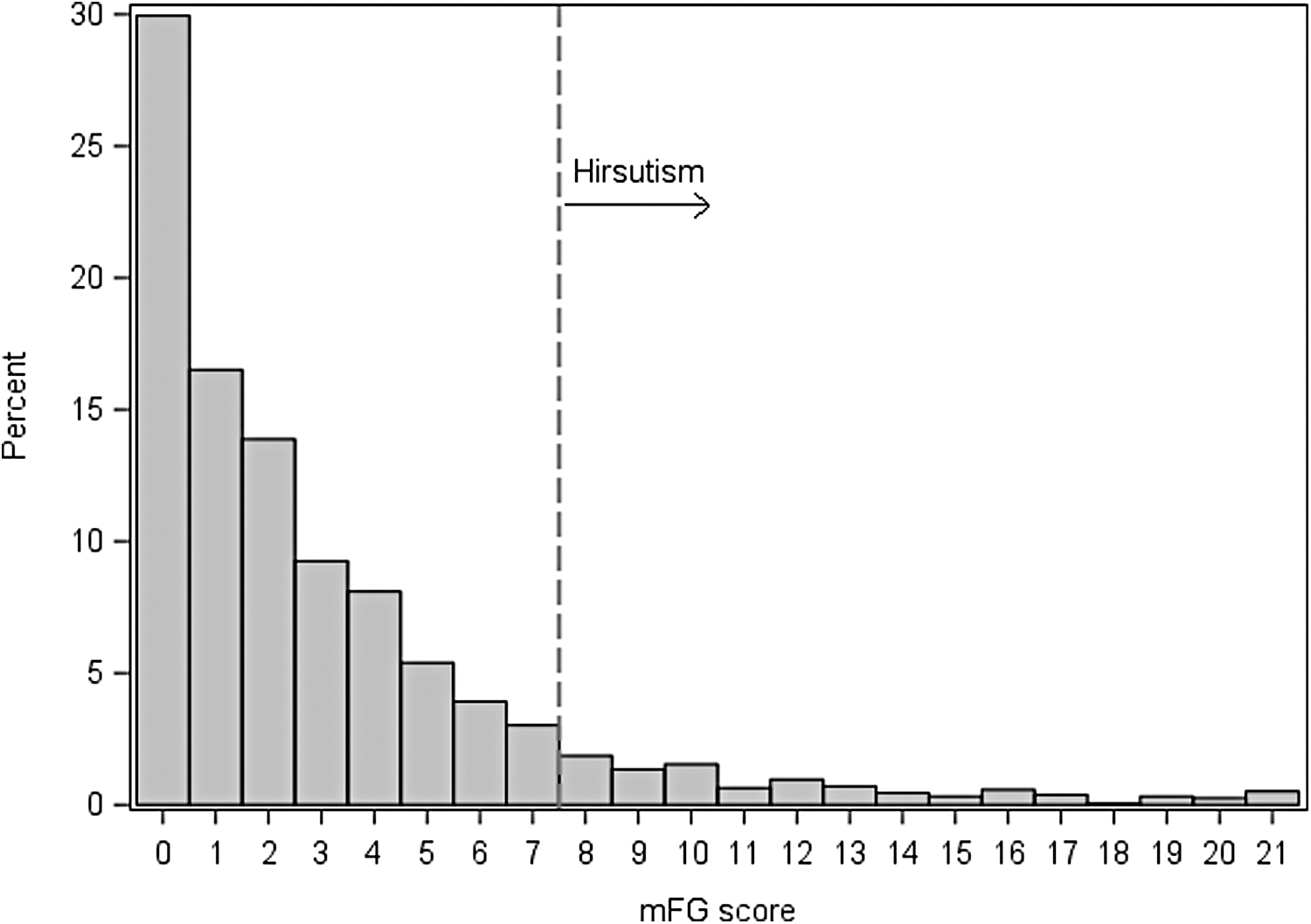
Histogram of mFG scores for SELF participants (n = 1556). Gray bars represent percent of women at each mFG score for scores 0–20; scores between 21 and 36 are combined in the 21+ bar (n = 8). Dashed line indicates the threshold used to define hirsutism (mFG score ≥8). mFG, modified Ferriman–Gallwey; SELF, Study of Environment, Lifestyle and Fibroids.
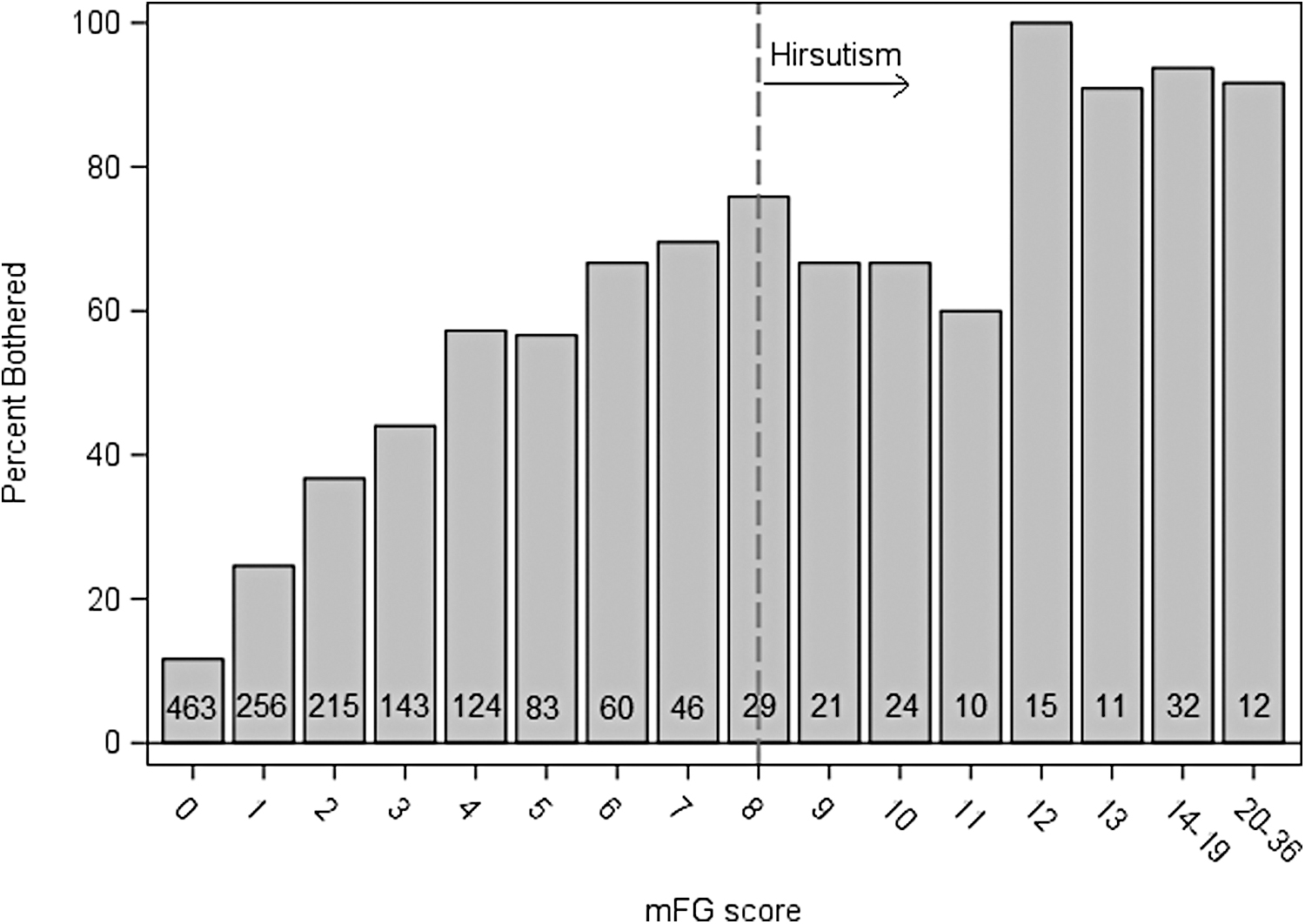
Bar chart of percent of women with increasing mFG scores who reported being bothered by excess hair among SELF participants (n = 1544). Gray bars represent the percent of women at individual mFG score for scores with ≥10 women (0–13), and combined scores 14–19 and 20–36. Numbers in the bars represent the total number of women reporting that mFG score. The dashed line indicates the threshold used to define hirsutism (mFG score ≥8). Those with missing data on the question about being bothered by excess hair growth (n = 12) were excluded.
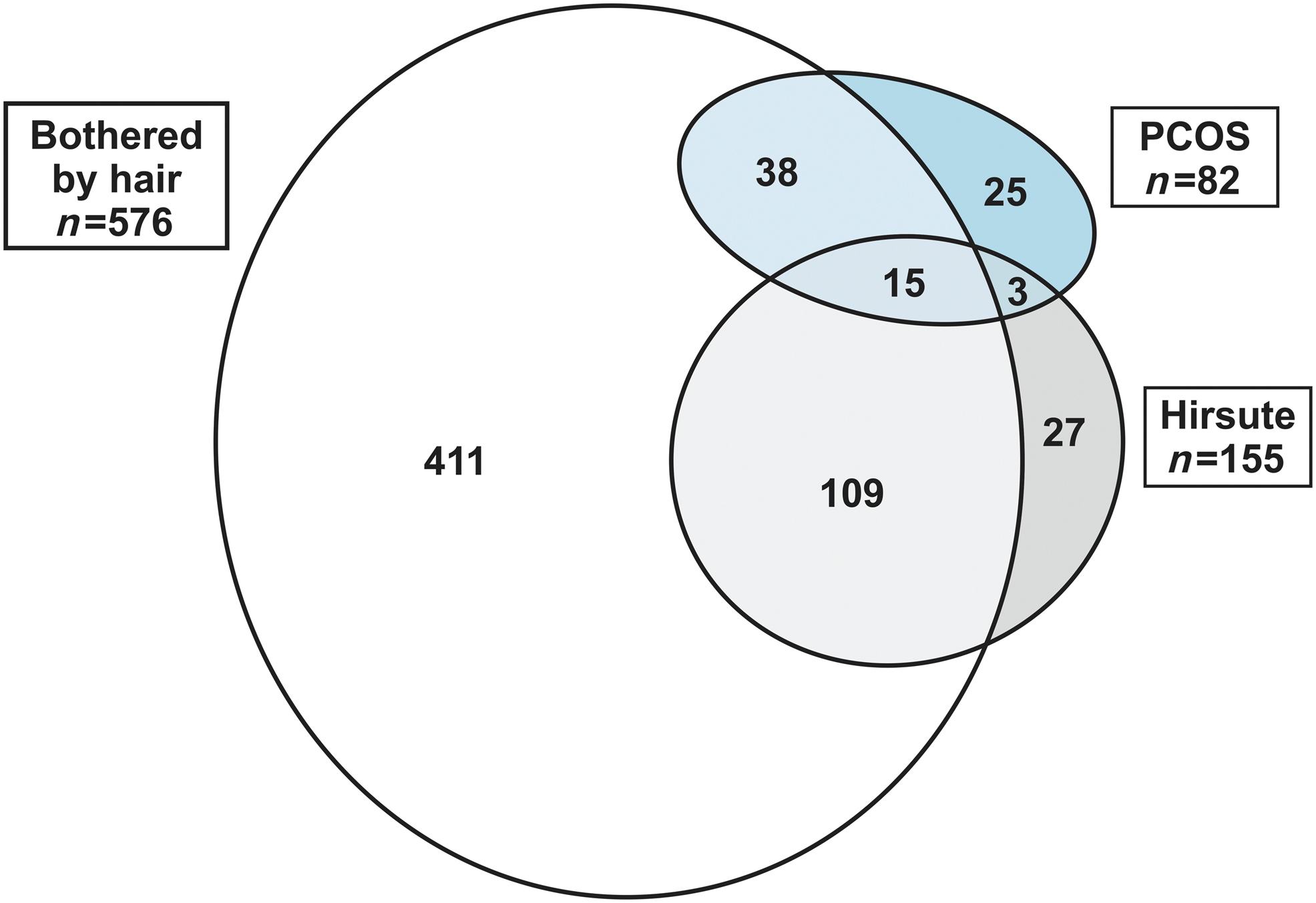
Venn diagram of SELF participants reporting PCOS, being bothered by excess hair, and hirsutism (n = 630). The figure includes two women missing responses to the question about whether they were bothered by excess hair (one had PCOS only and one had hirsutism only). Those who did not have any of the three conditions (n = 916) or were missing responses to the question about whether they were bothered by excess hair and did not have hirsutism or PCOS were excluded from the figure. PCOS, polycystic ovary syndrome.
Participant Characteristics by Hirsutism Status (n = 1556)
Obese I: BMI 30–34.9, Obese II and III: BMI ≥35.
Current use of metformin (n = 30), spironolactone (n = 3).
Includes eight women currently using an oral contraceptive pill with drospirenone.
BMI, body mass index; mFG, modified Ferriman–Gallwey.
Self-report of a history of severe facial acne compared with mild or no acne was positively associated with hirsutism (PR: 1.91, 95% CI: 1.31–2.79), as was physician-diagnosed PCOS compared with women without PCOS (PR: 2.22, 95% CI: 1.30–3.81; Table 2). Women reporting irregular cycles compared with normal cycles (PR: 1.78, 95% CI: 1.00–3.18) were also more likely to report hirsutism. Results from our sensitivity analyses were mostly consistent with the main analysis. Women reporting severe adult acne had approximately twice the prevalence of hirsutism (PR: 2.15, 95% CI: 1.47–3.16). Associations in the full cohort were similar to the subset that excluded women taking medication that might affect hair growth, except that, women in the full cohort who reported long menstrual cycles were also more likely to report hirsutism (PR: 1.75, 95% CI: 0.92–3.33) (Supplementary Table S2). Using a cutoff of 11 (95th percentile of mFG scores) associations of severe acne, PCOS, and cycle length with hirsutism were generally similar to the main analysis although less precise with only 62 women in this categorization of hirsutism (Supplementary Table S3). When we expanded the definition of hirsutism to include women with an mFG ≥4 (75th percentile), associations of severe acne, PCOS, and cycle length with hirsutism were attenuated (Supplementary Table S4).
Associations of Severe Facial Acne, Polycystic Ovary Syndrome, and Menstrual Cycle Length with Hirsutism Among Women Not Currently Using an Antiandrogenic Medication or Hormonal Contraception (n = 1150)
Current hormonal contraception, metformin, spironolactone, or drospirenone users excluded (n = 406).
Models adjusted for age (27–31, 32–36, 37+ years).
Ten women did not respond to the question about history of severe facial acne.
Cycle length model adjusted for BMI (underweight, normal weight, overweight, obese I, and obese II and II).
Thirty women missing usual cycle length because they reported not having a period or only one period in the 12 months before the study visit and 24 excluded for taking a hormonal birth control or another medication that regulated their period for the then entire 12 months period before the interview.
CI, confidence interval; PCOS, polycystic ovary syndrome; PR, prevalence ratio.
We found that responses to the initial checklist could not be used as a surrogate for mFG scores. The NPV for an mFG score of 0 using the general dark body hair question was only 0.50 and specificity = 0.95. Twenty-four of the women reporting no dark body hair on the checklist were classified as hirsute based on mFG scores ranging from 8 to 20.
Discussion
In this study of reproductive-aged African American women the prevalence of hirsutism using an mFG score ≥8 was 10%. Dark hair growth was most often reported as present on the upper lip, chin and lower face, stomach, below the belly button, and on the inner thighs. Women with a history of severe facial acne, physician-diagnosed PCOS, and irregular menstrual cycles were all more likely to report hirsutism than their counterparts without these conditions. As expected, 1 a large proportion of women in this cohort who did not meet the criteria for hirsutism reported being bothered by excess hair.
Our estimate of the prevalence of hirsutism falls within the range of estimates (0%–22%) reported in prior studies of mostly reproductive-aged women using an mFG of 8 as the threshold. 9,16 –19,28–31 Most of these studies used investigator-assessed mFG scores, while two used self-report. 17,31 Small studies comparing physician-assessment to patient-reported hirsutism have found higher self-reported scores, 11,32 possibly due to participant perception of the appearance of hair before removal or treatment, as these studies did not require participants to stop hair removal methods or hair reduction medications, 11 or only required discontinuation for 1 month before examination. 32
To our knowledge there have been only two other studies reporting the prevalence of hirsutism in reproductive-aged African American women in a non-PCOS selected population. The first study recruited women attending a pre-employment physical and did not investigate the potential impacts of taking a medication that might reduce excess hair growth. 29 They clinically assessed hirsutism and found that 4% of the 350 Black participants (18–29 years) had mFG scores indicating hirsutism (≥8). The second study was conducted in a cohort of women (21–45 years) trying to become pregnant who self-reported their mFG assessment. 31 Participants in prospective time-to-pregnancy studies tend to have lower fertility than the general population because women having unplanned pregnancies are not included. 33 In this study, 30% of the 364 Black/non-Hispanic participants had hirsutism (mFG ≥8). The higher prevalence of hirsutism in this compared with the current study may reflect such underlying characteristics as PCOS, irregular cycles, or concern about their fertility that may affect a woman's decision to enroll in the study. Further studies in the general population are needed to clarify both the prevalence of hirsutism in African American women and to determine the appropriate cutoff for this diagnosis given the wide-ranging estimates of hirsutism prevalence in these three studies. Data from unselected study populations from most other ethnic groups are similarly scarce. 9,16,17,28 An exception are the data from studies in East Asian populations, which consistently show hirsutism (mFG ≥8), is rare regardless of sample selection. 18 –20
The mFG is a somewhat subjective evaluation of excess hair, but it is positively correlated with elevated androgen levels in reproductive-aged women. 2,34 We found significant associations of hirsutism with acne, PCOS, and irregular menstrual cycles in this cohort. Our finding of irregular cycles being associated with hirsutism is consistent with the only other epidemiologic study that assessed this association in African American women, which also found that women with irregular cycles were more likely to report hirsutism. 31 When we defined hirsutism as the 95th percentile of mFG scores, in this cohort results were similar, although these results should be interpreted with caution given the imprecision of the estimates. Using a less restrictive definition of hirsutism (75th percentile of mFG scores) resulted in an attenuation of the associations observed in the main analysis indicating this more inclusive definition included women without hirsutism caused by existing hyperandrogenism. While associations of hirsutism with other androgen-related conditions provide data that suggest the hirsutism reported was likely to be androgen-related excess hair growth, a definitive hirsutism cutoff would require comparing scores to measured androgen concentrations, a biomarker not available in this study.
There is no standard method to assess hirsutism in epidemiologic studies, although the mFG scale (developed for clinical use) is commonly used. We found discrepancies in women's report of dark hair growth using a simple checklist question compared with the mFG assessment. This suggests that a pictorial representation provides the participant more context for answering, and we do not recommend using the checklist question to screen women for the absence of hirsutism. Importantly, 98% of the women in our sample responded to all the mFG questions suggesting that women are comfortable completing this assessment.
Being bothered by excess hair was not exclusive to women with hirsutism. Self-perceived excess hair is important because it is associated with quality of life, 32,35,36 but it probably includes hair growth in nonandrogen-dependent sites, thus not reflecting hyperandrogenemia. Current guidelines from Endocrine Society recommend treatment for women who report “patient-important” hirsutism, or hair growth that leads women to seek treatment. 1 Our data indicate that a much larger group of women report being “bothered” than have mFG scores consistent with hirsutism, and only a small group of both subsets are diagnosed with PCOS.
A strength of this study was that we assessed hair growth in a large community-based sample of young African American women. The study had little missing data, and our questionnaire allowed us to compare perceived problems with excess hair growth and the hirsutism scores. The rich covariate information allowed us to examine participant characteristics associated with hirsutism and its associations with other androgen-related conditions.
A potential limitation of this study was the use of a self-administered mFG assessment, which may have resulted in an overestimate of hirsutism. Alternatively, self-assessment could represent a more accurate assessment of facial and body hair in women who use hair removal/reduction methods or take a medication for the purpose of reducing hair growth. We did not ask about participants' use of methods to remove excess body hair or whether medications they reported were for treating excess hair growth. However, our results were essentially unchanged in analyses both including and excluding women taking a medication that could reduce excess hair growth. This is not surprising given that the vast majority of these medications reported were hormonal contraceptives, a commonly used medication among reproductive-aged women. While we did not have clinically assessed hirsutism to compare with self-reported hair growth in SELF, a recent study showed high sensitivity and specificity (81% and 80%, respectively) of women's overall report of male-like hair growth patterns when compared with clinically assessed mFG scores ≥4. 37
Conclusion
The 10% prevalence of hirsutism, using the usual cutoff of ≥8, we found in this cohort of reproductive-aged African American women, and associations of hirsutism with PCOS, severe acne, and irregular menstrual cycles, contribute important new data from a large community sample. Incorporating mFG assessments in future observational studies is likely to be highly acceptable to participants and provides an opportunity to study the epidemiology of hirsutism more broadly. Additionally, more data on the association between mFG score and androgen levels in young women of diverse ethnicities are needed to better understand the development of hirsutism and design better assessment tools.
Footnotes
Authors' Contributions
D.D.B. conceived, designed, and acquired data in the original study. H.B.C. contributed to the design of the present study, conducted the statistical analyses, and drafted the article. All authors (H.B.C., E.E.M., J.E.H., and D.D.B.) provided input on the interpretation of the data and article revisions critical for important intellectual content. All authors (H.B.C., E.E.M., J.E.H., and D.D.B.) approved the final article version for publication.
Author Disclosure Statement
All authors report no competing or personal financial interests.
Funding Information
This research was supported by the Intramural Research Program of the NIH, National Institute of Environmental Health Sciences (1ZIAES049003-30), and funds allocated for health research by the American Recovery and Reinvestment Act.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Appendix SA4
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.