
Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic has introduced acute and persistent psychosocial stressors for many individuals, with emerging gender differences that suggest women may be at greater risk for poorer mental health outcomes. This may have unintended consequences for women's overall health and well-being, including disruptions to reproductive function as elevated stress is often associated with menstrual cycle irregularities. The objective of this study was to determine if and how the COVID-19 pandemic and its related stressors have impacted women's menstrual cyclicity.
Materials and Methods:
An online survey instrument designed to capture self-reported information on menstrual cycle changes and perceived stress levels was distributed between July and August 2020. A total of 210 women between the ages of 18–45 years met stringent inclusion and exclusion criteria and completed the survey.
Results:
Of the 210 respondents, more than half (54%) reported changes in their menstrual cycles. These included changes in menstrual cycle length (50%), the duration of menses (34%), and changes in premenstrual symptoms (50%). Respondents with high perceived stress scale (PSS) scores during Covid were more likely to experience a longer duration of menses (p < 0.001) and heavier bleeding during menses (p = 0.028) compared with those with moderate Covid PSS scores.
Conclusions:
By uncovering a trend in increased menstrual cycle irregularities during the early months of the COVID-19 pandemic, this study contributes to our understanding of the implications that the pandemic may have on women's reproductive health.
Introduction
In December 2019
Intense feelings of fear, uncertainty, or anxiety related to the COVID-19 pandemic, coupled with the disruption of daily routines and behaviors spawned a global secondary mental health crisis. 5 –8 Adults in the United States who were subject to stay-at-home orders reported greater insomnia, stress, anxiety, depression, and suicidal ideation than they did before the outbreak 5 –11 and those who practiced social distancing experienced increased levels of depression and stress regardless of perceived social support and coping resources. 12,13 Women in particular have higher prevalence of anxiety, depression, and other stress-related disorders in women imparted by biological and social determinants of health. 14 –21 Therefore, the detrimental impacts of the pandemic on women's mental health may have additional unintended health consequences.
Menstrual cyclicity is an indicator of reproductive function, which is susceptible to disruptions from stress, insomnia, and depression. 22 –26 Menstrual cycle irregularities such as amenorrhea and changes in menstrual and premenstrual symptoms are often reported by women with mood disorders such as anxiety and depression, or by those facing acute life stressors. 27 –30 The female reproductive system is subject to modulating influences of stress through the interconnected nature of the hypothalamic–pituitary–gonadal (HPG) and hypothalamic–adrenal axes. 31,32 Given the influences of stress on the HPG axis, it is likely that high levels of stress experienced during the COVID-19 pandemic could alter menstrual cycle patterns and symptomology. This would parallel changes in menstrual cyclicity that women experienced after acute life stressors such as war, natural disasters, displacement, famine, and defection. 33 –37
Anecdotal reports of missed menstrual cycles or disruptions in menstrual cyclicity were reported in the popular press during the pandemic, yet limited data exist to confirm these reports. 38 –41 To address a possible association between stress during the pandemic and reproductive health, we developed a retrospective survey to assess self-reported changes in menstrual cyclicity and perceived stress levels both before and during the COVID-19 pandemic.
Materials and Methods
Survey, study participants, and recruitment
A social media-based snowball sampling strategy was utilized to distribute an online survey (Qualtrics, Provo, UT, USA) between July and August 2020. An invitation to participate in the survey using the following language, “Help us learn more about how the COVID-19 pandemic impacts women's reproductive health” was shared on the authors' social media pages and post viewers were encouraged to share the invitation within their own networks. The survey link received a total of 807 unique clicks with 46% (n = 374) received from Facebook, 31% (n = 251) from e-mail or text, 10% (n = 78) from Reddit, whereas the remaining 13% (n = 103) came from other sources.
All respondents were women who self-identified as being biologically female, between the ages of 18–45 years, and who currently reside in the United States. Exclusion criterion included (1) the current use of hormone treatments or hormonal birth control; (2) self-reported history of reproductive disorders, including but not limited to infertility, polycystic ovary syndrome, endometriosis, uterine fibroids or polyps, pelvic adhesions, pelvic inflammatory disease, or primary ovarian insufficiency; (3) pregnancy or breastfeeding within the past 12 months; and (4) self-reported history of gynecological surgery, including but not limited to hysterectomy, oophorectomy, or tubal ligation.
The survey contained 23 items and included themes such as demographics, menstrual cycle history, and self-reported levels of stress before and during the COVID-19 pandemic (Supplementary Data). Respondents reported changes in the schedule (time between menses or length of the menstrual cycle) and duration of menses (days of menstrual bleeding), menstrual flow (heavier or lighter bleeding), and intermittent bleeding (spotting). The 10-item perceived stress scale (PSS) assessment 42 was used to determine retrospective pre-Covid and Covid stress levels. Pre-Covid assessments were referred to as having occurred “prior to March 2020,” and Covid assessments explicitly referred to the months of March, April, May, and June 2020.
Data analyses
The Northwestern University Institutional Review Board deemed this study exempt from further review. Nonordinal data, including group comparisons for pre- and Covid PSS scores and self-reported menstrual cycle changes, were analyzed using nonparametric statistical analyses. Fisher's exact tests were performed using GraphPad Prism software (Version 9.0.1, La Jolla, CA, USA) to compare categorical data and Wilcoxon signed-rank tests were used to compare pre- and Covid PSS scores. p-Values <0.05 were considered significant.
Data sharing plan
Data can be provided by request from the corresponding author.
Results
Participant demographics
There were 210 individuals who met inclusion criteria and completed the survey. The majority were white (82%), non-Hispanic or Latinx (92%) individuals with an average age of 32.5 ± 5 years (Table 1). More than half (63%, n = 133) of the respondents indicated that their total household income was >$100,000. With regard to employment status, half of the respondents (50%, n = 104) indicated that they were considered nonessential employees during the COVID-19 pandemic, whereas 32% (n = 68) were considered essential employees. Respondents resided in 29 states, with the majority hailing from Illinois (40%, n = 84), California (11%, n = 24), and New York (8%, n = 17).
Respondent Demographics
SD, standard deviation.
Perceived stress throughout the Covid pandemic
Respondents completed the 10-item PSS to retrospectively evaluate pre- and Covid stress levels. The average Covid PSS scores were significantly higher compared with pre-Covid PSS scores (Mdn = 22, M = 22.0, standard error of the mean [SEM] = 0.16 vs. Mdn = 23, M = 23.4, SEM = 0.22, p < 0.0001) (Fig. 1A). Respondents' pre-Covid PSS scores revealed a distribution that skewed toward moderate stress levels, categorized by a PSS score between 14 and 26. Respondents' Covid PSS scores skewed toward the high stress category (PSS >26, Fig. 1B). Pre-Covid, 95% of respondents scored in the moderate stress range compared with 82% Covid. Respondents pre- and Covid PSS scores did not differ based on employment status; therefore, all respondents were pooled for analyses.
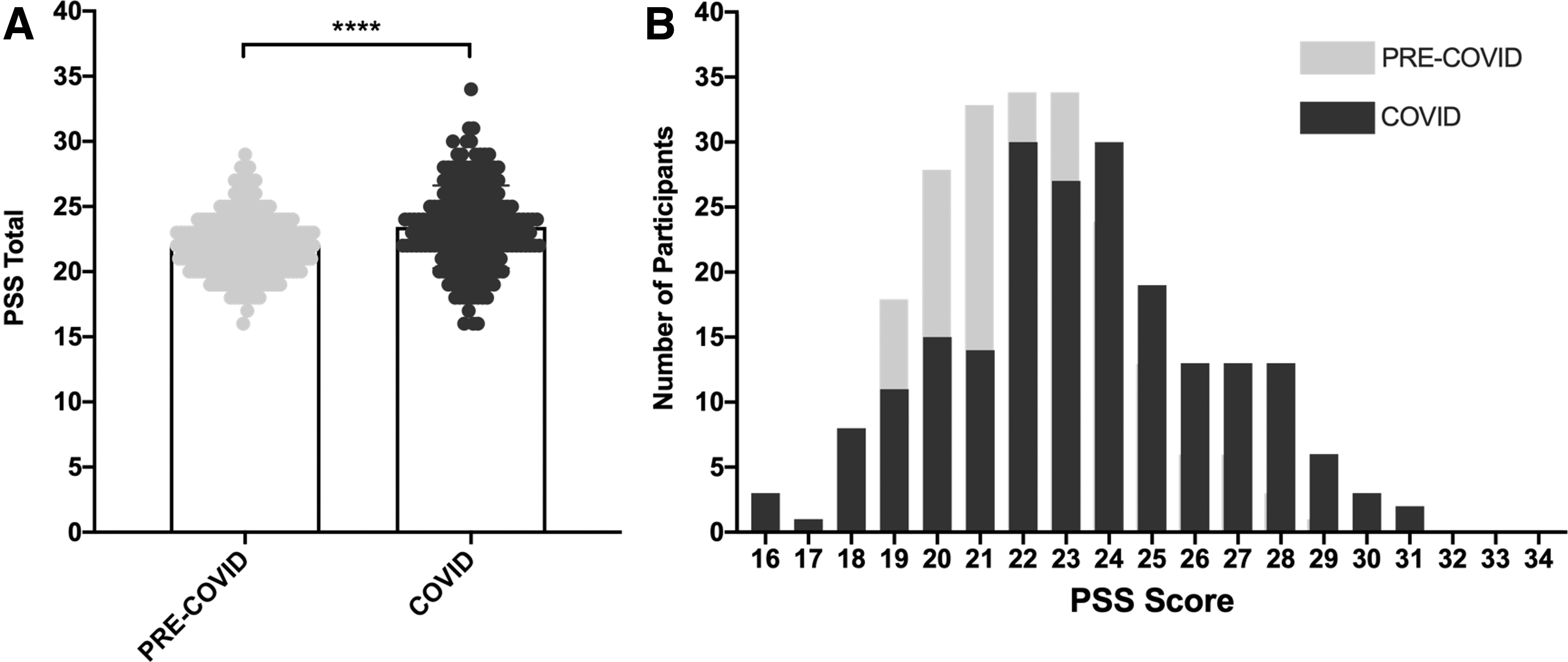
Comparison of respondents retrospective pre-Covid and Covid PSS scores.
Self-reported changes in menses
More than half of the respondents in this study indicated that they experienced one or more changes in their menstrual cycle during the pandemic (54%, n = 112) (Table 2). These included changes in the schedule of their menstrual cycle (50%, n = 106), duration of menses (34%, n = 72), and changes in premenstrual symptoms (50%, n = 104). When comparing menstrual cycle changes based on Covid PSS scores, respondents with both moderate and high scores experienced changes in the schedule of their cycle (49% vs. 58%; p = 0.371) along with changes in premenstrual symptoms (47% vs. 61%; p = 0.142). Respondents with high Covid PSS scores were significantly more likely to experience changes in the duration of menses (58% vs. 29%, p = 0.0008) and report one or more changes in menstrual bleeding (heavier and lighter bleeding, or intermittent bleeding) (71% vs. 50%, p = 0.020) compared with those with moderate Covid PSS scores. Respondents with high Covid PSS scores were also significantly more likely to report heavier bleeding (42% vs. 24%, p = 0.028).
Comparison of Self-Reported Menstrual Cycle Changes Between Moderate and High Post-Covid Perceived Stress Scale Scores
P ≥ 0.05 Not significant (ns); * P 0.01 to 0.05 Significant; ** P 0.001 to 0.01.
Discussion
Although it is well understood that increased psychosocial stress can result in menstrual cycle irregularities, this is one of the first studies to assess menstrual cycle irregularities in the context of the COVID-19 pandemic, and the first to associate such alterations with perceived stress. Our data are consistent with study by Phelan et al., which found that 46% of women self-reported an increase in menstrual cycle irregularities during the COVID-19 pandemic. 43
Given the unprecedented nature of the COVID-19 pandemic and its psychosocial impact, it is unsurprising that women in the United States may experience disruptions in menstrual cyclicity similar to other acute life stressors or natural disasters. 30,33,34,37,44 Previous investigations into the relationship between PSS scores and menstrual cyclicity found that PSS scores >20 were associated with menstrual irregularity 45 and heavy menstrual bleeding. 46 In this study, we find that women with high PSS scores (>26) experience significant disruptions to their menstrual cycle including changes in the duration of menses and heavier menstrual bleeding. More than half of the women in this study reported some change in their menstrual cycle during the COVID-19 pandemic, regardless of PSS score. This suggests that even among women who did not report significant stress related to the COVID-19 pandemic, alterations in menstrual cyclicity were common.
Interestingly, self-reported essential and nonessential employee status did not significantly impact stress scores throughout the pandemic period assessed. This may have been due to the homogeneity of the study population that consisted of predominantly wealthy white women who may have experienced similar stressors outside of their work environment. In addition, much of the current literature addressing the psychological impact of COVID-19 has focused on essential worker status and its relationship with stress. 47 –49 However, our data suggest that the impact of the pandemic on perceived stress was uniform throughout the population studied, regardless of employee status. 50,51 The similarities between PSS scores, irrespective of essential worker status, suggest that the pandemic is a shared stressor regardless of worker status.
Psychosocial stress and other mental health disorders have been associated with changes in the duration, corresponding to the number of days of menstrual bleeding, and quantity of menses that is reflected in heavier or lighter bleeding patterns. Women with self-perceived high stress jobs have reported both longer and shorter durations of menses, 52,53 whereas women who suffer from depression have separately reported longer durations of menses. 29 In this study, we find that COVID-19-related stressors may also be a contributing factor in menstrual cycle changes, as more than half of all women with high PSS scores reported a change in the duration of menses. In addition, respondents noted significant changes in menstrual bleeding during the COVID-19 pandemic. Previous studies have linked abnormal bleeding patterns and other menstrual irregularities to stress in adolescent and young adult populations, and it is reasonable to assume that stress may be contributing to alterations in menstrual bleeding patterns among adult populations as well. 50,54,55
During the COVID-19 pandemic rates of insomnia and poor sleep quality were consistently higher than pre-Covid rates. 56 –60 This may in part be due to rapidly changing responsibilities, fear of infection, social stress, and financial difficulties in the face of an uncertain future. 11,58,61 As disruptions to circadian rhythm are associated with irregular menstrual cyclicity, this also presents a potential influence on women's reproductive health. 23 Disrupted sleep patterns, as a by-product of higher levels of stress during the pandemic, could have also contributed to menstrual irregularities among our cohort. Age may also contribute to menstrual cycle variations or irregularity among women. Grieger et al. found that menstrual cycle variation is not significant between women in their 20s and early 30s, but is more common among women aged 35 years and older. 62 Although this study population ranged in age from 18 to 45 years, the average respondent was 32.5 years old and the effect of age on reporting outcomes would likely be minimal.
This survey was limited by a small U.S.-based sample and which utilized strict eligibility criteria. The survey link received a total of 807 unique clicks; however, only 210 individuals completed the screening questions designed to assess inclusion and exclusion criteria. Roughly 72% of American women utilize nonpermanent hormonal methods of contraception, which excluded a large percentage of potential respondents. 63 Strict eligibility criteria were necessary to eliminate the influence of reproductive pathologies or disorders on self-reported menstrual cycle changes in an attempt to isolate the impact of the pandemic. Likewise, we did not assess respondents' mental health history, or interrogate any pre-existing psychiatric conditions or disorders, which might contribute to or exacerbate underlying menstrual cycle irregularities. Our study population was also limited in terms of racial and ethnic diversity. Most respondents were white women, and as such we were unable to extrapolate additional information regarding the influence of race and ethnicity on menstrual cycle irregularities during the pandemic. Racial and ethnic minority populations continue to be disproportionately affected by COVID-19 due to social and structural determinants of health, racism, economic status, and health care access. 64 –66 Among women in the United States, those of racial and ethnic minority populations were more likely to experience select stressors such as food insecurity, financial hardships, homeschooling children, and lack of health care access compared with their white counterparts. 67 Inclusion of a more diverse study population would likely increase the significance of our findings. Finally, respondents were asked to complete the PSS assessment in a retrospective manner, thus the data in this study do not represent a true pre- and Covid environment and may be subject to recall bias. Typically, average PSS scores for women range between 12.67 and 13.45, which are lower than pre-Covid PSS scores reported in this study. 68 The difference in baseline level PSS scores does suggests that pre-Covid results may be influenced by recall bias. However, Covid PSS scores are similar to scores reported by studies investigating stress among the general population, health care workers, and students during the pandemic. 69 –71
Despite these limiting factors, the data presented in this study suggest that the COVID-19 pandemic may have directly contributed to menstrual cycle irregularities in women experiencing both moderate and high degrees of stress. These data affirm the experiences of women who have reported COVID-19-related menstrual cycle irregularities to health care professionals, in online forums, or through other media outlets and may stimulate a discussion among health care professionals and their patients regarding reproductive health during the COVID-19 pandemic. The association of high perceived stress and menstrual cycle irregularities is important because it supports findings that stress has downstream effects on reproductive function. 72,73 Stress due to the pandemic could potentially put women at higher risk for endocrine dysregulation. It is important for health care providers to be aware of this association because low estrogen levels can negatively impact metabolic and bone health. 74 To better understand the underlying impact of the COVID-19 pandemic on menstrual cyclicity, and more broadly on women's reproductive health, further investigation is needed. Our study identifies and highlights a critical need to assess the long-term reproductive implications of the COVID-19 pandemic.
Footnotes
Acknowledgments
The authors thank the survey respondents for their participation in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.