
Abstract
Background:
Many pregnant and postpartum Veterans have experienced multiple lifetime traumas, including military sexual trauma, intimate partner violence, and combat trauma. These women may be particularly vulnerable to increased post-traumatic stress disorder and other mental health problems following additional trauma exposures or stressful events, such as Coronavirus disease 2019 (COVID-19). This study sought to examine the impact of prior trauma exposures on the lived experience of pregnant and postpartum Veterans during the COVID-19 pandemic.
Materials and Methods:
Pregnant Veterans at 15 VA medical centers were surveyed at 20 weeks of pregnancy and 3 months postpartum asked about their COVID-19-related perinatal and mental health experiences, as well as the stressors that impacted them as a result of the COVID-19 pandemic.
Results:
Overall, 111 women Veterans completed both the pregnancy and postpartum surveys that included COVID-19 items. Sixty percent of our sample had experienced at least one potentially traumatic lifetime event, with 22% of our sample experiencing two or more of the included exposures. Women with a trauma history had 3.5 times increased odds of reporting their mental health as “much worse” compared to before the COVID-19 pandemic (95% confidence interval [CI]: 1.06–11.75) and were more likely to report that COVID-19 negatively affected their mental or emotional health “a lot” compared with women without a trauma history (odds ratio: 8.5; 95% CI: 1.93–37.48).
Conclusions:
COVID-19 has had a significant impact on pregnant and postpartum Veterans' mental health. Obstetricians should consider strategies to ensure women have access to mental health care during pregnancy, especially as the COVID-19 pandemic continues. Hospitals should also consider the importance of labor support companions during the COVID-19 pandemic and examine adjusting policies to allow for at least one labor support companion during labor and delivery.
Introduction
Coronavirus disease 2019
The COVID-19 pandemic has also led to widespread lockdowns and social distancing, resulting in social isolation, job loss, and other significant patient disruptions in everyday life. Along with these stressors, pregnant women have experienced disrupted prenatal care during the pandemic. COVID-19 has given rise to a greater reliance on obstetric telehealth as a means of reducing patient and provider exposure to COVID-19. 2 Recent studies of changes in prenatal care during COVID-19 have examined system-wide changes in care guidelines for frequency of prenatal visits, ultrasound examinations, and antepartum testing, as well as labor and delivery guidelines. 3 Although research suggests general provider acceptance of obstetric telehealth, 4 several studies indicate pregnant women are less accepting of the practice, 5 with concerns about fetal development and privacy for telehealth visits. 6
Changes in COVID-19 prenatal care and labor and delivery practices, in addition to stressors related to the COVID-19 pandemic such as fear of infection, loss of income, and social distancing, may lead to poorer mental health among pregnant and postpartum women. Recent studies have revealed significant increases in pregnant women's levels of anxiety and depression symptoms during the COVID-19 pandemic, 7,8 with generalized anxiety rates during pregnancy in the range of 63%–68%. 9,10 Other studies have examined women's perceptions and fears related to pregnancy during the COVID-19 pandemic and found women's worries were related to changes in delivery practices and altered social support during pregnancy. 11 Key social determinants of health, 12 including employment, food security, housing, financial strain, and social support have also likely been disrupted due to COVID-19, 13,14 thereby negatively impacting women's mental health during this time. 15
Previous traumatic life events may give rise to additional coping challenges during COVID-19 for some pregnant women. Research suggests that individuals with post-traumatic stress disorder (PTSD) from prior trauma(s) are particularly vulnerable to increased PTSD and other mental health problems following additional trauma exposures or stressful events. 16,17 Women Veterans in particular may be at risk to coping challenges during COVID-19, due in part, to military-related roles and experiences that portend risk for trauma exposure. Although a policy allowing women to formally serve in combat roles was not implemented until 2016, the wars in Iraq and Afghanistan blurred the lines between combat and non-combat roles, and women served in a variety of positions that put them at risk for injury and death, including combat trauma. 18 For example, Street et al. found in their national survey of post-9/11 veterans that 73% of women reported one or more combat experiences. 19
Combat experiences are not the only traumatic events that women Veterans experience. Interpersonal violence during and following military service are all-too-common experiences in the lives of women Veterans. Experiences of sexual harassment and assault during military services, referred to as military sexual trauma (MST), are prevalent, 20 with recent estimates suggesting that 44% of women deployed to combat zones experiencing sexual harassment and 10% experiencing sexual assault. 21 In addition to MST, intimate partner violence (IPV), defined as psychological, physical, or sexual aggression by a current or former intimate partner, is another common form of trauma women Veterans experience. 22,23 A recent telephone survey of a nationally representative sample of women Veterans who use VA primary care found that 18.5% reported past-year psychological, sexual, and/or physical IPV. 24
To examine the impact of prior trauma exposures and available social support on the perinatal care and mental health care experiences of pregnant and postpartum Veterans during the COVID-19 pandemic, we surveyed a racially diverse sample of women Veterans who were identified as pregnant within the Department of Veterans Affairs (VA), but received community-based obstetrical care, and thus were affected by changes in maternity guidelines and practices at obstetrics providers across the Unites States.
Materials and Methods
Participants and recruitment
This mixed-methods study was conducted under the auspices of the Center for Maternal and Infant Outcomes Research in Translation (COMFORT) and described in detail previously. 25,26 Pregnant Veterans at 15 VA medical centers were identified by local VA study teams based on their local procedures, for example, when a pregnancy consult was placed in the electronic medical record by the Veteran's provider. Recruitment was initiated with mailed invitation packets, including an introductory letter describing the study, and followed by research team telephone calls to potential participants. We conducted telephone surveys (∼45 minutes in length) with women Veterans at 20 weeks of pregnancy and 3 months postpartum. All survey data were collected using Research Electronic Data Capture (REDCap), a secure web-based application designed to support data capture for research studies. 27 Participants were given US$25 in the form of gift cards for completing each study interview. COMFORT was approved by the Veterans Administration Central Institutional Review Board.
Data collection
Questions related to the COVID-19 pandemic were added to our prenatal and postpartum surveys in March 2020 to better understand the challenges pregnant and postpartum women experienced during COVID-19 (Fig. 1). The COVID-19 questions were developed by our study team in collaboration with other VA colleagues to understand the impact of COVID-19 on mental health functioning. Overall, 356 women completed the prenatal, postpartum, or both prenatal and postpartum surveys. However, to understand the impact of previous trauma on response to COVID-19 throughout the pregnancy and into postpartum and to compare within participant over time, we only included participants who completed both prenatal and postpartum interviews between March 2020 and March 2021 (n = 111). A detailed description of how we arrived at the final study cohort included in this analysis can be found in Figure 2.
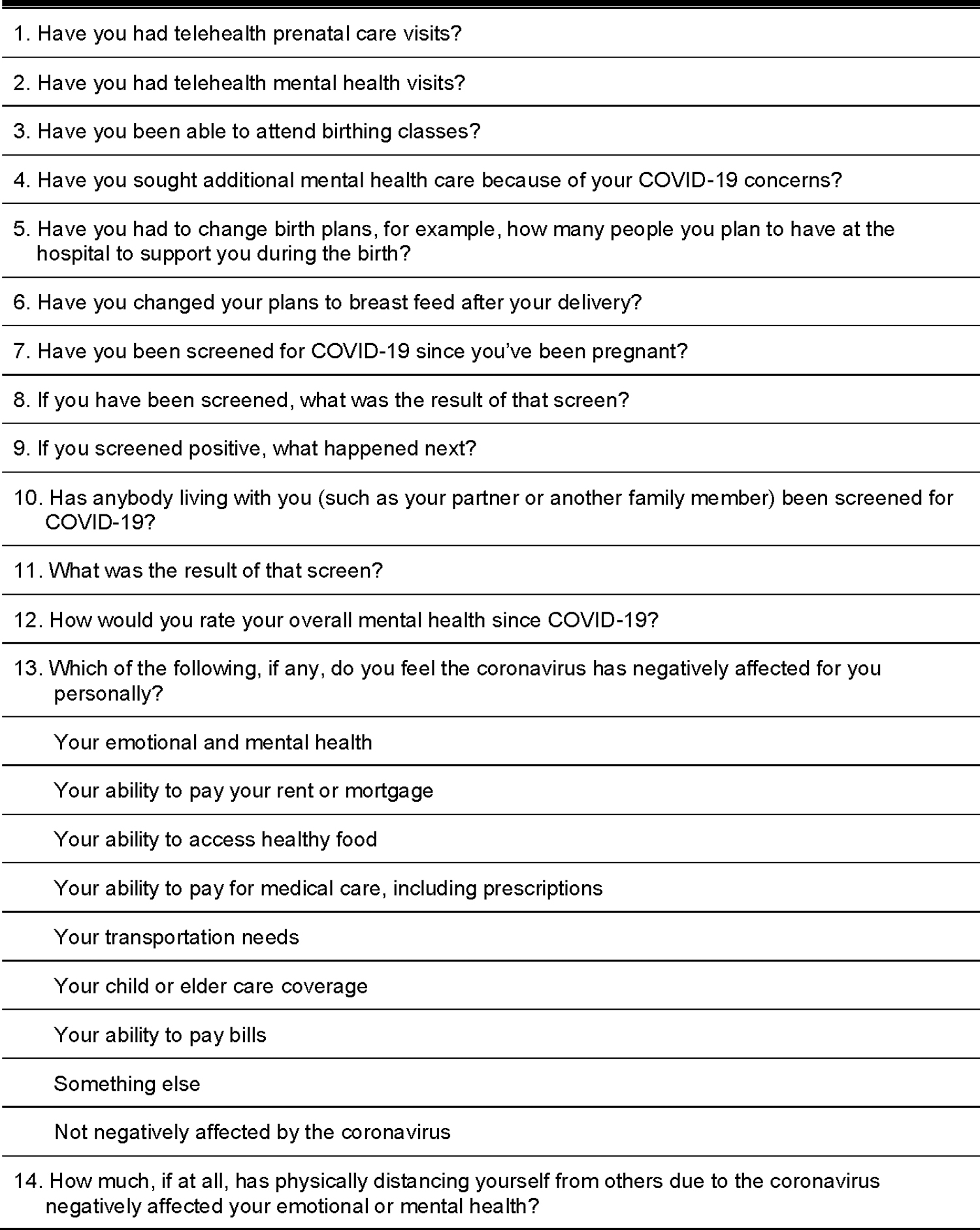
COMFORT COVID Questions. COMFORT, Center for Maternal and Infant Outcomes Research in Translation; COVID, coronavirus disease.
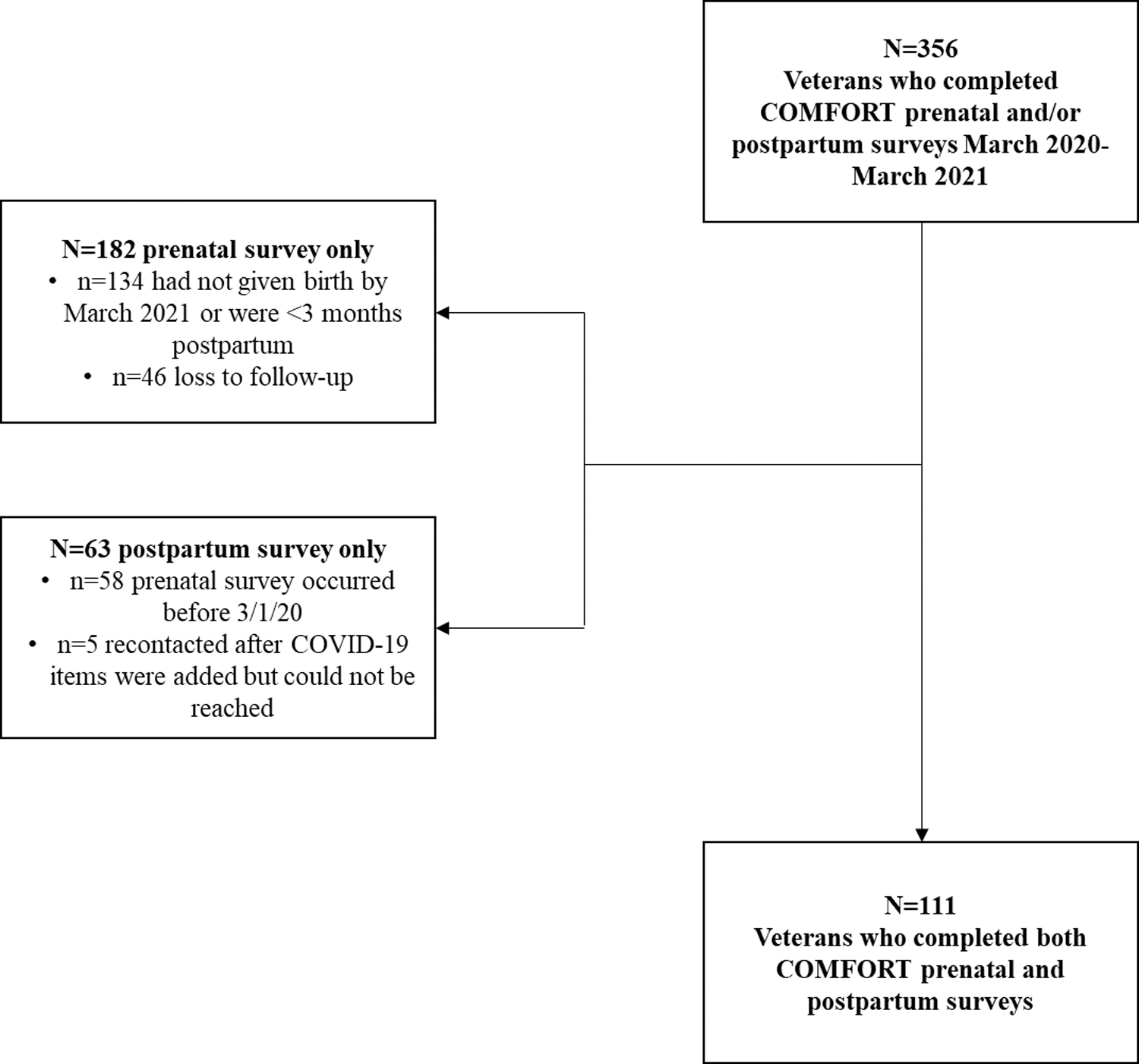
Participant flowchart.
Measures
We measured three types of trauma: recent history of IPV, history of MST, and history of combat exposure (yes/no). Recent IPV was measured using the Extended Hurt/Insult/Threaten/Scream (E-HITS) screening tool, which includes five items assessing IPV behaviors by a current or past partner in the past 12 months: physically hurt you, insulted you, threatened to harm you, screamed or cursed at you, forced you to have sexual activities. 28,29 Responses are scored on a five-point scale from 1 (“never”) to 5 (“frequently”) and summed for a total score (range: 5–25). A score of 7 or higher indicates a positive IPV screen, based on previous research with women Vetearns. 27 The MST questions were adapted from the VAs universal MST screening questions described in previous work 20 and assessed whether Veterans reported experience of MST (defined as sexual harassment and/or assault during military experience).
The Deployment Risk and Resilience Inventory-2, Section D (Combat Experiences), includes 17 items that ask about combat experience during the most recent deployment. Examples of items include, “During deployment, I was exposed to incoming fire” and “During deployment, I personally witnessed civilians being seriously wounded or killed.” Responses range from 1 (“Never”) to 6 (“Daily or almost daily”). 30 Guided by past analyses, 19 we utilized a liberal definition to define combat experience, where if any item on the scale was rated affirmatively (“2” or higher), we considered this as indicative of combat exposure during deployment. We defined women as experiencing “any trauma” if they reported any combat experience, past-year IPV, or MST.
We also asked about demographics, military, and pregnancy characteristics, as well as several key social determinants of health during COVID-19, including ability to pay bills, rent, or mortgage, ability to maintain a job, ability to access healthy food, and child or elder care coverage. Additionally, participants self-reported if they had ever been diagnosed with anxiety, PTSD, depression, or postpartum depression. We also prospectively measured depression symptoms with the Edinburgh Postnatal Depression Scale (EPDS) at both prenatal and postpartum time points. The EPDS is a validated screening tool for use in a perinatal population with a score of ≥10 determined to be an optimal cutoff point for detecting depression symptoms. 31
Quantitative analysis
To characterize our sample, we used chi-squared and Fisher's exact tests with categorical data and Student's t-tests (with the Satterthwaite adjustments when necessary) with continuous data. We then compared responses between the prenatal and postpartum time points using McNemar's tests for matched pairs, which tested the concordance between responses, and identified changes that were statistically significant. These comparisons included telehealth visits, ability to attend birthing classes, changes to birthing plans, mental health, and social determinants of health during COVID-19. To account for multiple comparisons, we used a Bonferroni-adjusted alpha of p < 0.002 to denote significant changes.
To examine whether changes to these responses over time differed for trauma groups, we utilized generalized estimating equations with a nonlinear link function via PROC GENMOD in SAS v.9.2 for binary outcomes. 32 This strategy accounts for repeated responses from participants at both the prenatal and postpartum survey time points by modeling correlated outcome data. An unstructured correlation structure was specified. We report odds ratios (ORs) and 95% confidence intervals (95% CIs) from models adjusted for timing of response (pregnancy or postpartum), first pregnancy (yes or no), history of mental health conditions (self-reported depression, anxiety, and/or PTSD), age at delivery, and race (white race vs. not white race). All statistical analyses were conducted in SAS version 9.2 (SAS Institute, Inc., Cary, NC, USA).
Qualitative analysis
An inductive approach to qualitative content analysis was used to analyze response to the following open-ended question: “What COVID-19 stressors did you experience in the way you received pregnancy or mental health care or the care you received during labor and delivery?” For each response, themes were generated for the words and phrases expressed by the respondents. Themes were then coded using a set of mutually exclusive categories (e.g., concepts). We then assessed frequency of each concept. Conceptual content analysis was completed by two coders and verified by a third coder. Any discrepancies in concepts or concept coding were discussed among the coders and the final coding was reached via consensus. Qualitative data was managed in the ATLAS.ti qualitative analysis software. 33
Results
Among the 111 Veterans who completed both the pregnancy and postpartum surveys, more than half (60%) were women of color. The majority of women (92%) were married or lived with a partner, and for 28% of respondents, this was their first pregnancy. Almost all women (96%) had received assistance from a VA maternity care coordinator during their pregnancy. Eighty-two percent received their first prenatal care visit during the first trimester of pregnancy. Nearly half of the study population had a history of mental health problems, with 50%, 45%, and 40% of our sample reporting a past diagnosis of anxiety, depression, and PTSD, respectively. Fifteen percent of the study population had a prenatal EPDS score greater or equal to 10, indicating depression symptoms, whereas nearly 10% of the women in the study had a postnatal EPDS greater than or equal to 10 (Table 1).
Demographics, Pregnancy Characteristics, and Mental Health and Trauma History (n = 111)
Other race includes participants who identified as races other than the categories listed here.
EPDS, Edinburgh Postnatal Depression Scale; IPV, intimate partner violence; MH, mental health; MST, military sexual trauma; PTSD, post-traumatic stress disorder; SD, standard deviation; VA, Veterans Affairs.
A substantial number of women had a history of trauma, with nearly 50% of women reporting a history of MST. Seven percent of women had an E-HITS score of 7 or greater, indicating IPV in the past year. More than one quarter of women (27.9%) had experienced some form of combat-related exposure (Table 1). Taken together, 60% of our sample had experienced at least one potentially traumatic event, with 22% of our sample experiencing two or more of the included exposures (18.9% combat experiences and MST; 2.7% IPV and MST). Women with a potential trauma history were more likely to be of Hispanic/Latino origin (30.3% vs. 11.1%, p = 0.02), have a history of anxiety (57.6% vs. 37.8%), a history of PTSD (62.1% vs. 8.9%, p < 0.0001), and to have used VA mental health care during pregnancy (57.7% vs. 21.6%, p = 0.001) compared with women without any trauma history. Trauma history did not differ based on any other demographic variable we examined (e.g., marital status, race, age; data not shown).
When examining changes in health practices and beliefs related to COVID-19 between pregnancy and postpartum, women reported significant changes in birth plans over the course of pregnancy, with nearly half of all women reporting a change in birth plans following pregnancy compared with reports during pregnancy (49.5% vs. 27%, p < 0.0001). COVID-19 screening increased over time, as more women reported that they were screened by the postpartum interview compared with during the pregnancy interview (89.2% vs. 14.4%, p < 0.0001), likely due to increased screening at labor and delivery. Overall, although not statistically significant once adjusted for multiple comparisons, women reported that their overall mental health was worse than before COVID-19 following their pregnancy (32% vs. 22.5%, p = 0.04; Table 2).
COVID-Specific Questions, by Time (n = 111)
p-Values from McNemar tests for matched pairs, testing the concordance between responses (p < 0.002 responses indicate that the change in the proportion of responses to each item from prenatal to postpartum is statistically significantly different, adjusted for multiple comparisons using the Bonferroni correction).
Compares responses combined as “A lot” versus “Some/a little/not at all.”
COVID-19, coronavirus disease 2019.
Among the social determinants of health items, fewer women worried about their ability to pay rent following pregnancy than during pregnancy (1.8% vs. 11.7%, p = 0.01). Conversely, women worried much more about their ability to pay bills following pregnancy rather than during pregnancy (30.6% vs. 16.2%, p = 0.001).
Our models examining the association between trauma history and health care experiences during COVID-19 indicated that women who had experienced a past trauma were more likely to rate their mental health worse than women without a trauma history. Women with a trauma history had 3.5 times increased odds of reporting their mental health as “much worse” compared to before the COVID-19 pandemic (95% CI: 1.06–11.75). Similarly, women with a trauma history reported that physical distancing measures due to COVID-19 were more likely to negatively affect their mental or emotional health “a lot” compared with women without a trauma history (OR: 8.5; 95% CI: 1.93–37.48; Table 3).
Trauma History Association with COVID Variables Over Time
All results are for trauma history versus no trauma history from generalized estimating equation models. Models are adjusted for timing of response (pregnancy or postpartum), first pregnancy (yes or no), history of mental health conditions (self-reported depression, anxiety, and/or PTSD), age at delivery, and race (white race vs. not white race). Trauma history is defined as women with an E-HITS score 7+ (indicates past year IPV), any reported MST, or any combat stressor, as measured by the Combat Experiences Scale on the Deployment Risk and Resilience Inventory (CES-DRRI). Each row of estimates is a separate model with the dependent variable as listed. Transportation needs could not be estimated due to no affirmative responses in the postpartum time period.
p-Values are from the overall type 3 test that investigated a difference between the independent variable (history of trauma) adjusted for timing of response (pregnancy or postpartum).
DV, dependent variable; LCI, lower confidence interval; OR, odds ratio; UCI, upper confidence interval.
Thematic analysis of postpartum women's responses regarding COVID-19 challenges
Women Veterans characterized their pregnancy-related stressors during COVID-19 into two major categories: (1) Limited social support during labor and delivery (endorsed by more than 50% of the sample) and (2) Dissatisfaction with virtual prenatal care visits (endorsed by 12% of the sample). We briefly describe these two major areas of stressors below.
Limited social support during labor and delivery
More than 50% of all participants reported that the largest pregnancy-related stressor during COVID-19 was the limited social support women experienced during labor and delivery as a result of COVID-19 hospital policies limiting the number of visitors. Many women had wanted a spouse/partner, a parent, or a doula in the hospital with them when they delivered, but most women were only allowed one person. In some cases, this precluded the use of a doula, as noted by a 32-year-old Veteran:
We really wanted to have a doula assist with labor but they only allowed one person in the room so we couldn't have a doula.
Three of the women we interviewed were not allowed to have anybody with them during labor and delivery, as noted by this 39-year-old Veteran from Dallas:
My partner was not allowed in the delivery room at all. They only let him come in after my C-section was finished.
One woman (aged 26 years) had an emergency delivery and did not get to have her husband with her in the hospital:
Since my delivery was an emergency, my aunt took me to the hospital and got me checked in, because my husband was at work. Since no one was allowed to leave and come back, my aunt had to stay while I delivered and my husband was not permitted to come in.
One Veteran (aged 38 years) described the reason she delivered in a hospital by herself:
My partner could not be there during labor and delivery because the hospital would not allow children in the hospital and we had nobody else to care for our other child.
Other women had to change their birth plans entirely, including the location of their delivery from a birthing center to a hospital, as described by this 36-year-old Boston Veteran:
I had planned to deliver in a birthing center, but it was closed due to COVID-19, so I had to deliver in the hospital instead. My partner was the only one allowed in the hospital with me.
Another woman from Los Angeles spoke of the dual stress of wearing a mask while delivering her baby and having limited birth support:
I had to wear mask during pushing even though my COVID-19 test was negative. Also, I could only have one person, no visitors or even a doula was allowed.
Dissatisfaction with virtual prenatal care visits
The other major source of stressors during COVID-19 was dissatisfaction with virtual prenatal health care. Overall, 12% of respondents expressed dissatisfaction with virtual prenatal care or mental health visits.
One pregnant Veteran from Boston (aged 27 years) noted:
The virtual prenatal care experience was not satisfying. I was not able to hear the infant's heartbeat and they couldn't take measurements of the baby.
Another pregnant Veteran from Dallas (aged 33 years) noted similar problems:
The prenatal telehealth experience was a waste of time. We had technology issues with connecting on both ends and I feel like I have been cheated in this pregnancy.
A third Veteran from Dallas (aged 30 years) shared the following:
Prenatal telehealth was alright, but it was even more brief than face to face. I probably should have sought additional mental health (care) but didn't. It feels like my gestational diabetes is from stress-eating due to COVID.
Discussion
To the best of our knowledge, this is the first article to examine pregnant women Veterans' experiences of perinatal care and mental health during the COVID-19 pandemic, and the first study to demonstrate a differential impact of COVID-19 on pregnant women with and without lifetime trauma. Our study suggests that pregnant women with a history of trauma in the form of combat experiences, MST, and/or IPV faced elevated pandemic-level stress. Veterans in our study had significant histories of combat and MST, in addition to IPV, with these traumas giving rise to poorer self-ratings of mental health during the perinatal period.
Previous studies of pandemic-related stress among pregnant women found that stress associated with feeling unprepared for birth due to COVID-19 and stress related to fears of perinatal COVID-19 infection were major factors in women's elevated pandemic-related stress responses. 15 Our study contributes to this literature by demonstrating that previous traumatic experiences further factor into pregnant and postpartum women's overall ability to cope with COVID-19 during pregnancy.
The finding that women's trauma history contributes to poorer mental health during the perinatal period is important, in that women Veterans are a population that often experience various types of physical, sexual, and psychological trauma exposures before, during, and following military service. 34 Past research has shown that individuals who develop PTSD caused by such traumas are more likely to report elevated stress symptoms following future trauma exposure. Although this study did not obtain information on the PTSD response to these prior traumas, given the strong associations documented in the literature between each of these types of trauma and PTSD, 19,35 along with the finding that the majority of trauma-exposed participants reported a history of PTSD, it is possible that post-traumatic stress symptoms reduced internal resources and resilience in the context of persistent stress 36 during the pandemic. In addition, past trauma experiences may cause or exacerbate difficulties in the ability to cope effectively with pandemic-related stressors (e.g., physical distancing), thereby increasing psychological distress.
Women identified limited social support during labor and delivery, as well as changes in birth plans, as major sources of pandemic-related stress. Our study is consistent with previous COVID-19 studies that have demonstrated the challenges associated with limited birthing supports. 37 In response to COVID-19, hospitals have largely eliminated visitors in inpatient settings. Current recommendations advise health care facilities that only visitors essential for patients' “physical or emotional well-being and care” are permitted. Exceptions to this rule have been made for labor and delivery, end-of-life care, and pediatric intensive care. 38 “Minimum necessary” visitors are recommended in labor and delivery settings, generally translating to one visitor. 39
These policies may have potential disproportionate burdens among women of color, who are more likely than white women to have previously received birthing support through doulas, and to desire it for future pregnancies. Support persons during labor have been shown to be particularly important among low-income Black and Latina women with evidence of lower rates of cesarean birth, increased breastfeeding initiation, and longer duration of breastfeeding 40 –42 with doula support. Given existing evidence demonstrating disproportionate rates of maternal morbidity and mortality among pregnant women of color, 43,44 the presence of support persons for women of color is critically important, particularly as women struggle with mental health issues related to COVID-19.
Echoing previous studies, pregnant and postpartum women's self-assessed mental health declined as a result of COVID-19. Women's overall mental health, as measured by self-rated mental health since the onset of the COVID-19 pandemic, significantly worsened during the perinatal period. Women's concerns regarding money, including the ability to pay rent and bills, are reflective of national trends in unemployment during COVID-19, with 20% of Hispanic or Latino women and 19% of Black women losing their jobs during COVID-19, which are the highest rates of job loss among all race, ethnicity, and gender groups. 45 We did not assess whether women or their partners lost their jobs during the COVID-19 pandemic, but the concerns that women of color expressed related to financial security suggest that social determinants of health, such as economic security, are greatly impacting women's mental health.
Another challenge experienced by women in our study was the shift to virtual prenatal and mental health care. Overall, ∼32% of pregnant and postpartum respondents reported receiving virtual prenatal care during their pregnancies, while roughly 38% received virtual mental health care. Recent studies have demonstrated that telemedicine results in similar outcomes and increased patient satisfaction for low-risk pregnancies and improves access to subspecialty care for those living in underserved areas. 46,47 However, women in our study reported dissatisfaction with their telehealth experiences, particularly in prenatal care.
Veterans spoke of the challenges with technology (e.g., confusing instructions regarding how to log-on), disappointment with the quality of information exchanged during the visit (e.g., not being able to hear the baby's heartbeat or do measurements of the fetus), and feeling rushed during the visit. Moving forward, health care providers and their support staff should ensure women have adequate access to telemedicine, including consistent access to the internet and assistance with logging in. Providers may also need to engage women Veterans in conversations regarding how to cope with pandemic-related stress, and refer Veterans to counseling services, virtual support groups, and consistently screen pregnant women for depression.
There are several important limitations to our study. First, the women Veterans in our study may be different from other pregnant women in that they had access to a VA maternity care coordinator who helped them with questions regarding pregnancy during COVID-19. Our analysis shows that nearly 100% of pregnant and postpartum women worked with a VA maternity care coordinator, and this may have resulted in improved pregnancy perceptions and experiences among this cohort of women compared with the general population who did not have a pregnancy care coordinator with whom to work. Second, because this study focused on women Veterans, who often have significant histories of combat and interpersonal trauma exposure, 34,48 and concomitant mental health comorbidities, 26,49 our findings, particularly in terms of deteriorating mental health during pregnancy, may not be representative of the larger population of pregnant and postpartum women.
Another limitation was the limited qualitative findings that arose from this study, thereby limiting our ability to understand the full extent of women's experiences with labor/delivery during pregnancy. Finally, our assessment of trauma exposures was limited to three prevalent types of trauma that are commonly experienced by women Veterans. As noted previously, women Veterans often experience other traumas as well, including physical and sexual abuse in childhood and lifetime IPV experiences. A more comprehensive assessment of trauma (and PTSD) should be examined in future research.
Conclusions
Our study has important implications. First, COVID-19 has had a significant impact on pregnant and postpartum women's mental health. Obstetricians should consider strategies to ensure women have access to mental health care during pregnancy, especially as the COVID-19 pandemic continues. Second, the current findings reinforce the importance of obstetricians, family planning providers, and maternity care coordinators providing trauma-informed care. This includes being knowledgeable of the substantial prevalence and pervasive impact of military and non-military traumas on pregnant women's health and associated health needs. Third, women may experience important challenges related to social determinants of health, including childcare, finances, and other needs.
Obstetricians and mental health providers should address these issues during prenatal and postpartum care visits, and work with women to identify resources and strategies to address problems related to social determinants of health. Finally, hospitals should consider the importance of labor support companions during the COVID-19 pandemic and examine adjusting policies to allow for at least one labor support companion during labor and delivery. Improved COVID-19 testing policies and strategies should be used to ensure women are not alone during labor and delivery.
Footnotes
Author Disclosure Statement
This is original research that has not previously been presented or published elsewhere. All authors of this article have met each of the requirements for authorship as stated in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals. No authors have any conflicts of interest with this work. The opinions expressed here are those of the authors and do not represent the official policy or position of the U.S. Department of Veterans Affairs.
Funding Information
This study was funded by the Department of Veterans Affairs Health Services Research and Development: IIR13–81.