
Abstract
Objectives:
Oral health is an integral part of women's health, yet many women face barriers and go without necessary dental care. The objectives of this study were to (1) examine and compare pregnancy-related oral health knowledge and barriers to dental care access during pregnancy among women with private and public insurance and (2) estimate awareness of available Medicaid pregnancy dental benefit among Medicaid-enrolled women and explore associated factors.
Methods:
A cross-sectional survey was administered to a convenience sample of 21- to 45-year-old women (n = 187) visiting a large urban academic health center in Virginia. Data on pregnancy-related oral health knowledge, barriers to dental care access, Medicaid dental benefit awareness, health insurance, socio-demographics, health information source, and last dental visit were collected. Chi-square tests, t-tests, and multivariable regression were used to examine associations at p ≤ 0.05.
Results:
More than half of the women reported private insurance (52.4%), 40.3% reported Medicaid, and 8.3% reported being uninsured. Medicaid-enrolled women reported a lower prevalence of a routine dental checkup in the past year (44% vs. 71%, p = 0.002), lower knowledge scores (2.9 vs. 3.6, p < 0.001), and more barriers to accessing dental care during pregnancy compared with privately insured women. One in every three Medicaid-enrolled women (34%) was unaware of the Medicaid pregnancy dental benefit. Benefit awareness was associated with the receipt of health information from a health care source (p = 0.030) and a high oral health knowledge score (p = 0.018).
Conclusions:
There was a significant gap in dental care use and knowledge between Medicaid-enrolled and private-insured women in our study sample. Targeted programs should be developed to educate women about the importance of oral health and share information about available Medicaid dental coverage to reduce barriers to dental care during pregnancy.
Introduction
Oral health is essential throughout a woman's life, and particularly during pregnancy. However, many women in the United States often go without necessary dental care. 1 Use of dental services during pregnancy is safe, effective, and unanimously endorsed by professional associations. 2,3 Yet, only 47% of women in Virginia had a dental visit during pregnancy. 4
There are substantial disparities in dental care use and unmet dental needs by income among pregnant women. 5 According to 2015 Virginia pregnancy surveillance data, only 42.4% of non-Hispanic Blacks and 40% of Hispanics had a dental cleaning dental visit during pregnancy compared with 51% of non-Hispanic White women. Medicaid-enrolled women were half as likely to visit the dentist during pregnancy than their private-insured counterparts (25% vs. 59%). 5 A similar trend in oral health utilization has been seen among pregnant women in the previous years too. In March 2015, to improve access to dental care among low-income pregnant women and reduce oral health disparities, Virginia implemented comprehensive dental benefit coverage for pregnant women aged 21 years and older enrolled in Medicaid. 6 Before this, dental services available to these women were limited to emergency dental extractions. The new pregnancy dental benefit was advertised and promoted through the state Medicaid program and through the dental benefits administrator. The information was shared with all pregnant enrollees and both dental and medical providers.
Although the dental coverage provided was comprehensive, early years of data did not show high uptake of dental services by pregnant women. 7 It was estimated that the new dental coverage would be available to and impact ∼45,000 women, but during 2015–2017, 10,395 women utilized the benefit. 8 Various factors can affect the translation of coverage to the utilization of services, including the beneficiaries' awareness of available coverage and services, demand and/or need for services, and health care knowledge. 2,9 To understand these information gaps, this study explored differences in pregnancy-related oral health knowledge and barriers to dental care among reproductive-aged women by health insurance type among women attending a large academic center. The second objective estimated the awareness of the available Medicaid Pregnancy Dental coverage among Medicaid-enrolled women and identified associated factors.
Methods
Study participants
This cross-sectional study included a convenience sample of women visiting an urban academic health center in Virginia between October 2017 and May 2018. The study was approved by the Virginia Commonwealth University's Institutional Review Board. Women were eligible to participate in the study if they were 21–45 years old and a mother to a child or currently pregnant. Participants were recruited by displaying study flyers in the waiting area of the pregnancy clinic and the dental clinic. The eligible participants were given an information sheet explaining the study and asked to complete a paper/pencil questionnaire in the clinic's waiting area after verbal consent. An oral hygiene kit was given as a token of appreciation for the participant's time.
Survey questionnaire and variables
The survey was developed by adapting the questions from previous studies and was available in English and Spanish language. 10,11 The survey consisted of demographics questions (age, education, and race/ethnicity), health insurance type (private, Medicaid/FAMIS, or no insurance), pregnancy status (yes/no), number of children, age of the youngest child, pregnancy-related oral health knowledge, barriers to accessing dental care during pregnancy, last routine dental visit in years (<1, 1–2, 3 to 5, and >5), a primary source of oral health information (friends/family, social media, health clinics, and other), and awareness of Medicaid pregnancy dental coverage (yes/no). We will refer to this variable as dental coverage awareness from hereon.
Pregnancy-related oral health knowledge measures (hereon referred to as knowledge) included four questions, and barriers measure included five questions. Possible responses were “yes, no, and not sure.” For analyses, “no” and “not sure” responses were combined. The knowledge score was constructed by summing the number of correct answers. Sources of oral health information were later condensed into two categories: family/friends and social media as “Social” and health care clinics and any free text responses that referenced health care as “Healthcare.”
Statistical analysis
Descriptive and bivariate analyses were performed to determine sample characteristics and associations between insurance type and demographics, knowledge, and barriers. Categorical variables were tested using Fisher's exact test or chi-squared test of association (as sample size dictated), and a two-sample t-test was used for continuous variables. Exploratory multivariable logistic regression was used to assess factors associated with dental coverage awareness among Medicaid-enrolled women. The model included sociodemographic factors (age, race, number of children, and education) and oral health knowledge, last year dental checkup, source of health information, and pregnancy status. Results were considered significant for p < 0.05. Data analysis was carried out using SAS EG v.6.1.
Results
The survey was administered to n = 187 women aged 21–45 years. The median age of the youngest child was 2.5 years with an interquartile range of 0.8–7.0. Two women did not complete the vast majority of the questions, and their data were excluded. Of the remaining 185, 4 women did not respond to the insurance question. The maximum missing number of responses for any included variable was 5. Table 1 provides the sample distribution.
Sample Characteristics by Type of Health Insurance
SD, standard deviation.
When compared by health insurance type, Medicaid-enrolled women were younger (29.2 years), Black/African American race (78%), had high school education (53%) compared with women with private insurance or no insurance. Dental utilization differed by insurance type; 90% of women with private insurance had a routine checkup in the last 2 years compared with 77% among Medicaid-enrolled women and 67% among women without insurance. Compared with 37% of privately insured women, 55% of Medicaid-enrolled and 60% of uninsured women reported health clinics as their health information source. Overall, 33% of women reported “other” as their health information source. Some of the responses listed in the other category included their individual dental provider, internet searches, and a combination of sources. All characteristics were significantly associated with the health insurance type (Table 1).
There were also significant differences in women's knowledge and barriers based on insurance type. The overall knowledge score among women with private insurance was 3.6 of 5 (standard deviation [SD] = 0.71) compared with 2.9 (SD = 1.11) in Medicaid-enrolled women and 3.2 (SD = 1.21) in uninsured women (p < 0.0001). The correct response rate ranged between 59% and 99% for all five questions. The question with the lowest correct response rate was, “Can pregnancy make women more susceptible to dental disease?” Overall, 70% of the participants answered correctly, 80% of privately insured compared with only 67% of uninsured and 59% of Medicaid-enrolled women (p = 0.0476). There were also significant differences in the percent responding correctly for the items “Is oral health linked with general health?” (p = 0.0004) and “During pregnancy, is it safe to get routine dental care such as checkups and cleanings?” (p = 0.0001). For both questions, women with private insurance had a higher percentage of the correct answer (99% and 97%, respectively). No significant difference by insurance type was observed for, “Can teeth/gum disease have a negative impact on pregnancy?” Responses ranged between 73% and 87% (Fig. 1).

Pregnancy-related oral health knowledge by health insurance. p-value from Fisher's exact test comparing three insurance types. Overall percent was not included in the test but is reported for visual comparison only. Error bars represent 95% confidence intervals.
Responses to five barriers to accessing dental care during pregnancy differed widely and significantly by insurance type (p < 0.0001). Compared with women with private insurance, Medicaid-enrolled were two to three times, and uninsured were three to five times more likely to report financial barriers or lack of dental insurance. Nearly a third of Medicaid-enrolled and uninsured women reported safety concerns regarding dental care during pregnancy compared with 8% with private insurance. Inability to find a dentist/dental office that would treat pregnant women or take Medicaid insurance was 15%–20% among Medicaid-enrolled compared with 0%–1% among women with private insurance (Fig. 2).
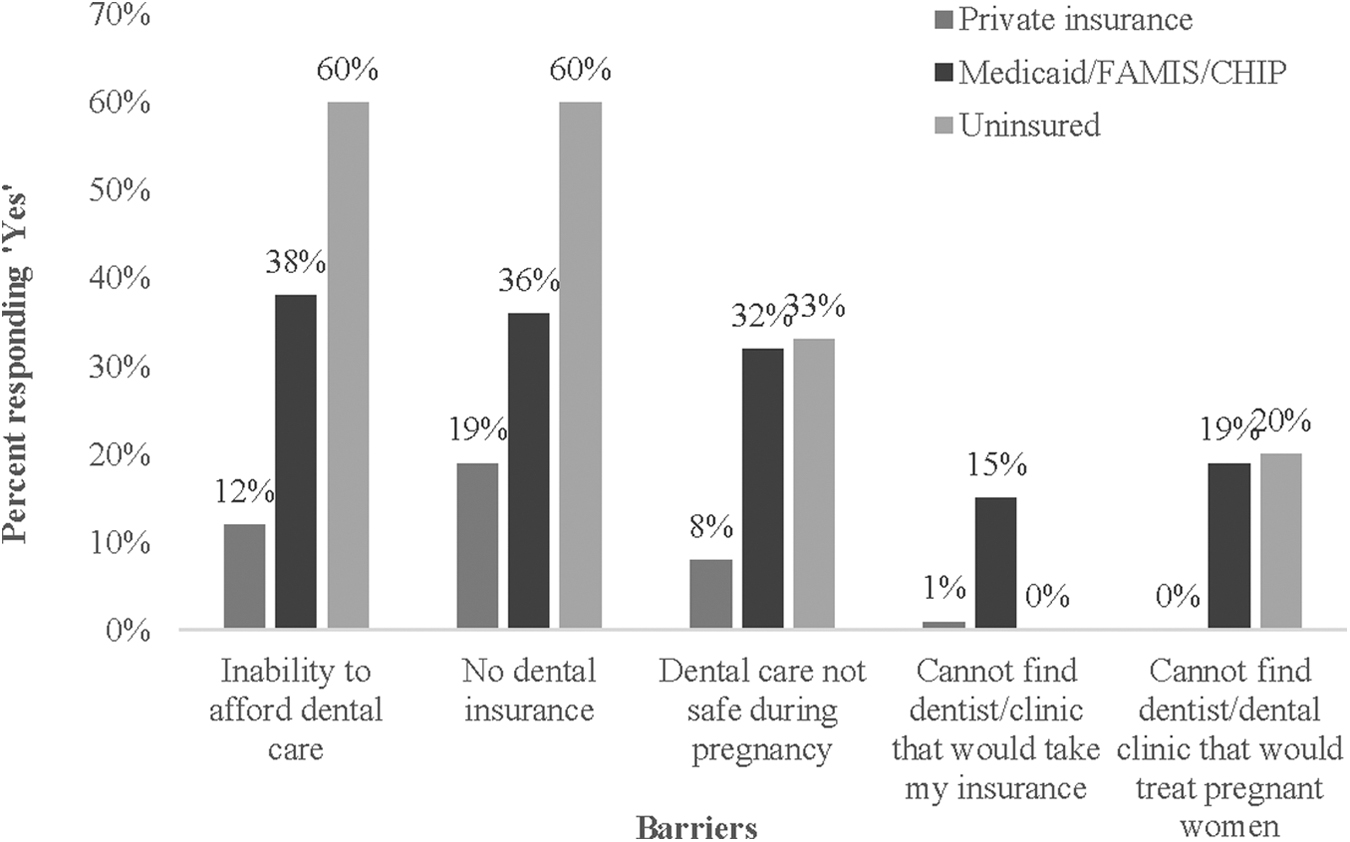
Barriers to dental care access during pregnancy by health insurance type. p < 0.0001 for all barriers.
The awareness of the dental coverage among Medicaid-enrolled women (n = 68, 5 women did not answer the awareness question) was 66% (Table 2). Race/ethnicity, education, source of health information, and last dental visit variables were condensed into two categories to allow for better estimation. The bivariate analysis found significant relationships between dental coverage awareness and oral health knowledge score (p = 0.008) and health information source (p = 0.026) (Table 2).
Awareness of Medicaid Dental Pregnancy Benefit Among Women Enrolled in Medicaid
p-Value from bivariate analysis.
p-Value from overall multivariable logistic regression model <0.05.
aOR, adjusted odds ratio from the logistic regression model; CI, confidence interval.
In the adjusted logistic regression model, the knowledge score was significantly associated with dental coverage awareness (adjusted odds ratio [aOR] = 2.77, 95% CI: 1.18–6.51; p = 0.0193). Women who reported a health care provider or other health care source as their primary health information source had five times higher odds (aOR = 5.06 95% CI: 1.00–25.49) for Medicaid dental coverage awareness compared with their counterparts (p = 0.0496). The dental coverage awareness did not differ significantly by pregnancy status (Table 2).
Discussion
We found gaps in pregnancy-related oral health knowledge among reproductive-aged women by insurance type. Medicaid-enrolled and uninsured women experience barriers to accessing oral health during pregnancy at a much higher rate compared with those with private insurance. The provision of comprehensive dental coverage for pregnant women in Virginia can address many of the frequently reported access barriers to dental care, but its awareness among Medicaid-enrolled women needs to be improved.
In this study, almost 40% of Medicaid-enrolled women did not know that pregnancy is a period of higher risk for oral health problems. One-fifth were unaware of the linkages between oral health and general health, and 25% had safety concerns about receiving dental care during pregnancy, suggesting the need to improve oral health knowledge. Our findings are consistent with other studies that have reported similar or lower oral health knowledge among minority and low-income pregnant women. 11,12 Medicaid-enrolled women reported a higher frequency of barriers to dental care access during pregnancy. Thus, these findings combined with limited pregnancy-related oral health knowledge can further limit access and use of dental care among Medicaid-enrolled women. 13
Despite the availability of dental coverage for pregnant women since 2015, not many eligible women have used this coverage. We found that one in three reproductive-aged women enrolled in Medicaid were unaware of the available pregnancy dental coverage in Virginia. Furthermore, to our surprise, awareness did not differ by pregnancy status. This may be a possible indication of inadequate promotion/outreach or knowledge about the available dental coverage among health providers and programs that serve these women. Focused interventions to reduce oral health misconceptions, address barriers, and improve dental coverage awareness through health care and community-engaged service providers are warranted to improve access and use of dental care among Medicaid-enrolled reproductive-aged women. Programs that can connect community resources, educate women, provide preventive care and dental referrals can improve oral health knowledge and increase dental utilization. 14
Dental coverage awareness was found to be positively associated with the oral health knowledge score and health information source. These results highlight the opportunity for the academic center health care providers and programs to educate reproductive-aged Medicaid-insured women about the health benefits available to them. Health care provider oral health promotion is also found to be significantly associated with increased use of dental services. 4 Women referred to a dentist by their gynecologist had five times higher odds of visiting a dentist than those who were not referred. 15 Frequent prenatal visits could be teachable moments where health providers can educate women about oral health and share dental benefit information verbally or through written materials along with a referral to a dental care provider. Health care clinics and programs that serve pregnant women (e.g., Special Supplemental Nutrition Program for Women, Infants, and Children; Early Head Start; Home Visiting) can integrate oral health topics in prenatal classes, help in care coordination, provide oral health education flyers with pregnancy-related oral health information, and information about available dental coverage through the Medicaid program. However, to create a culture of health care integration and leverage the missed opportunities during prenatal visits, it is essential to address health care providers' barriers to oral health promotion. 16
This study's findings are timely and valuable as Virginia plans to expand comprehensive dental coverage to all Medicaid-enrolled adults beginning July 2021. The information from this study can help program administrators, clinicians, and oral health stakeholders identify groups for focused outreach and effective ways to promote adult dental coverage.
Limitations
First, the study sample was recruited using a convenience sample technique, and the data were self-reported. Thus, it is subjected to selection and recall bias. To our knowledge, it is the first study to examine awareness of a Medicaid policy for dental coverage during pregnancy. Second, health insurance questions did not ask about dental insurance to compare with other state-level findings and help determine broader groups for targeted interventions. The precision of the regression model was low, as indicated by the wide confidence intervals (CIs). This may be because of the small sample size for Medicaid-enrolled women. However, this analysis allowed us to explore the factors associated with awareness of dental coverage. Finally, the data were collected in an academic health care setting that could limit the generalizability of our findings to other settings/states.
Nevertheless, our sample was a subset of the population to whom the pregnancy dental coverage was applicable. Despite the above limitations, the study provides a valuable assessment of oral health knowledge, barriers to dental care, and baseline estimates for dental coverage awareness among reproductive-aged Medicaid-enrolled women in Virginia. Future research from a larger and more diverse sample is warranted to deepen the understanding of how dental coverage awareness impacts dental care use patterns among women and what barriers women face in using the available benefit.
Conclusions
In our sample, significant gaps existed in oral health knowledge among reproductive-age women by health insurance status. Medicaid-enrolled and uninsured women were three to five times more likely to face barriers to access dental care during pregnancy than women with private insurance. Insurance coverage for dental services can aid in reducing barriers to dental care. However, a significant proportion of Medicaid-enrolled women were unaware of available dental coverage during pregnancy through Medicaid even after 3 years of the policy implementation. Improvement in oral health knowledge and awareness of dental coverage can address barriers to dental care access and use and reduce disparities in oral health and overall health outcomes of Medicaid-enrolled women. As the first examination of the awareness of Medicaid policy for dental coverage during pregnancy in an urban academic center setting, this study's findings can inform oral health and women health providers and Virginia policy stakeholders on factors associated with dental coverage awareness.
Footnotes
Acknowledgments
The authors thank all research assistants who helped in data collection and survey participants who took part in the study.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the VDH or HRSA.
Ethics Approval and Consent to Participate
The study was approved by Virginia Commonwealth University's Institutional Review Board.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded in part by the Virginia Department of Health (VDH) contract received by S.N. and T.H.B. under the VDH Perinatal and Infant Oral Health Quality Improvement grant by the Health Resources and Services Administration (HRSA).