
Abstract
Background:
Hip fractures can dramatically impact the health and self-sufficiency of older people. We investigated the influence of pre-fracture functional status on functional decline and mortality after hip fracture, and possible sex differences in this regard.
Materials and Methods:
The sample comprised 288 older patients hospitalized with hip fracture in an Orthogeriatric Unit. Data on perioperative management and multidimensional evaluation were collected. After 15 months, we obtained information on housing arrangements, new falls, walking level, and self-sufficiency (Barthel Index [BI]) through outpatient visits or phone interviews. Data on re-hospitalizations and deaths were obtained from hospital records.
Results:
The sample median age was 87 years, and 75% were women. The median pre-fracture BI was 75 (interquartile range [IQR]: 50, 100), and at follow-up it decreased by a median of 20 (IQR: 40, −5) points. Sex differences emerged among those with the highest pre-fracture functional status (BI ≥85), with women showing lower BI loss than men (−15 [IQR: −40, 0] vs. −30 [IQR: −80, −15], respectively; p = 0.04). A pre-fracture BI ≥85 (vs. <85) was associated with a 41% lower mortality rate (95% confidence interval [95% CI]: 0.21–0.79), especially in women (hazard ratios = 0.28, 95% CI: 0.11–0.69). Moreover, male sex was an independent risk factor for functional loss after a hip fracture (odds ratio = 2.52, 95% CI: 1.09–5.80).
Conclusions:
Older men may have a worse functional prognosis than women after a hip fracture. This difference seemed to be exacerbated in cases of high pre-fracture functional performance, suggesting that females have a greater functional reserve, namely better adaptation and recovery strategies to deal with the fracture. Clinical Trial Registration: Registration code: NCT02687698.
Introduction
Sequelae of hip fractures are very important as they substantially impact quality of life, morbidity, and mortality, especially in older people. 1 The natural history of hip fractures is dismal if patients are left untreated, but even with surgery the mortality rate is 10% after 1 month and reaches 36% after 1 year in patients having undergone both surgery and rehabilitation. 2,3 In addition to mortality, hip fractures substantially impact individuals' functional status.
Globally, 1.66 million hip fractures occur worldwide every year and 4.5 million people are disabled from this injury. Indeed, about 30% of hip fracture patients are estimated to become permanently disabled: 40% of them lose the ability to walk independently, and 80% cannot independently perform day-to-day activities after the fracture. 4
There may be some differences between men and women in the burden of hip fractures on older people. Hip fracture incidence is higher among women, especially in older age, 5,6 with the female: male ratio being around 3:1. This greater frequency of hip fractures among women is due to both the reduction in bone mineral density after menopause and a higher risk of falls related to sex-specific body composition features, such as lower muscle mass 7 Despite the higher incidence of hip fracture among women, male patients are generally frailer and have a higher 1-year mortality rate after hip fracture.
Previous studies have suggested that the survival advantage of women could be partly due to the worse clinical status of men at the time of the fracture, and their higher risk of postoperative complications. 8 –10 The evidence regarding functional recovery after hip fracture in men and women is still mixed. Interestingly, a study on the recovery of walking performance found a male advantage only among those cognitively intact, whereas there were no differences in the presence of cognitive deficits 11
Overall, these findings suggest that pre-fracture factors influence the prognosis of hip fractures, and it can be hypothesized that such effect may be modified by sex- and gender-related aspects. Among these pre-fracture factors, low functional status is considered a strong and independent predictor of poorer functional outcomes. 8,12,13
In light of these considerations, the study aims were: (1) to assess the impact of pre-fracture functional status on functional loss and mortality in older men and women; and (2) to determine whether sex independently influences health-related outcomes, such as functional status, mobility, and mortality.
Materials and Methods
Subjects
This prospective study was carried out in the Orthogeriatric Unit of the Hospital of Bolzano (Italy). We enrolled patients aged 75 years or older, who had been admitted for low-energy hip fractures from June 2016 to June 2017. Exclusion criteria included having experienced a hip fracture due to high-energy trauma (e.g., a road accident) or cancer.
Of the 299 individuals initially enrolled for the study, we excluded 6 individuals who died before undergoing surgery, and 5 who did not undergo hip fracture surgery, resulting in a final sample of 288 patients.
The study participants underwent an initial assessment during their hospital stay. A follow-up assessment was carried out after a mean interval of 15 months through face-to-face interviews (n = 57) or structured phone interviews (n = 117) by the same physicians. Of the original sample of patients, 79 had died, and 35 were lost at follow-up. A total of 174 patients were, therefore, evaluated for post-fracture functional status.
The study was given formal authorization by the local Ethics Committee and complied with the ethical standards of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All patients, or their next kin for those with cognitive impairment, gave written informed consent to take part in the study.
Measures
The following information was collected from each patient during hospitalization by physicians working at the Orthogeriatric Unit: sociodemographic data (age, sex, living arrangements), hip fracture characteristics (type and side of the hip fracture), the timing of surgery (≤ vs. >48 h after the event), type of anesthetic (epidural vs. general), and surgical method (categorized as hip prosthesis placement vs. nail/proximal femoral nail antirotation placement). In addition, we carried out a multidimensional assessment to collect data on: – pre-fracture mobility level, through the Fracture Mobility Score;
14
the patients' mobility levels were categorized as freely mobile without aids, mobile outdoors with one aid, mobile outdoors with two aids or frame, some indoor mobility but never going outside without help, and no functional mobility; – functional status, through the validated Barthel Index (BI), with a score ≥85 indicating high-functioning individuals;
15
– clinical complexity, considering the number of chronic diseases through the Cumulative Illness Rating Scale (CIRS)—Comorbidity Index (CI), and their severity trough the CIRS—Severity Index (SI)
16
; – polypharmacy
17
defined as the use of >5 drugs per day (diuretics, anti-hypertensives, benzodiazepines, opioids, antidepressants, antipsychotics); – physician-diagnosed cognitive impairment; – history of hip fractures; – in-hospital rehabilitation after the fracture.
After a mean period of 15 months, physicians contacted the study participants (or their next of kin for the cognitively impaired) and collected information on their current living arrangements (home vs. nursing home), mobility level (able vs. unable to walk), and post-fracture BI. Information on the vital status of the study participants over the intervening period was obtained from local hospital records. Using the data cited earlier, for the purposes of our study we defined functional loss as a reduction of more than 9.8 points in the BI score over the follow-up period, considering the value of the minimal clinically significant BI change as a cut-off 18 ; and mobility loss, as the transition from being able to be unable to walk. We also recorded all-cause mortality.
Statistical analysis
The normal distribution of continuous variables was checked with the Shapiro–Wilk test and graphical examination. The baseline characteristics of our study participants are expressed as means ± standard deviation (SD) for continuous normally distributed variables, as medians and interquartile range (IQR) for non-normally distributed variables, or as frequencies (percentages) for the categorical variables. Men and women were compared for these characteristics with the Student's t-test, Mann–Whitney test, or Chi-square test, as appropriate.
Since the distribution of pre- and post-fracture BI scores were non-normal, values were expressed as median (IQR) and compared in the sample as a whole and stratified by gender and by pre-fracture functional status using the Wilcoxon test.
The association between sex and the odds of functional or mobility loss was performed through multinomial logistic regressions. These outcomes were tested in two separate multinomial models, which included functional or mobility loss as primary outcome, and death as an alternative outcome. The strengths of these associations were expressed as odds ratios (OR) and 95% confidence intervals (95% CI).
The impact of pre-fracture functional status on mortality in the sample as a whole and stratified by sex was assessed using Cox regressions and expressed as hazard ratios (HR) and 95% CI.
The logistic and Cox regression models were first adjusted for age and sex (Model 1), and then also for additional potential confounders (pre-fracture living arrangements and mobility limitation, cognitive impairment, CIRS-CI, number of drugs used, repeated hip fracture, time of surgery, and post-fracture rehabilitation; Model 2). Covariates were selected based on the characteristics that seemed to differ between men and women at baseline and/or could play a possible confounding role in the tested associations.
All analyses were performed in SPSS 21.0 for Windows (IBM Corp, Armonk, NY, USA). Statistical tests were two-tailed, and statistical significance was assumed at a p < 0.05.
Results
Table 1 shows the baseline characteristics of the total sample (73 men, 215 women). The participants' median age was 87 (IQR: 82–91) years, with the men being significantly younger than the women. Before the hip fracture, most of the participants lived at home (83.7%) and were able to walk (64.9%), either independently or with assistance/walking aids (52.1%), with no differences by sex. The median pre-fracture BI was 75 (IQR: 50–100), again with no sex differences. Participants had a median of three chronic diseases, with the men having a slightly higher number and severity of chronic illnesses than women according to the CIRS-CI and CIRS-SI scales, respectively.
Baseline Characteristics of the 288 Study Participants Stratified by Sex
Numbers are counts (%) for categorical variables, and medians (interquartile range) for continuous variables.
CIRS-CI, Cumulative Illness Rating Scale–Comorbidity Index; SI, severity index.
Around one-third of the sample presented with dementia (36.5%), whereas more than half (55.9%) were taking >5 drugs/day, with diuretics, antidepressants, benzodiazepines, and antipsychotics being the most widely used medicines. Regarding surgery timing and type, we observed that women were more likely to undergo surgery earlier than men and to be treated with screws or intramedullary nails, whereas men were more frequently treated with total or hemiarthroplasty.
A total of 174 participants underwent the 15-month follow-up. Compared with these individuals, those lost were more likely to be younger (median age 83 [IQR: 80–87] vs. 88 [82–91], p = 0.001), to live at home (97.1% vs. 81.5%, p = 0.02), and to have fewer chronic diseases (median CIRS-CI score 2 [IQR: 1–3] vs. 3 [IQR: 2–4], p < 0.001), and a higher pre-fracture functional status (median BI 100 [IQR: 70–100] vs. 72.5 [IQR: 70–100], p < 0.001).
No differences between groups in terms of sex distribution, pre-fracture mobility, and prevalence of polypharmacy and cognitive impairment were observed. Further details on the characteristics of male and female participants lost or died during the follow-up are shown in Supplementary Table S1.
Table 2 shows the BI changes experienced in the 15 months after the hip fracture by the study participants, stratified by sex and pre-fracture functional status. Over the follow-up, we observed a significant median BI loss of −20 points (IQR: −40, −5) in the total sample, with no differences between men (−25, IQR: −50, −10) and women (−20, IQR: −35, −5). Sex differences emerged only in the high-functioning group, with men exhibiting twice as great a loss in BI as women (median BI loss −30 [IQR: −80, −15] vs. −15 [IQR: −40, 0], respectively; p = 0.04).
Median Functional Changes over the 15-Month Follow-Up Period by Sex and Pre-Fracture Functional Status
Bold values indicates statistical significance of p value is less than 0.05.
Describe sex difference considering high functioning group.
Numbers are medians (interquartile range). Within-group p-values are derived from the Wilcoxon test; between-group p-values are derived from the Mann–Whitney test.
BI, Barthel Index.
Considering the minimal clinically significant change of BI, during the follow-up, 73% of participants lost ≥9.8 BI points compared with their pre-fracture BI, with no differences by sex. As concerns mobility, comparing pre- and post-fracture assessments, 39.9% of the sample remained able to walk (independently or with walking aids), 26% remained unable to walk, and 34.1% worsened in their mobility level, similarly in men and women (data not shown).
Logistic regression analysis confirmed these results (Supplementary Table S2), with men demonstrating a chance of functional decline almost three-fold higher than that of women (OR = 2.94, 95% CI: 1.04–8.30), whereas no significant findings emerged for mobility loss.
During the follow-up, 31 men (42.5%) and 48 women (22.2%) died (p = 0.001). When considering the association between pre-fracture functional status and mortality at Cox regression (Fig. 1, Supplementary Table S3), in the total sample we found that having a pre-fracture BI ≥85 was associated with a 59% lower mortality (95% CI: 0.21–0.79, p = 0.01) compared with those who had a lower functional status. The interaction between pre-fracture BI and sex was marginally significant (p = 0.07) and, after stratification, women demonstrated a stronger inverse association between pre-fracture functional status and mortality (HR = 0.27, 95% CI: 0.11–0.67) than men.
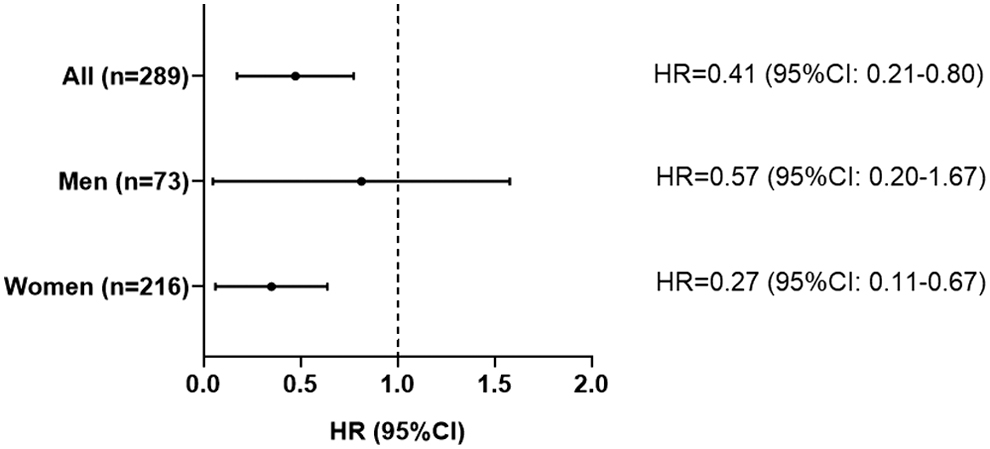
Cox regression for the association between pre-fracture Barthel Index (≥85 vs. <85) and mortality over 15-month after hip fracture in the total sample and by sex. Cox regression considers 15-month mortality (outcome) as a function of having a pre-fracture Barthel Index ≥85 (exposure; reference category: Barthel Index <85). Model is adjusted for age, sex (only in the non-stratified analysis), pre-fracture living arrangements, pre-fracture mobility limitation, cognitive impairment, Cumulative Illness Rating Scale—Comorbidity Index, number of drugs used (<5 vs. ≥5), repeated hip fracture, time of surgery (< vs. ≥48 hours), and post-fracture rehabilitation. 95%CI, 95% confidence interval; HR, hazard ratio.
Discussion
Our study confirms that hip fracture is associated with a significant worsening in functional status in older people and supports the presence of differences between men and women in this regard. Indeed, the latter seem to have a lower risk of functional loss and to be more able to buffer the impact of hip fracture on their self-sufficiency, supporting the hypothesis that they may have greater functional reserve.
Our participants were older than those studied in previous similar works, and the sample included a large number of oldest-old individuals. In line with previous reports, men were younger than women at hospital admission, 10,11,19 –21 and they presented a slightly higher number and severity of chronic diseases. 10,20,22 The latter characteristics are likely to have influenced the lower frequency of individuals undergoing surgery within 48 hours after ward admission observed in men compared with women.
As shown by several studies, the time between hospital admission and hip fracture surgery, along with other factors such as the American Society of Anesthesiologists (ASA) physical status and the number of comorbidities have been associated with higher rates of mortality and perioperative complications. 21,23
At the 15-month follow-up, around a quarter of our study participants had died. Of note, among the survivors, almost two-thirds experienced a clinically significant loss in BI compared with their pre-fracture status. This picture is consistent with the results of previous works, which report similar functional losses 12 and 1-year mortality (ranging between 14% and 36%), 23 and confirms the extreme burden of hip fracture for older people's self-sufficiency and health. Regarding the impact of sex on these outcomes, in line with current literature, we found higher mortality among men, despite them being younger than the women at the time of fracture. 10,19 –22
Differences between men and women in functional outcome after hip fracture have been previously studied, with inconsistent results. Some studies found no significant sex differences in functional recovery after the event, 10,22,24 whereas others reported better functional outcomes either for males 25,26 or for females. 19,21 Moreover, although there were no significant differences between men and women in pre-fracture functional status, male sex was also an independent predictor of loss of self-sufficiency. The sex differences seemed to be more marked among those who were functionally independent before the hip fracture.
We found that in this subsample the median loss in BI was twice as high in men as in women over the same study period. Although our analyses were adjusted for pre-fracture functional status and other factors, such as clinical complexity, which are associated with poor health-related outcomes, we cannot rule out the possibility of residual confounding linked to greater vulnerability of men.
Overall, these results suggest that women are more likely to recover and preserve their pre-fracture functional status, especially those in the high-functioning group. In this regard, it could be argued that, like the concept of cognitive reserve, the ability of individuals to reduce the burden of adverse events (e.g., hip fractures) to maintain their self-sufficiency may be considered a sort of functional reserve. (1) This kind of reserve could be influenced by several sex- and gender-related factors. Among these, it is possible that women have better coping strategies than men, and they are therefore better able to deal with adverse events, such as hip fracture or related functional impairment.
Indeed, previous studies have suggested that men may be more fragile and their coping strategies less suited to a situation of functional dependency compared with women. 11,21,27 In addition to the differences observed in the functional burden of hip fractures, we found that pre-fracture functional status was more strongly associated with mortality in women than in men. This finding corroborates previous studies on the relationship between some markers of frailty and clinical complexity, such as the number of comorbidities, with a 12-month mortality after hip fracture 28
The current study has not only its strengths, but also some limitations that need to be acknowledged. The main limitation concerns the small sample size, especially of male participants, which may have reduced the statistical power of our analyses, particularly when stratifying by sex and by pre-fracture functioning. In addition, functional status was assessed only by BI and level of mobility, whereas no objective measures of post-fracture physical performance (e.g., walking speed) were taken.
However, given the study's real-world setting, data on post-fracture physical performance could have been of limited use due to the unavailability of the corresponding pre-fracture information. Moreover, BI has been shown to be a reliable tool for evaluating patients' levels of self-sufficiency and is widely used in clinical practice 27 This work's strengths, on the other hand, lie in the prospective study design and the number of collected variables.
Further, with its focus on the sex differences, the study makes an interesting contribution to current literature on the topic, although more extensive investigations on specific gender domains that could influence individuals' functional reserve are still needed. Nonetheless, this work highlights the importance of taking this factor into account and of adopting a personalized approach in dealing with patients with hip fractures in daily clinical practice.
Conclusion
Our findings reveal male sex to be an independent predictor of poor functional prognosis after a hip fracture, whereas women with a higher pre-fracture functional status have a lower risk of mortality and are more likely to recover and preserve their self-sufficiency post-fracture, possibly due to greater functional reserve. Identification of the factors that aid recovery after hip fracture and influence individual functional reserve may help clinicians plan targeted, personalized interventions to reduce the burden of hip fracture on the self-sufficiency, quality of life, and overall health status of older men and women.
Footnotes
Acknowledgments
The authors thank all the patients and physicians who contributed to the study. They thank Tessa Say for English language editing of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding information was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.