
Abstract
Intimate partner violence (IPV) affects many, and health care has the potential to provide a safe space for individuals experiencing IPV. However, physicians cite lack of time and education as barriers. The aim of this study is to complete a review of published IPV curricula in medical school, residency training, and postresidency training. We performed a scoping review to provide a quantitative assessment and summary review of existing IPV curricula. In May 2020, a librarian conducted a search of Ovid MEDLINE, Ovid EMBASE, and Scopus. We evaluated each article for the following curriculum content and structure items: (1) year introduced; (2) delivery method; (3) curriculum type; (4) curriculum content; (5) curriculum effectiveness; and (6) implementation barriers. Fifty-six articles met criteria, most were for medical school learners (n = 32, 57.1%) and short-term (lasting less than one academic year) (n = 41, 73.2%). For residency, IPV curricula were most frequently taught in family medicine, internal medicine, and emergency medicine. Formal lecture and use of standardized patients were the most popular delivery methods. Most curricula taught risk factors for and identification of individuals who have experienced IPV. The most cited implementation barrier was limited time in standard medical education, followed by inability to measure the effectiveness of the curriculum. There was great variation in the methods of assessing effectiveness of IPV curricula. Published IPV curricula are varied, without consistent validated tools for assessing efficacy. Future initiatives to establish a standard of competency for medical students regarding IPV, including a standard curriculum, may better ensure that physicians are capable of identifying and caring for individuals who have experienced IPV.
Introduction
In the United States, over a third of women have experienced intimate partner violence (IPV) in their lifetime and over 10 million men and women are affected yearly. 1 IPV includes sexual abuse, physical abuse, psychological aggression, control of reproductive or sexual health, and stalking. 2 Individuals who have experienced IPV are at an increased risk for a myriad of adverse health outcomes, including higher rates of gynecologic, musculoskeletal, pulmonary, dermatological, gastrointestinal, cardiovascular, and neurological conditions. 3,4 More than half of individuals who have been affected by IPV also experience psychiatric disorders, including anxiety, psychosis, and substance abuse. 5,6 Many report long-term health complications, with an average of two of every three individuals who have experienced IPV attributing their health problems to IPV. 4
Despite the rate of IPV rising 46% between 2014 and 2015, 7 the Liaison Committee on Medical Education (LCME), a United States institution, removed violence and abuse as a mandatory curricular component for U.S. medical schools. 8 –10 They provided no explanation for this change and made the requirement broader to state that medical school curriculums should include “instruction in the diagnosis, prevention, appropriate reporting, and treatment of the medical consequences of common societal problems”. 11 Given that physicians who are trained in IPV are more likely to ask questions routinely, identify, and care for individuals who have experienced IPV, 12 efforts to increase IPV curricula in medical school training are imperative.
Violence is a public health crisis and is a preventable cause of disease. Health care professionals can play a key role by providing both preventative care to individuals who have experienced IPV and treating their symptoms derived from the perpetrated violence. 13 Physicians are often the first professionals to encounter individuals who have experienced IPV and are in a unique position to ask about IPV and refer the patient to ongoing support. Survivors often believe that their doctors are some of the few people to whom they can disclose their experiences. 14 Therefore, physicians play a vital role in identifying individuals who have experienced IPV and halting the cycle of abuse by assessing and asking patients directly, validating patients' feelings, documenting, and referring patients to helpful resources.
However, primary care and other frontline physicians generally lack significant clinical training in behavioral health and IPV, 15 which contributes to low efficacy for identification and management skills, the fear of offending patients, and the perceived lack of time in the clinical setting. 16 Many cite not intervening due to the lack of knowledge of legal issues, cultural barriers to communication, and the perceived unresponsiveness of patients. 16 Furthermore, physicians' awareness of the prevalence of IPV is poor, 17 and patients are rarely asked about IPV.
There is only a 1.5% to 12% screening rate for IPV in the primary care setting, despite the fact that the U.S. Preventive Service Task Force recommends screening all women of childbearing age for IPV regardless of the presence of visible signs or symptoms of abuse. 17 –19 Furthermore, major medical associations, including the American Academy of Family Physicians, the American Medical Association, and the American College of Obstetricians and Gynecologists, recommend routine IPV screening. 20
Interventions that begin early in medical training, such as in medical school, are more likely to have long-lasting effects on an individual's practice. 21 Interventions in residency training also demonstrate significant improvements in trainee practices. 22 A study of 33 internal medicine residents found that residents who are educated in IPV are more knowledgeable of its connection to medicine, more inclined to screen for IPV, and have more confidence in their abilities to help such patients. 22,23
When surveyed, 125 third and fourth year medical students and primary care residents (pediatrics, family medicine, internal medicine, and obstetrics/gynecology) report that they feel their IPV training is inadequate and leaves many gaps in knowledge. 24 Furthermore, there is not consensus among medical students and residents of different specialties on the optimal curriculum content and clinical skills for teaching IPV to medical trainees. 25 –27 Understanding what currently exists in this curricular area can guide future efforts to improve training for future physicians.
The objective of this study was to complete a scoping review of published curricula on IPV in medical school, residency training, and postresidency training and provide a summary of the findings to guide the standardization of an optimal curriculum for medical students (MD/DO schools). Because of LCME's removal of the IPV specific standard, this review focuses on medical student education. Residency and post-training educational articles were included to understand the current distribution of IPV curricula and analyze what methods are most effective for implementation.
A scoping review approach was taken to provide a quantitative assessment and summary review of existing IPV curricula. The goal of this study was to characterize IPV curriculum content and structure items, including the year curriculum was introduced, method of delivery, curriculum type, curriculum content, curriculum effectiveness, and implementation barriers.
Materials and Methods
We conducted a scoping review following the methodological framework outlined by Arksey et al. 28 along with the PRISMA extension for scoping reviews (PRISMA-ScR) checklist. 29
In May 2020, a medical librarian conducted a literature search of Ovid MEDLINE, Ovid EMBASE, and Scopus using a combination of MeSH (Medical Subject Headings) terms and keywords, including domestic violence OR physical abuse OR battered women OR spouse abuse OR intimate partner violence AND medical education OR undergraduate medical education OR education, medical, undergraduate OR internship and residency OR medical resident AND curriculum OR teaching.
The literature search produced a total of 703 references from 1946 through 2020 and was not limited by country. After removing duplicate references, we reviewed 409 for either inclusion or exclusion. Studies that met inclusion criteria contained primary sources and educational materials on IPV for medical students, residents, or physicians. Studies were excluded for: non-English language, nonempirical research on IPV, materials for nonhealth students or clinicians, opinion or commentary pieces, and survey studies looking at aggregate data.
Three researchers independently reviewed each title and abstract to determine whether it met the proper inclusion criteria and exclusion criteria. The lists of articles identified by each researcher were compared for discrepancies. In the setting of a disagreement on any article, the three researchers discussed the article until there was a consensus among the three. Three researchers independently reviewed each of the full-text articles that met inclusion criteria (N = 56). The evaluated content areas were chosen based on an aggregate review of IPV curriculum types by Hamberger. 22 It outlined the different models found in IPV implementation and integration, barriers to implementation, curricular content, and evaluation types.
Content variables
Each article that met inclusion criteria was evaluated for the following curriculum content and structure items in the article's full text (N = 56); (1) the year the curriculum was introduced; (2) the method of curriculum delivery; (3) the type of curriculum; (4) the curriculum content; (5) the effectiveness of the curriculum; and (6) the barriers experienced in implementing the curriculum (Table 1). Each article was first evaluated for those of the aforementioned variables it included. Then, it was further qualitatively analyzed to address the details of the criteria. Table 1 defines the criteria and definition of each variable included.
Description of Curricular Descriptive Variables
Results
This scoping review generated 409 articles. Of these articles, 48 were excluded for being nonprimary source articles and another 189 articles were excluded for not mentioning IPV or domestic violence in their titles and/or abstracts. If IPV or domestic violence was not referenced in the title, the abstract was still assessed for any mention before exclusion. Of the remaining 172 articles, 55 were excluded for not being related to medical education/training. The remaining 103 articles were read in depth, and of these, 48 were excluded for being survey studies with aggregate data of more than one curriculum, leaving 55 scholarly articles. One article was added after reviewing key references, for a total of 56 articles included for review and assessment (Fig. 1).
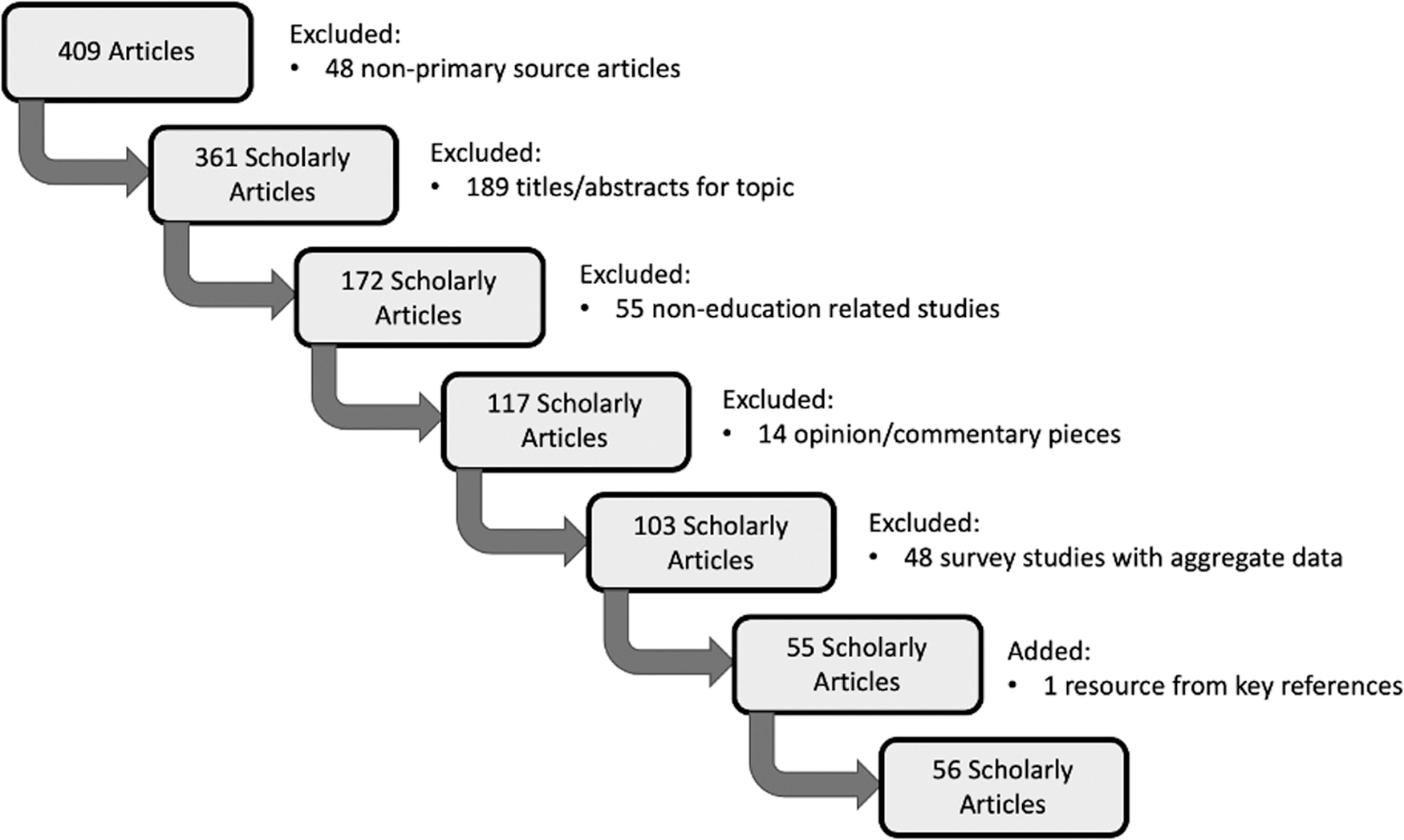
Results of the scoping review.
Only five of the articles were published after 2015. Tables 2 and 3 include a quantitative summary of the literature review by content variable and article type.
Quantitative Summary Results of the Literature Review
Quantitative Summary Results of the Literature Review
Stage of training
A majority of curricula took place during medical school (n = 32, 57.1%), and others discussed IPV curricula in residency training and a few for physicians postresidency. For residency training, the IPV curricula were most frequently taught in family medicine, pediatrics, internal medicine, emergency medicine, psychiatry, and obstetrics and gynecology programs.
Mode of curriculum delivery
Formal lecture (n = 32, 57.1%) and use of standardized patients (n = 28, 50.1%) were the most popular methods of curricular delivery. The less common methods included having group reflections (n = 23, 41.1%), written materials (n = 21, 37.5%), online modules or videos (n = 15, 26.8%), opt-in experiences (n = 12, 21.4%), and real clinical patient encounters (n = 11, 19.6%).
An exemplary model was presented by Joyce et al., who incorporated both didactics and standardized patients, as well as real clinical patients, while using both subjective and objective measurements of effectiveness. They demonstrated that second year medical students' knowledge and self-confidence improved through their curriculum. 49 Third year medical students' ability to screen and identify individuals who have experienced IPV through standardized patients also improved, as demonstrated by pre- and postcurricular surveys that tested subjective measures of self-confidence and knowledge in regard to IPV in the clinical setting.
Curriculum form
Those that met the criteria for short-term (73.2%) and problem-based (62.5%) curricula were the most common. Nine were identified as long term (16.1%), 13 as immersion programs (23.2%), and 12 as integrated (21.4%).
The curriculum at the University of Pittsburgh School of Medicine incorporated didactic training into three points in the existing medical school curriculum. 33 IPV was taught during ethics lectures in the first year, in small group sessions during the OBGYN clerkships in third year, and during small group sessions during the multidisciplinary outpatient clerkship in third year. In addition, students were given the opportunity to participate in an advocacy program to provide support to individuals who have experienced IPV in the emergency department and to volunteer in a clinic housed within a shelter. 33
Curriculum content
The teaching of the risk factors for IPV (n = 33, 58.9%) and the identification of individuals through history taking (n = 35, 62.5%) constituted the most prevalent content within the curricula assessed. Many also included physical examination components in their curriculum (n = 26, 46.4%). Other common content topics included associated health consequences (n = 24, 42.9%), barriers to seeking/providing health (n = 23, 41.1%), legal protections (n = 23, 41.1%), community resources (n = 30, 53.6%), and guest speakers (IPV survivors, social workers, legal teams) (n = 24, 42.9%).
Schrier et al. covered these topics in their curriculum. 72 Part of the curriculum involved an Objective Structured Clinical Exam (OSCE) activity in which students conducted a history on a patient who presented with abdominal pain and had concerns with a relationship at home. The OSCE activity not only required that students identify the clinical presentation of IPV but also assessed knowledge of social and legal resources to best help the patient develop a plan moving forward.
Shefet et al. utilized the OSCE to emphasize points of discussion regarding legal educational points such as duty to inform individuals who have experienced IPV of aid resources, to document IPV in a patient's medical chart, and to respect patient autonomy in such cases. 73 The study found that students performed well on the OSCE with a first-time pass rate of 97.5%.
The curriculum studied by Ferrell et al. serves as an example of the case-based problem-solving model and has shown that participation leads to increased routine inquiry of IPV by residents. 39 Despite the increase in screening that occurred after completing the curriculum, residents still reported discomfort in asking patients about IPV.
Barriers associated with curricular implementation
Time to implement the curriculum was the most cited barrier to implementation (n = 22, 39.3%), followed by lack of engagement, advocacy, and interest (n = 16, 28.6%), inability to measure the effectiveness of the curriculum (n = 14, 25.0%), cost/resources (n = 11, 19.6%), scalability (n = 8, 14.3%), and lack of faculty support or perceived relevance (n = 5, 8.9%). One article cited the LCME requirement to include topics such as abuse as a driving force behind implementing an IPV curriculum back in 2007. 43 No studies in this literature search directly quoted the 2015 LCME removal of IPV as a mandatory curricular component as a barrier to implementing such a curriculum.
Determining the effectiveness of the curriculum
Many of the articles did not specify how the effectiveness of the curriculum was determined (n = 20, 35.7%). Of those that did discuss effectiveness, there was great variation in the methods of assessing effectiveness of the curricula. Survey questions widely ranged from questions regarding objective knowledge to questions assessing comfort in speaking with IPV patients, with some studies not disclosing their survey questions. The surveys were typically produced specific to each school's curricular content.
Some cited subjective improvement in trainee confidence and comfort in caring for IPV patients. 31,34,38,39,42,45,48,49,51,53,54,57,58,61,64 –66,69 –71,73 –75 A notable survey utilized was the Physician Readiness to Manage Intimate Partner Violence (PREMIS) survey. This survey is validated and offers reliable and comprehensive measures of the subjective effectiveness of an IPV curriculum. 48
Some administered pre- and postcurricular surveys assessing objective knowledge about IPV and its connection to medicine. 23,32,33,35,36,43,44,49,52,57,58,62,64,66,71,73,75,79 Others used student performance on rotations or on OSCE and standardized patient simulations before and after curricular implementation. 41,48,49,53,59,62,72 Many cited subjective improvements in self-reported confidence in ability to identify individuals who have experienced IPV, objective improvements in knowledge of IPV's associated health consequences, increased awareness of legal and available societal resources, and higher scores in OSCE and standardized patient simulations (Table 3).
Discussion
Equipping physicians with knowledge on the prevalence, assessment techniques, and interventions for IPV are critical to halting the cycle of violence. As demonstrated, published IPV curricula exist. However, curricula vary greatly without consistent validated tools to assess effectiveness at achieving necessary learning objectives. This is further complicated by the fact that there are no standards for the level of knowledge medical students should have regarding IPV.
Literature exists on the best methods to deliver educational content and the most effective time period during a student's training. For example, standardized and real patient encounters contribute substantially to the medical education process. 81 Students who participate in standardized patient encounters perform significantly better on patient interviews than those who only participated in conventional didactics. 81 Improved performance was documented in five key areas: the use of open-ended questions, encouragement of patient participation, clarification of missing information in a patient's history, encouragement of patient emotions, and time management of the interview. 82
Formal didactics and standardized patient encounters were the most frequently used method of teaching IPV to medical students, residents, and attending physicians. Didactics and case-based learning provide an opportunity to dispel beliefs commonly cited by physicians, including concerns that individuals who have experienced IPV would not want to disclose to an opposite gender physician, the belief that their role does not include addressing IPV, and that IPV is not relevant to health care. 83,84 IPV curricula can challenge these beliefs, as well as outline the legal reporting obligations and the community resources available for individuals who have experienced IPV through a case-based format, as demonstrated by Shefet et al. 73 Imbedding legal topics and IPV resources into case-based learning formats is a promising strategy.
Another well received method for instruction uses didactic lectures accompanied by case-based problem-solving activities. 85 This method allows students to form a deeper level of comprehension, fosters interactions among classmates, improves student performance, and increases motivation for self-directed learning outside the classroom. 85 A case-based approach may be ideal for increasing routine inquiry, but may require additional teaching methods to improve physician comfort in addressing IPV.
Group reflections were also frequently used and may be another effective tool in this space. The value of reflection in medical education has long been supported by literature. 86 Reflective competence demonstrates an individual's ability to integrate actions with an understanding of the action, so they can continuously learn from those actions and modify them based on a specific scenario, which can strengthen the doctor–patient relationship and help provide better patient care. 86 Continually and systematically reflecting on one's own practice allows students to better translate their reflections into action. 86 Many curricula covered in this literature search utilized group reflections to solidify the lessons learned throughout the IPV-training experiences. 23,26,32,38,40,46 –49,51,55,58,60,66 –68,70 –73,75,77,79
A long-term integrated approach is the preferred format for teaching IPV. When topics are integrated longitudinally into various courses, students find these lessons more relevant to their future careers. 22 Most of the curricula reviewed were designed as short-term (less than one academic year) experiences with only a few that were designed to have IPV integrated throughout the current medical school curriculum. Buranosky et al. is a model curriculum as they utilized a problem-based curriculum that was both long term and integrated into the curriculum rather than being an independent course. 33
Student scores regarding IPV awareness, comfort screening for IPV, support of universal IPV screening, and importance of interventions for individuals experiencing IPV significantly increased over the years and were also higher with the addition of experiential activities compared to those without. For example, the mean score for a question regarding support for universal IPV screening on a Likert scale (quantified as 1–5) was 4.0 for students with no experiential exposure to IPV patients, but 5.0 for those who did have experiential exposure (p < 0.001). Their problem-based approach showed the students how the multidisciplinary team cares for an IPV patient. 87
In contrast, some of the short-term curricula covered in this literature search did not show as promising results. A study by Berger et al. demonstrated that there was no change in comfort in discussing IPV or whether students felt they had adequate time to screen for IPV in trainees before and after the implementation of the curriculum. 31
Consistency was not found for the methods of measuring the effectiveness of the IPV curricula reviewed. Outcomes were evaluated in various ways, including trainee feedback, pre and/or post-training surveys, subjective comfort of the trainees, and more objective measures of knowledge and OSCE examinations. Few studies evaluated the long-term impact of training on trainee behaviors such as assessment rates.
One example of a program that did this was by Haase et al., which utilized a short-term optional formal lecture for first-year medical students that covered topics such as identification of individuals experiencing IPV, history for screening individuals, and community resources available for individuals who have experienced IPV. 43 They found that 2 years following the initial teaching of the IPV curriculum, students performed well on a survey that assessed self-reported feelings of preparedness, frequency of IPV screening with patients, whether a student has identified an individual experiencing IPV, and whether the student recognized the acronym for IPV advocacy that was taught in the curriculum, highlighting that the knowledge gained from the curriculum was retained by students in the long run.
Based on the successful curricula explored in this literature search, a proposed method to evaluate the effectiveness of a curriculum comes in three parts: pre and post training surveys in student confidence and attitudes, i.e., ‘progress testing’, pre and post training surveys in student objective knowledge of the curriculum, and a practical exercise in which student performance is evaluated. 88 A validated survey that addresses these topics of interest is the PREMIS questionnaire that encompasses perceived IPV knowledge and preparation, objective IPV knowledge (measured by multiple choice and true/false questions), IPV attitudes and beliefs, and practice issues such as self-reported behaviors (including likelihood of actually screening patients). 89
Objective measurements such as performance on OSCE examinations, surveys on knowledge related to IPV, and chart review of trainee encounters with patients for routine inquiry and identification of IPV should also be implemented to complement the subjective assessment done by the PREMIS survey. Since IPV screenings are often performed by other members of the medical team such as nurses, interventions supported by social workers, including an interprofessional approach to training, should also be considered.
Despite many of the identified studies using effective medical education methods, there was variation and inconsistency in the implementation of these methods in IPV curricula. For example, the didactic lectures utilized by some institutions solely focused on the clinical presentation of IPV or assessment of IPV, leaving out other critical topics related to treating and caring for individuals who have experienced IPV. 36,46
Furthermore, there were studies in our literature search that did not utilize didactic and standardized patients as teaching methods. 45,63,68,75 Two of these studies did evaluate the effectiveness of their respective curricula and had interesting findings. 45,75 One study utilized a curriculum aimed at attending physicians and utilized an online problem-based curriculum which showed a 17.8% improvement in self-confidence of physicians in their ability to manage IPV patients. 45 Another study included an online case-based CME program for primary care physicians that showed significant improvement in self-efficacy and self-reported IPV management. 75 While the results of these programs were encouraging, it is notable that they target attending physicians who likely have already received some IPV training in the past.
Evidence-based and research-informed approaches from organizations such as Futures Without Violence, with training materials that have been developed by and for health professionals, may help to standardize curriculum content for medical students. 90 Project Connect is one example of a violence prevention and response initiative where over 7000 health care providers received training and technical assistance, with improvements in clinic policies and protocols, and connection to resources and safety for patients. 90 –92
An ideal IPV-specific curriculum for medical trainees includes a multifaceted approach that combines didactic lectures, standardized patient encounters, case-based approaches, and group reflections. A long-term, integrated, and problem-based approach to IPV is ideal. Continuous education on specific IPV topics throughout medical school and residency is most likely to equip medical practitioners with the toolkit to best approach specific issues in medicine such as IPV.
Integrating a standardized and freely available IPV curriculum can help address some of the common barriers cited, by providing ready-made resources that do not take away from an existing curriculum, but instead add to current teaching. Substantial curricular change requires support from the highest levels of academic institutions, as well as faculty development and awareness campaigns. The lack of current LCME requirements to specifically teach IPV to medical students may serve as a barrier, and a mandated policy may help assure curricular implementation. This is especially noteworthy considering that only five articles regarding specific IPV curricula have been published since the 2015 removal of the LCME IPV requirement. 33,52,55,63,69
LCME requirements can influence what is incorporated into the medical school curriculum as evidenced by the inclusion of the 2000 LCME requirement that medical students demonstrate a level of cultural competence. 93 This mandate aimed to address the biases that may lead to health care disparities in minority populations. Following the mandate, curricula addressing cultural competence increased in U.S. medical schools. 94
Another important skill that needs to accompany training on IPV for medical professions is a trauma-sensitive approach to care. A trauma-sensitive approach assures a safe environment that minimizes the chances of re-traumatizing patients. 95 It also creates a space where people are empowered and comfortable to share their experiences and address their trauma on their terms as part of their medical care. 96 Outcomes of a trauma sensitive approach include safety, trustworthiness and transparency, peer support, collaboration and mutuality, empowerment, voice and choice, cultural, historical, and gender issues. 95,96
Violence and abuse are forms of active oppression for individuals and it is important to teach future physicians to advocate for their patients' human rights. This is especially important in light of the current COVID-19 pandemic, in which IPV has been referred to as the “pandemic within the pandemic.” 97,98 Quarantine mandates isolated individuals further than they may have been prepandemic. Some individuals did not have access to telehealth because of lack of internet, leading to increased risk of abuse and isolation. Teaching students the principles of health equity and how it impacts patient care is important to ensure access to care and interventions equitably accessible by all groups, despite their place of residence, their race, ethnicity, culture, or language, their occupation, their gender, religion, education, socioeconomic status, and social capital. 99
Limitations
This study is subject to limitations inherent to a scoping review design, including that it may have missed relevant studies and that the quality of the articles was not assessed. Second, non-English articles were excluded, meaning we may have missed information from these articles. Third, the literature search was limited to articles about IPV curricula that are currently published and have been referenced in studies. This strategy excluded unpublished curricula, as well as curricula and teaching initiatives that are performed by student interest groups and professional organizations.
Limited information was available regarding curricular assessments in the reviewed articles and those that did demonstrated wide variability in assessments limiting the evaluation of the effectiveness of the included studies. Many studies utilized subjective feedback and differing forms of assessments to test trainee knowledge and comfort following the implementation of the curriculum, making outcome comparison difficult. Finally, there are some databases and search terms that were not included in this literature search and, therefore, may have excluded additional resources and references.
Conclusions
IPV is a problem that can affect all individuals regardless of sex, gender, age, socioeconomic status, cultural group, and other background factors. IPV curricula exist in medical training, but they are highly variable and not consistently evaluated for efficacy. Furthermore, our scoping review shows that published IPV curricula may have an opportunity for improvement to align with best practices in medical education. A longitudinal, case-based, and integrated curriculum implemented early in medical school may be the best model for training on IPV. Standardizing a national curriculum and raising the importance of this curriculum to the level of medical school accreditation will ideally improve the rates of training in medical school.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.