
Abstract
Background:
Pregnancy complications may recur and are associated with potentially modifiable risks. The role of interconception preventive care in reducing repeat pregnancy complications is understudied.
Materials and Methods:
This retrospective cohort used 2007–2012 Medicaid claims from 12 states. Included women who had an index birth complicated by prematurity, hypertension, or diabetes, a subsequent birth within 36 months, and Medicaid eligibility for ≥11 of 12 months after index birth. Logistic regression assessed for an association between the exposure of preventive visits in the year after index birth and primary outcomes of prematurity, hypertension, or diabetes in the subsequent pregnancy. Regression adjusted for confounders including demographics (age, race and ethnicity, rural residence, state), index pregnancy features (complications, prenatal visits, multiple gestation, maternal and infant length of stay, year), visits to address complications in the index birth, and interpregnancy interval.
Results:
Of 17,372 women, mean age was 24.3 ± 5.3 years, and race/ethnicity was 50.3% non-Hispanic White, 27.2% non-Hispanic Black, and 11.9% Hispanic. In the index pregnancy 43.3% experienced prematurity, 39.2% experienced hypertension, and 34.2% experienced diabetes. In the year after the index pregnancy, 54.7% had at least one preventive visit. In the second pregnancy, 47.7% experienced prematurity, hypertension, or diabetes. Recurrence rates were 28.1% for preterm birth, 38.0% for hypertension, and 48.3% for diabetes. Preventive visits were associated with reduced hypertension in the subsequent pregnancy (OR 0.88, 95% CI 0.82–0.97) but not reduced preterm birth or diabetes.
Conclusions:
Preventive visits after an index birth complicated by prematurity, hypertension, or diabetes were associated with 10% lower odds of hypertension in a subsequent pregnancy, but not with reductions in diabetes or prematurity. Some complications may be more amenable to interconception preventive services than others.
Introduction
Preventive health care after birth includes postpartum visits to assess obstetrical recovery, routine adult health care, contraceptive services, and counseling to optimize health during subsequent pregnancies. It may also include secondary prevention involving management of complications of pregnancy or other chronic health conditions. 1 –6 These visits may occur with an obstetrical specialist or with any other clinician able to provide these services.
Pregnancy complications such as gestational diabetes, pregnancy-induced hypertension, and prematurity may recur across pregnancies, and are increasingly recognized as risk factors for long-term cardiovascular health for women. 7 –9 These common conditions are associated with modifiable risk factors, including but not limited to smoking, dietary habits, and obesity, that may be addressed during preventive visits. 4,10 High quality preventive health care may, therefore, be particularly significant after complications of pregnancy. Women with hypertension or diabetes during pregnancy are more likely to access preventive care in the year after birth, however, women with preterm birth are less likely to access care, compared to women without these complications. 11
Previous studies on recurrent pregnancy complications have not addressed the role of interconception preventive health care in modifying recurrence rates in subsequent pregnancies. 9,12,13 The goal of this study was to assess whether preventive care in the year after a birth was associated with decreased complication recurrence, in a heterogeneous population with regards to complications. Though pregnancy complications, and related chronic disease states, warrant disease-specific follow-up, the exposure of preventive care is potentially related to mitigation of common risk factors. A heterogenous population provides an opportunity to understand the potential role of general interconception preventive care in improving pregnancy outcomes among women with a high risk for subsequent pregnancy complications.
Materials and Methods
Population
This retrospective cohort used Medicaid Analytic eXtract (MAX) data maintained by the Centers for Medicare and Medicaid Services. MAX includes person-level data on Medicaid eligibility and utilization. 14 Our cohort included women aged 12–55 with two births from 2007 to 2012. This represented the most recent data available to our team. This study was reviewed and deemed exempt by the Institutional Review Board at the Children's Hospital of Philadelphia.
State-level inclusion criteria were intended to reduce bias by ensuring that included states were as close as possible to having complete encounter-level data available for all births. We included both fee-for-service and managed care claims from states with high-quality encounter-level data and with data that allowed high rates of linkage between mother and infant claims.
The quality of encounter-level data for each state was assessed using an established method in which each state's managed care data is compared to fee-for-service data. The rationale for this is that fee-for-service data underwent additional quality checks before release compared to other managed care data. 11,14,15 This ensures adequate encounter-level data in states with significant managed care populations. We required linkage of mother and infant claims to better classify preterm birth. These linkages relied on (1) maternal delivery stay or delivery date to infant date of birth, (2) Medicaid case number, and (3) zip code. We included women from 12 states (Alaska, Colorado, Indiana, Michigan, New Hampshire, New York, North Dakota, Oregon, South Dakota, Tennessee, Vermont, Wyoming).
Additional individual-level inclusion criteria (Fig. 1) supported our goal of examining the relationship between preventive health care after an index birth and subsequent pregnancy complications. First, we only included women with hypertension, diabetes, or preterm birth in the index pregnancy (see below for details regarding these classifications). Second, we included women with 11 or more months of Medicaid eligibility in the year after birth. This ensured that the exposure of preventive care would be available, and eliminated the influence of insurance, a predictor of utilization, from our analysis. Third, because benefits of preventive care in the year after birth may diminish with time, we included women with two births within 3 years.
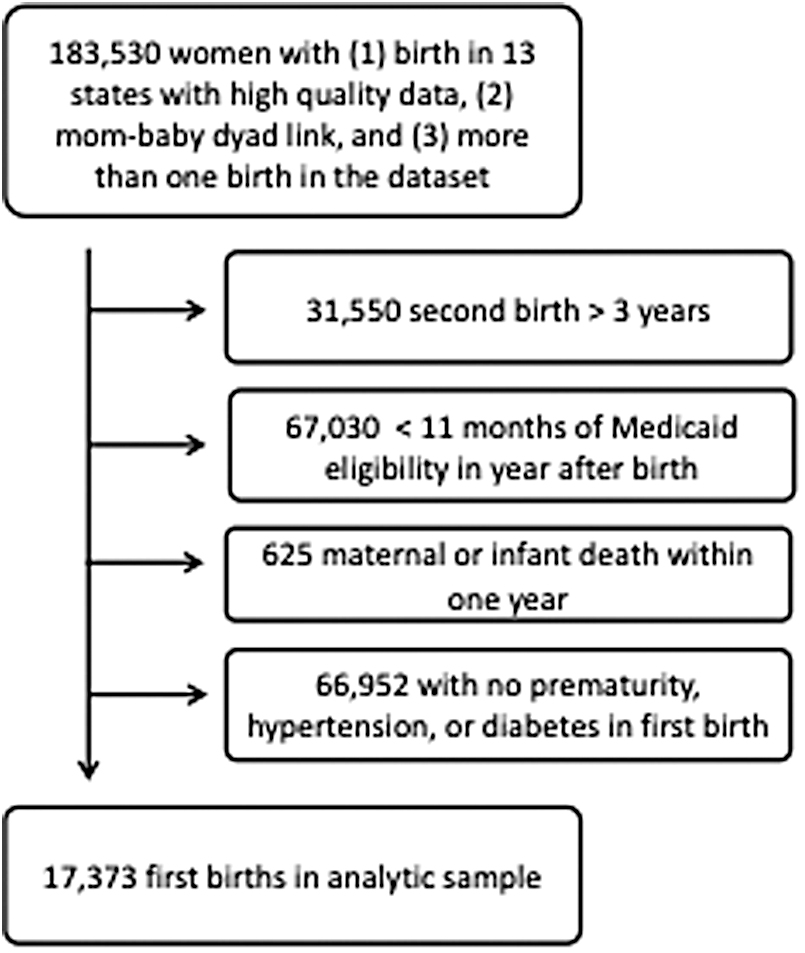
Construction of the cohort.
We did not have data on parity. We refer to these two births as the index birth and the subsequent birth. Fourth, we included women where both mother and infant survived the first year after index birth.
Exposure: Preventive visits in the year after index birth
Preventive visits were classified using ICD and CPT codes from outpatient visits in the year after index birth (Supplementary Table S1 details all definitions based on ICD and CPT codes). We included four visit types in our classification of preventive visits: postpartum visits, visits for contraceptive services, routine gynecological visits, and routine health maintenance visits.
Outcomes: Subsequent pregnancy complications
This study had three primary outcomes: diabetes, hypertension, and preterm birth in the subsequent pregnancy. Each condition was classified at two time points: during the index pregnancy and during the subsequent pregnancy. Diabetes and hypertension were dichotomized and based on either ICD or medication codes from pregnancy through 3 months postpartum (Supplementary Table S1). ICD code selection was based on prior studies using administrative data to assess these conditions or validate ICD-based classifications, and medication codes were identified based on treatment guidelines. 16 –20 Conditions could be classified based on a single ICD code with no medication codes.
When conditions were classified based on medications alone (i.e., women were prescribed medications commonly used to manage diabetes or hypertension, but had no ICD codes associated with these conditions) we required at least two occurrences of relevant medications. There are validated approaches to distinguish between pregnancy-associated and chronic hypertension and diabetes in administrative data. 17,18 We considered using this more granular classification, however, our data differed in key respects from prior validations, and we ultimately applied this distinction only during sensitivity analysis (Subgroup and Sensitivity Analyses). Classification of hypertension included codes for preeclampsia.
We identified preterm birth or low birth weight (later referred to as “preterm birth”) using ICD and CPT associated with short gestation or low birth weight. 21,22 Maternal and infant length of stay (LOS) at the subsequent birth, in days, were secondary outcomes.
Covariates
Analysis adjusted for factors that may be associated with both pregnancy outcomes and interconception preventive care. Covariate selection was based on prior birth outcomes literature and on Andersen's Model of Health Services Use, a theoretical model of health care utilization. 23,24 Andersen's Model focuses on need, predisposing, and enabling factors, at the individual or community level, as drivers of utilization.
Demographic factors are considered predisposing factors to health care use. We included age in years at the index birth as a categorical variable (<20 years, 20–24, 25–29, 30–34, and ≥35). Race and ethnicity were collapsed to Hispanic, non-Hispanic Black, non-Hispanic White, and other.
Health care use in other contexts is a predisposing factor for interconception care. 25 We therefore assessed the number of prenatal visits during the index pregnancy. We also assessed visits in the year after birth related to index pregnancy complications, specifically any visit coded for hypertension, diabetes, or prematurity. These visits may have occurred with obstetricians or other clinicians providing ambulatory visits for women. The content of these visits may have overlapped with preventive visit content (see above description of exposure variable). We considered these visits separately to minimize potential confounding by indication, where increased illness severity may be associated with both increased visit number and with potential subsequent adverse outcomes.
Geographic residence may be an enabling factor for health care use and may influence pregnancy outcomes. Residential zip codes eligible for programs under the Federal Office of Rural Health Policy were classified as rural. 26 We adjusted for residential state and year of birth to account for variations in Medicaid and other maternal-child health programs. Interpregnancy interval, in months, was considered. There is a potential bidirectional relationship between preventive health care after birth and short interpregnancy intervals. We included interpregnancy interval because we could not exclude its role as potential confounder in the relationship between preventive care and outcomes in a subsequent pregnancy.
We assessed health during the index pregnancy as markers of need. We included preterm birth, hypertension, and diabetes in the index pregnancy. We defined these conditions in the index pregnancy using the same strategy described above in classification of outcome variables. We also included mental health (depression or anxiety) identified with ICD codes during the index pregnancy, because we previously found these conditions were associated with increased interconception preventive care. 11 Maternal and infant LOS during the index pregnancy, in days, were included as markers of severity of perinatal complications, another component of need. Finally, we considered multiple gestations in either the index pregnancy or the subsequent pregnancy as two separate covariates.
Analysis
Analyses were conducted using Stata 16.0 (StataCorp, College Station, TX). 27 We examined analytic factors, comparing women with preventive visits and those without. We used t-tests to compare continuous variables and chi-squared tests to compare categorical variables. We assessed recurrence of preterm birth, hypertension, and diabetes between the index pregnancy and the subsequent pregnancy.
Association between preventive care and subsequent pregnancy complications
We conducted multivariable regression analysis to assess for a relationship between preventive care in the year after index birth and complications in a subsequent pregnancy within 3 years.
We used logistic regression for our primary outcomes of prematurity, hypertension, or diabetes, and linear regression for secondary outcomes of maternal and infant LOS. Each regression adjusted for maternal age, race, ethnicity, rural zip code, index pregnancy features including number of prenatal visits, multiple gestation, preterm birth, hypertension, diabetes, and mental health conditions, interpregnancy interval, complication follow-up (i.e., follow-up of index pregnancy complications), multiple gestation in the subsequent pregnancy, state of residence, and index birth year. In these regressions, we were also interested in the relationship between complication follow-up visits and subsequent pregnancy outcomes.
Subgroup and sensitivity analyses
There may be overlap between services delivered during preventive visits and during visits for follow-up of index pregnancy complications. Relatively few women had any visits to follow-up on complications. We conducted a subgroup analysis excluding women with any complication follow-up visit from our models to assess whether our findings were stable when excluding these possibly overlapping services.
We also conducted subgroup analyses in which we considered prematurity in the subsequent pregnancy only among those with prematurity in the index birth, hypertension only among those who had hypertension in the index pregnancy, and diabetes only among those with diabetes in the index pregnancy. We also assessed subsequent pregnancy outcomes in the subgroup with two or more complications in the index pregnancy.
We conducted several sensitivity analyses. First, because women with preventive care differed from women without preventive care to an extent that may not be well adjusted for using regression alone, we conducted propensity score matching to assess whether findings changed when using this method to account for potential differences between cohorts. 28 To do this, we created a propensity score by modeling the likelihood that women received preventive care based on maternal age, race, ethnicity, prematurity, hypertension, diabetes, and mental health conditions in the index birth, rural zip code, prenatal visits during the index pregnancy, state of index birth, and year of index birth. We stratified our match based on interpregnancy interval less than 1 year versus 1 year or greater. After generating a propensity score, we used the psmatch2 package in Stata 29 to match women with and without preventive visits based on propensity scores. 28
Using the matched cohort, we then proceeded with regression models that assessed for residual confounding, including covariates used in the match and interpregnancy interval, complication follow-up visits, and multiple gestation.
A second sensitivity analysis explored the classification of hypertension and diabetes, considering whether the findings changed if we defined these outcomes more narrowly, that is, as pregnancy-induced hypertension or gestational diabetes (as opposed to any hypertension or any diabetes) in the subsequent pregnancy. Compared to the main analysis, this analysis limited our definition of hypertension and diabetes by using ICD codes specific to pregnancy-related hypertension or diabetes. We also excluded women with any relevant medication use before the second trimester from definitions of pregnancy-related disease.
Third, various methods have been proposed to estimate the number of preventive visits in the postpartum period. 30 We considered an expanded definition of preventive visits that allowed us to count visits with CPT codes for preventive care but no associated preventive ICD codes (Supplementary Table S1).
Finally, we considered whether we could identify a dose response for preventive visits and improved outcomes in the subsequent pregnancy. Because of the right-skewed distribution of preventive visits, we did this by categorizing the preventive visits as 0, 1, and 2 or more.
Results
The full cohort consisted of 17,372 women. During the index pregnancy 7519 (43.3%) had preterm birth, 6902 (39.2%) had hypertension, 5937 (34.2%) had diabetes, and 2672 (15.4%) had more than one of these complications. Table 1 demonstrates characteristics of the full cohort and the cohort stratified by those with and without preventive visits. Fifty percent of the cohort was non-Hispanic White, 27.2% were non-Hispanic Black, and 11.9% were Hispanic. Overall, 9502 (54.7%) women had a preventive visit in the year after birth, with a median of 1 visit and a range of 0–14 visits. Only 1496 (8.6%) had a follow-up visit specific for a complication of the index pregnancy. The follow-up time, represented by the interbirth interval, ranged from 7–36 months, with a mean of 20.8 ± 7.2 months.
Characteristics of Women with Hypertension, Diabetes, or Preterm Birth in an Index Pregnancy, Stratified by Receipt of Preventive Visits in the Year After Birth
p-Values represent results of chi-squared tests for categorical variables and one-way ANOVA for continuous variables.
See Supplementary Table S1 for details of preventive visit definitions. Analyses use not expanded definition of preventive visits unless otherwise noted. The expanded definition of preventive visits counts visits that have either a preventive CPT code OR a preventive ICD code is considered as an outcome in sensitivity analysis.
IQR, interquartile range; LBW, low birth weight; LOS, length of stay; SD, standard deviation.
In this cohort of women with a complication of preterm birth, hypertension, or diabetes in the index pregnancy, 8299 (47.7%) also experienced a complication in the subsequent pregnancy (Table 2). Women with diabetes had the highest rate of recurrence, at 48.3%. This was followed by hypertension (38.0%) and preterm birth (28.1%). Most women who had complications in both pregnancies experienced the same complication in both pregnancies. However, 8.2% of women only experienced a complication in the subsequent pregnancy that they had not experienced in the index pregnancy.
Pregnancy Complications Across the First and Second Birth
Italic values represent recurrence of pregnancy complications.
Association of preventive care and subsequent pregnancy complications
Table 3 compares recurrent pregnancy complications between those with and without preventive visits. In multivariable regression, there was decreased odds of any pregnancy complication in the subsequent birth for women who had preventive visits (OR 0.92, 95% CI 0.86–0.98). This was driven by a decrease in odds of hypertension (OR 0.89, 95% CI 0.81–0.97). There was no association between preventive care and the other primary outcomes of preterm birth or diabetes. Preventive care was associated with statistically significant though clinically small reductions in maternal and infant LOS in a subsequent pregnancy (maternal LOS −0.13 days, 95% CI −0.21 to −0.06; infant LOS −0.67 days, 95% CI −1.20 to −0.13).
Association of Preventive Care in Year After Index Birth and Outcomes in Subsequent Pregnancy
Bold italics p-value <0.05; italics p-value <0.10. We used logistic regression for dichotomous outcomes (preterm birth, hypertension, diabetes), and linear regression for continuous outcomes (maternal and infant length of stay). Multivariable and matched sample regression also adjusted for maternal age, race, ethnicity, rural zip code, index pregnancy features, complication follow-up visits, state, and year of index birth, multiple gestations, and interpregnancy interval.
CI, confidence interval; OR, odds ratio.
In contrast to the primary exposure of preventive visits, follow-up visits specific to index pregnancy complications were positively associated with complications in the subsequent pregnancy (preterm birth OR 1.30, 95% CI 1.11–1.51; hypertension OR 2.28, 95% CI 2.00–2.60; diabetes OR 4.51, 95% CI 3.94–5.15).
Subgroup and sensitivity analysis
In subgroup analysis (Supplementary Table S3) excluding 8.6% of the cohort with complication follow-up visits, the effect size for the primary outcomes were stable (association between preventive care and hypertension in a subsequent pregnancy OR 0.91, 95% CI 0.83–1.00).
In separate subgroup analyses considering recurrence of each index pregnancy complication separately (Supplementary Table S3) effect sizes for the association between preventive visits and complication recurrence were stable compared to the full cohort analysis, though confidence intervals were wider. In particular, among those with preterm birth in the index pregnancy, the odds ratio of subsequent preterm birth among those with preventive visits versus no preventive visits was 0.95 (95% CI 0.86–1.06). The odds ratio for preventive visits versus no preventive visits and subsequent hypertension among those with index pregnancy hypertension was 0.90 (95% CI 0.81–1.01), and for subsequent diabetes among those with index pregnancy diabetes was 0.84 (95% CI 0.74–0.95). Similar results were found for the subgroup with two or more complications in the first pregnancy.
In sensitivity analyses, the direction of the associations and effect sizes were stable for the primary outcomes. In particular, for the association between the exposure of preventive care and the outcome of hypertension in a subsequent pregnancy, odds ratios ranged from 0.89 to 0.93 in the sensitivity analyses. In some cases, the statistical significance of the findings was reduced, possibly due to reduced statistical power in the sensitivity analyses.
Matching improved covariate balance on all measures between the women who received interconception care and those who did not (Supplementary Table S2), particularly race and ethnicity, rural zip code, prenatal visits, and index pregnancy complications. The matched cohort included 13,396 women. Findings were similar to the unmatched analysis for the association between preventive visits and all outcomes with the exception of a reduction in the effect size for the association between preventive care and infant LOS (Table 3).
Considering an outcome definition of pregnancy-induced hypertension or gestational diabetes in the subsequent pregnancy (Supplementary Table S4), we saw a similar effect size as the main analysis, with reduced odds of pregnancy-induced hypertension in the subsequent pregnancy after preventive visits (OR 0.93, 95% CI 0.84–1.04). Similarly, in a separate sensitivity analysis considering an expanded definition of preventive visits as the exposure of interest, the effect size remained stable suggesting reduced odds of pregnancy-induced hypertension in the subsequent pregnancy after preventive visits (OR 0.91, 95% CI 0.82–1.01). In both cases, the confidence intervals may have been widened because of decreased power.
When considering the exposure of preventive visits as a categorical variable (Supplementary Table S5) we found the greatest benefit to a small number of visits. We stratified at 0 visits (45.3% of the sample), 1 visit (34.5%), and 2 or more visits (20.2%). We found reduced odds of any complication in the subsequent pregnancy comparing one visit to none (OR 0.91, 95% CI 0.84–0.97). When comparing odds between those with 2 or more visit versus none, there was no change in odds (OR 0.94, 0.86, 1.02). This same pattern was observed when considering individual outcomes of prematurity, hypertension, or diabetes.
Discussion
In this cohort of women with index pregnancy complications, interconception preventive visits were associated with reduced hypertension in a subsequent pregnancy, and with clinically small reductions in maternal and infant LOS at the subsequent birth. To our knowledge, this is the first large cohort to link interconception preventive visits to subsequent pregnancy outcomes.
For Medicaid-insured women who experience prematurity, hypertension, or diabetes during pregnancy, our data suggest that half will experience a complication during their next pregnancy. Women should be offered information about potentially modifiable risks and access to evidence-based risk mitigation strategies. Particularly for women with hypertension during pregnancy, our findings support benefits from engagement in interconception preventive care. However, we note that half of the cohort had no complications in their subsequent pregnancy. This finding may be important for women who experienced difficult pregnancies and have concerns about future pregnancy outcomes.
Preventive care between pregnancies is intuitively appealing because optimal women's health before pregnancy is associated with improved pregnancy outcomes. 31 Yet we lack robust evidence identifying high value interconception services. Observational studies, such as ours, may be limited by inconsistency in care. Quality standards and consistent service delivery may be needed to fully realize and measure the potential of interconception care. Experimental strategies to evaluate interconception care, for example through encouragement designs, would also contribute to a more robust evidence base.
Our findings suggest that certain complications of pregnancy, particularly hypertension, may be more amenable to health care interventions than others. For some conditions, the tendency toward recurrence may be so high that preventing recurrence is not an appropriate goal for interconception care. Examining outcomes such as severe maternal morbidity 32 in subsequent pregnancies may better capture the value of interconception care. Additionally, examining preventive health care in the context of social determinants of health may strengthen future work.
Our analysis may have been subject to confounding by indication, in which women who had more severe complications were more likely to seek health services, including preventive care. We attempted to account for this by distinguishing between preventive visits and visits specifically intended to follow-up on index pregnancy complications, and by conducting a sensitivity analysis that excluded women with visits intended for follow-up of complications.
Notably, only 8.6% of our cohort completed visits specific to pregnancy complications, suggesting that secondary prevention is an underutilized strategy to reduce repeat pregnancy complications. However, a separate sensitivity analysis found that women in the middle quintiles for preventive visits had better subsequent pregnancy outcomes than those in the top quintile, and suggests that analyses remained subject to some confounding by indication. This type of confounding would tend to bias our main findings toward the null.
Our findings may also be subject to misclassification bias. With hypertension and diabetes, misclassification may occur because of billing errors or, in the sensitivity analysis, because of the clinical challenge of distinguishing between chronic and pregnancy-related conditions. Many women had ICD codes or medications related to both chronic and pregnancy-related hypertension or diabetes. Codes suggestive of chronic disease in the index pregnancy did not perfectly predict chronic disease in the subsequent pregnancy.
Others have validated use of administrative data to distinguish these conditions, but have done so with data that differ from the data we used. For example validations have used single hospital data, which may have more homogeneous billing practices than our data, or have used data that precede pregnancy, which is not consistently available for Medicaid-insured women. 16 –18 Because of concerns about potential misclassification, we chose to take an inclusive approach to classifying these conditions, and considered a more narrow definition as a sensitivity analysis.
Effect sizes remained consistent regardless of the definitions used, suggesting that the associations we found were not particularly sensitive to these concerns, at least in our data. Perhaps more importantly, our data could not distinguish between complications that were controlled versus those that were not. Health systems lack strategies to consistently deliver treatments that may prevent progression of pregnancy-related diabetes or hypertension to chronic conditions. 33 In addition, there are other potential risk factors for adverse birth outcomes, such as body mass index, that we were unable to address as they are not well identified by administrative claims. 34
Misclassification may also have occurred in our exposure of preventive visits, in that content may differ across visits billed similarly, weakening the signal of high-value preventive services. A sensitivity analysis considering differing definitions of preventive visits did not appear to change the observed associations. In addition, we did not account for potential variability in access to or utilization of preventive care beyond 1 year after birth. These analyses therefore may understate the benefits of high-quality preventive care focused on pregnancy-relevant health issues.
We included women with Medicaid insurance for a year after birth, and our data only extend through 2012, which may limit generalizability of our findings. Because of slow processing and release of MAX data, this is the most recent data available to our research team. The availability of consecutive years of claims and the national scope make this the strongest available data of which we are aware to address our research question. Many women in our sample likely had sustained Medicaid eligibility due to particularly low income or SSI eligibility. Compared to all births covered by Medicaid, our sample was more non-Hispanic White, and more likely to live in rural zip codes. 35 Subsequent Medicaid expansion in some states may have improved access since 2012.
Because we focused on women with Medicaid eligibility in the year after birth, our estimates may be appropriate to settings with expanded insurance coverage for postpartum women. In addition to Medicaid expansions, recent focus on the Fourth Trimester and management of cardiovascular risks in pregnancy may have improved the quality of care since our study period, in which case our findings may underestimate the current value of interconception preventive health care. 36 –39
Conclusions
Preventive visits in the year after index birth were associated with reduced hypertension in a subsequent pregnancy within 3 years, but not with reductions in prematurity or diabetes. Recurrence of pregnancy complications was common in this multistate sample of Medicaid-insured women. Women who experience pregnancy complications should have access to high-quality interconception health care, but may also require additional support to ensure optimal health in subsequent pregnancies and throughout the life course.
Footnotes
Authors' Contributions
All authors contributed to conceptualization of this research and interpretation of findings. Ms. Passarella and Dr. Gregory were responsible for data management and analysis. Dr. Gregory drafted the initial article. All authors reviewed and revised thearticle, approved it in this form, and agreed to be accountable for the work.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding sources.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Analysis was supported by the Health Services Research Administration, Maternal Child Health Bureau (R40MC31762). Data were provided via an agreement between the Centers for Medicare and Medicaid Services, a component of the U.S. Department of Health and Human Services, and the Children's Hospital of Philadelphia (CHOP) under project “Variations in Health and Health Outcomes for Medicaid Insured Patients” (DUA RSCH-2017-51234). Funding support for the data agreement was provided by the Harriet and Ronald Lassin Endowed Chair in Pediatric Neonatology at CHOP. Support was also provided by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number K23HD102560. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the U.S. Department of Health and Human Services.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.