
Abstract
Background:
To address the opioid epidemic, physicians are encouraged to identify means of reducing patient opioid exposure. Electronic medical records (EMRs) often include default order sets with automated orders for opioid medications, which may influence how much opioids physicians prescribe. We sought to evaluate the impact of de-selecting an automated order for oxycodone-acetaminophen from an EMR order set for postpartum vaginal deliveries on inpatient opioid exposure by comparing the proportion of patients who received an opioid after an uncomplicated vaginal delivery before and after the EMR change. As secondary outcomes, the impact on average total morphine milligram equivalents (MMEs) and discharge opioid prescriptions was investigated.
Materials and Methods:
A quality improvement study was conducted through retrospective chart review of uncomplicated vaginal deliveries for the four quarters before and after the EMR order set change occurred. The total proportion of patients who received an opioid in the postpartum period was then determined for the preexposure and postexposure groups. The total average MME consumed for patients who received an opioid in each group was determined and the total proportion of patients who received an opioid prescription at discharge was compared.
Results:
A total of 5826 records of uncomplicated vaginal deliveries met the criteria for analysis. In the preintervention group, 32.9% of patients received an opioid postpartum, compared to 12.5% of patients in the postintervention group, representing a decrease of 62.0% (p < 0.001). Of those who received opioids, the preintervention mean total opioid consumption was 28.4 MME (±27.6) compared to 33.6 MME (±46.4) postintervention, and there was no significant difference in median total opioid consumption: 22.5 MME (interquartile range [IQR]: 7.5–47.5) preintervention compared with 20.8 MME (IQR: 7.5–45.0) postintervention (p = 0.902). No significant difference was found with discharge opioid prescriptions between the two groups.
Conclusion:
Order sets within EMR systems appear to have a significant influence on physician prescribing behaviors and removing these automated orders for opioids should be considered.
Introduction
Opioid use is a major concern in the United States with epidemic levels of abuse. From 1999 to 2010, opioid-related deaths increased in parallel with opioid prescriptions. 1 While prescription rates plateaued in 2012 and have since started to decrease, the prescribing rates in the United States in 2015 were still three times higher than they were in 1999 and four times higher than Europe in 2015. 1,2 Physicians have been encouraged to identify and reduce overprescribing practices to reduce overall demand and abuse rates. 1
Specific to Obstetrics and Gynecology, opioids are commonly prescribed in the setting of postoperative pain control, which can present the opportunity for the improvement of opioid stewardship. One recent study suggested that among patients who received opioids at the time of gynecologic surgery, new persistent opioid use was found in 6.8% of patients 90 to 180 days after their procedure, in the absence of intervening surgical or anesthesia encounters. 3 Another found that a smaller percentage of opioid-naive women, about 1 in 300, would go on to develop persistent opioid use in the year following cesarean delivery. 4
For vaginal deliveries, several studies have shown ∼30% of women fill an opioid prescription in the peripartum period. 5 –7 In one large national analysis, about 4% of these patients went on to develop persistent opioid use. 6 Given ∼2.5 million vaginal deliveries occur annually, 8 the overall number of women this represents is higher than acceptable. As such, the American College of Obstetricians and Gynecologists (ACOG) recommends nonpharmacologic agents such as heating pads or ice packs in conjunction with oral analgesics such as acetaminophen and ibuprofen as first-line agents for postpartum pain after vaginal delivery. 9
Electronic medical records (EMRs) play a major role in ordering medications for patients, particularly through default order sets. These order sets not only help promote efficiency by bundling commonly needed orders and prescription quantities but they may also influence ordering habits. Several previous studies have demonstrated that providers are most likely to prescribe the default quantity of opioids as set in their EMR, 10 –13 suggesting that default order sets play a sizeable role in prescriber order habits. Within the field of obstetrics, it has been shown that an EMR change, which halved the dosage for post-cesarean oxycodone, resulted in a 56% decrease in opioid use 48 hours after delivery. 14
This is in line with evidence that opioids are likely overprescribed without actually improving pain outcomes, as one quality improvement study in a tertiary care center demonstrated that eliminating routine ordering of opioid medications significantly decreased opioid use without increasing pain scores. 15
Before 2016, the EMR at our institution (Cerner Powerchart) included an order set for postpartum vaginal deliveries with an automatically selected order for oxycodone-acetaminophen 5 mg/325 mg every 4 hours as needed for pain, which would need to be manually de-selected to not prescribe the medication. With the goal of improving opioid stewardship and decreasing unnecessary opioid exposure, this automatic selection was removed in February 2016. After this change, a physician would now need to actively check an additional box to order an opioid for postpartum care.
We hypothesized that the removal of a defaulted selection for oxycodone-acetaminophen within the postpartum order set would result in decreased opioid consumption among women after uncomplicated vaginal delivery. Second, as we expected fewer patients would have access to a standing opioid order, we anticipated this would also result in decreased average total morphine milligram equivalents (MMEs) for those patients who did receive an opioid, as well as fewer narcotic prescriptions on discharge.
Materials and Methods
We conducted a quality improvement study through retrospective chart review at our institution, a tertiary care center and 746-bed teaching hospital Phoenix, AZ, where, in 2016, there were 5575 deliveries, 4072 vaginal and 1503 through cesarean section. This project was reviewed and approved by the Institutional Review Board before the initiation of research. Data were obtained using current procedural terminology (CPT) codes for vaginal deliveries (CPT codes 59400, 59409, 59410, 59610, 59612, and 59614) for the four quarters before and after the order set change in February 2016.
We excluded patients delivered by cesarean section and with delivery complications or known reasons to require opioid medications, specifically current opioid use or history of opioid use disorder (ICD-10-CM code F11; ICD-9 304 and 305.5), postpartum tubal ligation (CPT code 58605), vacuum or forceps-assisted vaginal delivery (ICD-10-CM O81; ICD-9 669.5), third or fourth degree perineal lacerations (ICD-10-CM codes O70.2 and O70.3; ICD-9 664.2 and 664.3), uterine rupture or inversion (ICD-10-CM codes O71.0, O71.1, and O71.2; ICD-9 665.0, 665.1, and 665.2), intrauterine fetal demise (ICD-10-CM code O36.4; ICD-9 656.40), spontaneous abortion (ICD-10-CM code O03; ICD-9 634.9), and molar pregnancy (ICD-10-CM code O01.9; ICD-9 630).
Patients were divided into two groups by delivery date (pre- and post-February 2016). The medication administration record data were accessed for each patient. All opioid administration events were identified and patients were sorted by whether they received an opioid medication during the inpatient postpartum period. For the patients who did receive an opioid while inpatient, the total dosage consumed was calculated in MMEs and averaged between both groups.
As the order set change occurred within the month of February 2016, we considered deliveries from that month as part of the preintervention group. The fraction of patients receiving an opioid was then determined for both the preintervention and postintervention groups as a whole and as a month-by-month basis for the time period of the study.
Our primary outcome was the fraction of patients administered an opioid, while inpatient before and after the EMR change in February 2016. As secondary outcomes, we determined the average inpatient opioid dosage for those patients who received an opioid prescribed in MME both before and after the EMR change, as well as the total proportion of patients discharged with opioids in both groups.
Statistical methods
Descriptive statistics were used with continuous variables reported as means and standard deviations (SDs), or if the data were not normal, as median and interquartile range (IQR). Categorical variables were reported as number and percent. To compare the two time periods, chi square tests were used for categorical variables and Mann–Whitney U tests for continuous variables. In addition, a control chart was plotted for this interrupted time series and standard rules used to determine special cause variation. A p-value <0.05 was considered significant with no correction for multiple comparisons. IBM SPSS for MacIntosh, version 26.0 (IBM Corp., Armonk, NY), and QIMacros 2021, KnowWare International, Inc., were used for the analysis.
Results
A total of 9045 records returned from our initial database inquiry. Of these, a further 3219 records were found to include one or more exclusion criteria, resulting in 5826 records of uncomplicated vaginal deliveries for analysis.
The patient demographics are summarized in Table 1. There were no significant differences in age or racial make-up in both groups. More than half the patients reported Hispanic ethnicity and the mean age was ∼27 years in each group. Rates of obesity and gestational diabetes were slightly higher in the postintervention group, whereas the rate of preeclampsia was slightly higher in the preintervention group.
Patient Demographics
Represented as mean age with SD in parenthesis.
Represented as total number with relative percentage in parenthesis.
BMI, body mass index; SD, standard deviation.
The results are summarized in Table 2. For the primary outcome, 32.9% of patients of the preintervention group (n = 914 of 2775) received an opioid postpartum, compared to 12.5% of patients (n = 381 of 3051) in the postintervention group, representing a decrease of 62.0% (p < 0.001) and an absolute change of 20.4%. When graphed by month (Fig. 1), this decrease in rate is first apparent in February 2016 when the EMR change was made with 24.6% (n = 73 of 297) of patients receiving an opioid.
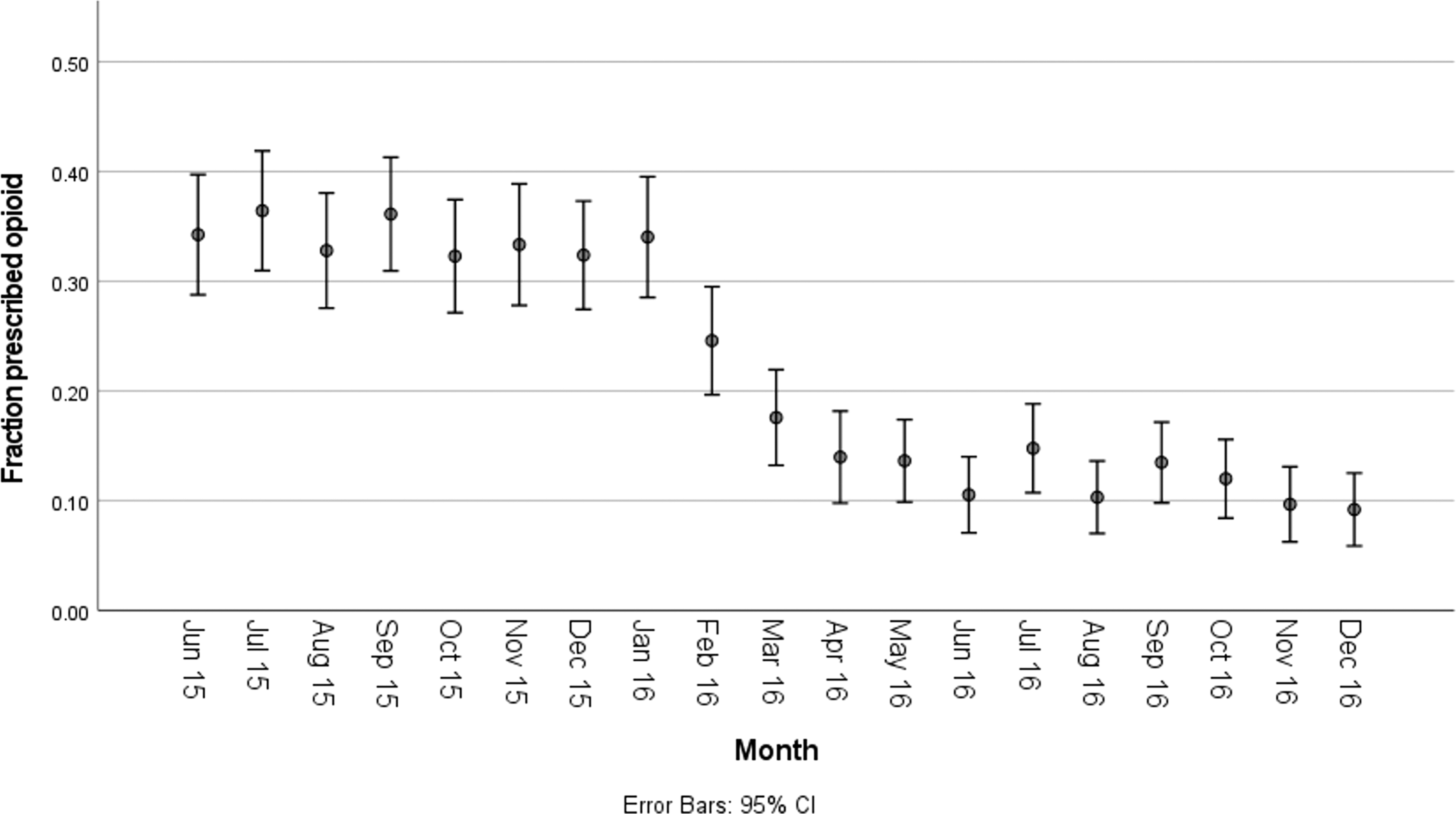
Fraction of patients after uncomplicated vaginal delivery, who received an opioid in the postpartum period, while inpatient (X-axis) by month (Y-axis).
Results
Represented as percentage of patients with total number in parenthesis.
Represented as mean MMEs with one SD in parenthesis.
Represented as median MME with IQR within parenthesis.
IQR, interquartile range; MME, morphine milligram equivalent.
A control chart was plotted and standard rules used to determine special cause variation (Fig. 2). All the following rules indicated that there was a significant change in rates after the intervention:

Control chart with proportions of patients receiving opioids before and after the intervention (X-axis) by month (Y-axis). Values and three SD confidence limits are plotted. SD, standard deviation.
One point beyond the three SD limit (of baseline limit)
Eight or more points on one side of the centerline (of baseline centerline)
Four out of five points outside of one SD
Two out of three points outside of two SD
Any noticeable pattern, cycle, or trend
The preintervention mean total opioid dosage consumed by patients who received an opioid was 28.4 MME (±27.6) and the postintervention mean total dosage was 33.6 MME (±46.4). However, as these data were not normally distributed, the median total dosage and IQR were evaluated. The preintervention median total dosage prescribed was 22.5 MME (IQR: 7.5–47.5) compared with 20.8 MME (IQR: 7.5–45.0) postintervention (p = 0.902). The mean total MME consumption was graphed by month in Figure 3.

Total mean MMEs consumed by patients who received an opioid before and after the intervention (X-axis) graphed by month (Y-axis). Values and two SD confidence limits are plotted. MMEs, morphine milligram equivalents.
Discharge opioid prescription rates were found to be similar between the preintervention and postintervention groups: the preintervention discharge prescription rate was 4.85% (n = 135 of 2786) and the postintervention rate was 4.42% (n = 135 of 3054) (p = 0.454).
Discussion
This successful quality improvement project showed that by removing a preset opioid order following vaginal delivery, fewer women used opioids postpartum. These results suggest that default orders in EMRs can have a significant impact on prescriber ordering habits, including opioid orders and subsequent administration. Our findings are consistent with previous studies 10 –13 that have suggested providers tend to order according to the default selections in EMR order sets. In general, these studies have evaluated how EMR preestablished orders have impacted the amount of opioids patients are provided at discharge or in the emergency department setting, where patients are provided a set quantity of medication for them to self-administer.
Building on this, our study demonstrates that the effect of EMR default orders extends to the inpatient setting, where medications are administered by nursing staff and “as needed,” or PRN medications must be requested. This effect can be significant, as removing the automatic for oxycodone-acetaminophen 5 mg/325 mg from our EMR led to a 62.0% decrease in patient opioid exposure during the study period, which accounted for over 600 expected patients in the postintervention group.
For those patients who did receive an opioid inpatient before and after the order set change, it would initially appear that these patients consumed a higher mean total opioid dose after the automatic order was removed (28.4 MME before compared to 33.6 MME postintervention). However, as the data did not conform to a normal distribution, parametric comparison between these groups was not possible. Therefore, the groups were compared by nonparametric testing and the median total MME was found to be similar between each group (22.5 MME and 20.8 MME preintervention and postintervention, respectively; p = 0.902).
To better visualize any trend, the mean total MME consumption was graphed by month (Fig. 3). Higher monthly mean MMEs were noted after February 2016, as well as an increase in the monthly SDs. While we had hypothesized that the absence of a standing opioid order would lead to decreased total consumption as fewer patients would have access to the medication “on-demand,” the comparable median MMEs suggest most patients exposed to an opioid postpartum consumed similar amounts before and after the EMR change. The increase in the mean MME likely reflects those patients with higher dosage requirements, which in a smaller patient population now contributes to a distribution that is skewed to the right. This is supported by the similar median MMEs and higher SD of the mean MME for the postintervention group (46.4 compared to 27.6 preintervention).
While we had anticipated that a decrease in inpatient opioid exposure would result in a decrease in opioid prescriptions at discharge, interestingly, there was no significant difference before and after the change to the EMR order set. Under 5% of patients were discharged with an opioid, which differs from other studies, and showed about 30% of women received an opioid prescription at discharge following a vaginal delivery. 5 –7 One factor in this may be that there is no automated component of our EMR regarding discharge opioid prescriptions. This contrasts with other described EMRs 10 –12 where a default quantity of opioids is proposed when ordering these medications. While providers are able to save their own preferred medication quantities, this amount is determined by the physician.
Another contributing factor may be a prescribing culture, which anticipates the need for opioids at the time of discharge for uncomplicated vaginal deliveries to be uncommon; however, this cannot be determined without more information regarding prescriber motivations. The similar rates of discharge prescriptions for both groups suggest either a baseline patient population with ongoing pain control needs or a prescriber ordering preference. More focused study would be needed to clarify why these patients continued to receive opioids, both inpatient and at discharge.
This order set change occurred during a time where efforts were underway to reduce opioid prescribing at the individual hospital, health care system, and statewide levels. While to our knowledge, there was no other intervention in effect at the time of the EMR change, many soon followed. Statewide reporting of outpatient opioid prescribing was mandated in May 2016. A statewide emergency was declared regarding the opioid epidemic in June 2017 and health care institutions were required to develop opioid administration policies and quality controls. 16
Subsequent legislation was signed in January 2018, which included surveillance of patient-filled prescriptions, electronic prescribing requirements, limitation of prescriptions to 90 MMEs, and educational sessions for physicians and medical students. 17 The general emphasis on better opioid stewardship that heralded these interventions may have contributed to decreased opioid prescribing behaviors during the time of our study; however, the temporal association of the EMR change with the significant decrease in inpatient opioid exposure makes it more likely that the observed impact was due to the removal of the automated order.
A strength of our project included the large numbers of deliveries over a relatively short time period. This permits us to evaluate ordering habits of generally the same group of providers and to control for shifts in prescribing preferences over the long term, although it does limit how this change compares to multiyear trends.
Our study is also limited in that there is no way to track how opioids were ordered, whether it was through the order set or not, nor identify specific provider ordering habits or motivations. It was also not designed to evaluate what impact this change in opioid ordering had on patient pain scores or satisfaction. While the automated order in question was oxycodone-acetaminophen 5 mg/325 mg, a more focused evaluation would be useful to evaluate which types of opioids were administered between each group to whether the order set change impacted ordering preferences.
As providers and institutions adopt multipoint strategies to improve opioid stewardship in response to the opioid abuse epidemic, a thorough review of EMR order sets that include automatic orders for these medications can serve as an effective quality improvement measure to decrease opioid exposure to a significant number of patients in the peripartum setting. Other studies 10 –13 have shown that prescribers will tend to prescribe the default quantities proposed by an EMR in discharge or outpatient settings.
In the inpatient postpartum setting, the simple act of requiring a prescriber to actively select for these medications in uncomplicated vaginal deliveries can further lead to a reduction in the number of patients who will receive an opioid medication. Clinical administrators and consensus groups with management responsibility over their respective EMR settings should consider the unconscious effects these default order sets can have on prescribers. Automatic orders for opioids should be avoided where appropriate and care should be employed in determining the lowest acceptable default quantity for outpatient prescriptions in EMRs that feature this setting. Routine monitoring of opioid prescribing habits can help identify what impact these settings have on patient opioid exposure.
To address the health care system's role in opioid overprescription, education for prescribing physicians and patient care teams regarding appropriate opioid administration and alternative pain management strategies should be provided in conjunction with removing automated opioid orders. An emphasis should be placed on creating a culture of mindful opioid stewardship where the need for these medications is reduced, patient exposure is minimized, and individuals are provided opioid quantities specific to their pain requirements.
Conclusions
Automatic order sets within EMR systems appear to have a significant influence on physician prescribing behaviors. Requiring a prescriber to manually select for an opioid medication for pain control in uncomplicated postpartum vaginal deliveries as opposed to employing an automated order is associated with a reduction in the number of patients who will receive an opioid medication while inpatient.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.