
Abstract
Background:
This study examined the association between Medicaid expansions under the Affordable Care Act (ACA) and births among low-income women of reproductive age in the United States.
Materials and Methods:
We used data from the 2008 to 2019 American Community Survey to estimate the association between state adoption of Medicaid expansion under the ACA and the percent of low-income women of reproductive age with a birth in the past year using a difference-in-difference research design. Subgroup analysis was explored by race and ethnicity, age group, educational attainment, marital status, and number of children.
Results:
We found that Medicaid expansion was associated with a small reduction in births among low-income women of reproductive age by 0.45 percentage points (95% confidence interval: −0.84 to −0.05). In subgroup analyses, we found reductions in births among Hispanic women, American Indian or Alaska Native women, women 25–29 years of age, women 35–39 years of age, unmarried women, and women with more than three children.
Conclusions:
Reductions in births associated with Medicaid expansion could suggest that expanding Medicaid addressed previously unmet reproductive health care needs among low-income women of reproductive age. The reductions in births among low-income women that we observe were occurring among some groups with higher unintended pregnancy rates, including Hispanic women, American Indian or Alaska Native women, young women, and unmarried women. These findings underscore the importance of reproductive health care access through insurance coverage on empowering women to have control over their reproductive decision-making and timing.
Introduction
Insurance expansions increase access to health insurance by extending coverage eligibility to populations that previously were not eligible. Recently, Medicaid expansion under the Affordable Care Act (ACA) expanded eligibility in favor of Medicaid coverage for low-income adults up to 138% of the federal poverty level (FPL) in states that chose to expand their programs, which had considerable effects on increasing insurance coverage among low-income women of reproductive age. 1
As a result of these coverage increases, studies have shown that adoption of Medicaid expansion under the ACA has been associated with increased access to family planning and contraceptive services. 2 –5 By expanding access to affordable contraception and family planning counseling, subsidizing medical care, and the general income transfer effect of insurance (i.e., allowing families to spend less on health care and more on other goods), Medicaid expansion may affect births among low-income women.
Prior studies of the association between public and private insurance expansions and births have found mixed results. 6 –10 Medicaid expansions for pregnant women have been associated with increases in births among some women, while Medicaid family planning waivers (limited to expansions for contraceptive coverage) have been associated with decreases in births among some women. 6,7 The ACA-dependent coverage provision, a private insurance expansion that allowed dependents to maintain coverage through a parent's plan until the age of 26, was associated with an overall decrease in childbearing among young adult women. 8 The Massachusetts health reform, which included an insurance mandate and subsidized private insurance coverage, was associated with fertility increases among married women and fertility decreases among unmarried women 20–34 years of age. 9
The ACA Medicaid expansion represents the largest contemporary expansion of health insurance to low-income people in the United States, providing eligibility for comprehensive coverage regardless of age, pregnancy, or parental status. As such, it is possible that the ACA Medicaid expansion has different or larger associations with births than other previous forms of public and private expansion, including earlier components of the ACA such as the dependent coverage provision. One previous study has explored this question: Palmer used birth certificate data and a simulated eligibility method to examine how the ACA Medicaid expansion and subsidized private insurance Marketplaces affected births among childless women. 10
Palmer found that subsidized private coverage was associated with increases in the birth rate, but no effect of the ACA Medicaid expansion on the birth rate among childless women. 10 However, this study included women of all incomes, which could have diluted effects among low-income women who were directly affected by the Medicaid expansion.
The objective of this study was to estimate the association between the ACA Medicaid expansions and births among low-income women of reproductive age, and identify differential effects by race, ethnicity, age group, education levels, marital status, and number of children. This article represents the second article to examine the effect of the ACA Medicaid expansions on births, using a different methodology, dataset, sample, and additional subgroup analyses than the previous work. 10
Evaluating the effects of the ACA Medicaid expansions on births can help to identify women's reproductive health care needs that may have been previously unmet before these health insurance expansions and inform Medicaid nonexpansion states of the potential benefits of expanding their Medicaid programs as well as potential effects of coverage expansions in the House-passed Build Back Better Act. Identifying the subgroups affected could enhance understanding for policymakers to craft policies that address women's reproductive health care needs.
Materials and Methods
Data
We used 2008–2019 person-level data from the American Community Survey (ACS) Integrated Public Use Microdata Series (IPUMS). IPUMS is the world's largest individual-level population database and provides U.S. census microdata for analysis at the person level. 11 These data have been used in past analyses of the relationship between insurance expansions and births. 9 All analyses were weighted using ACS-provided person weights. This study was determined to be not human subject research by the Columbia University institutional review board.
Sample and measures
We included low-income women of reproductive age 19–44 with household incomes at or below 138% of the FPL, the income threshold for Medicaid eligibility under the ACA Medicaid expansions. We limited our sample to women with available data for our outcome of interest (recent birth data were missing for 0.21% of the sample). Our outcome of interest was a binary indicator for having given birth in the past year, self-reported in the ACS.
Study design
We employed a quasi-experimental difference-in-difference research design to compare changes in births before and after the 2014 Medicaid expansions in Medicaid expansion states relative to nonexpansion states. Because problems can occur with staggered difference-in-differences that include variation in treatment timing, we restricted expansion states to only those that adopted Medicaid expansion in 2014. 12 We excluded six states—Alaska, Indiana, Louisiana, Montana, New Hampshire, and Pennsylvania—because of late Medicaid expansion adoption (Supplementary Table S1).
Statistical analysis
We estimated linear probability models for our difference-in-difference analysis, where the main predictor was an interaction between a binary indicator for state Medicaid expansion status and a binary indicator for whether it was before (2008–2013) or after (2015–2019) the 2014 Medicaid expansions. We excluded 2014 as a policy transition year, which helps to account for the lag in when we may see effects due to the duration of pregnancy and our outcome measuring births in the past year. All models included state and year fixed effects to control for time-invariant characteristics related to state residence or year that could affect births.
Adjusted models included covariates for women's age, marital status, race, Hispanic ethnicity, educational attainment, household number of own children (which could include children resulting from the recent birth), and residence in a metropolitan area. We also controlled for state-year level indicators for Medicaid family planning waivers (available from the Kaiser Family Foundation), 13 Medicaid waivers for abortion coverage (available from Guttmacher Institute), 14 the unemployment rate (available from the Bureau of Labor Statistics), 15 maximum monthly welfare benefits for a family of three (available from the Urban Institute Welfare Rules Database), 16 and state-mandated contraceptive coverage in private health insurance plans (available from the National Conference of State Legislatures and Guttmacher Institute). 17,18
We conducted stratified subgroup analysis by race and ethnicity (non-Hispanic black, Hispanic, non-Hispanic white, Indigenous—American Indian or Alaska Native, and Asian women), by age (19–25, 26–32, 33–39, and 40–44 years of age), by educational attainment (high school or less and more than high school), by marital status (married or not married), and number of children (one child or less, two to three children, or more than three children). There were no missing data for any covariate as the Census fully imputes missing data. We used heteroskedasticity-robust standard errors clustered by state to account for within-state correlation of error and the state-level variation in Medicaid expansion adoption.
We additionally conducted analyses to assess the assumptions for our difference-in-difference models, including plotting trends over time, pretrend tests overall and by subgroup, and event study models (Fig. 1; Supplementary Tables S2 and S3; Supplementary Fig. S1). These analyses examining the parallel trend assumption can confirm that even if states that chose to adopt Medicaid expansion may be different from nonexpansion states, the prepolicy trends are similar between the groups, and differences in trends in the postpolicy can therefore be attributed to the policy change.
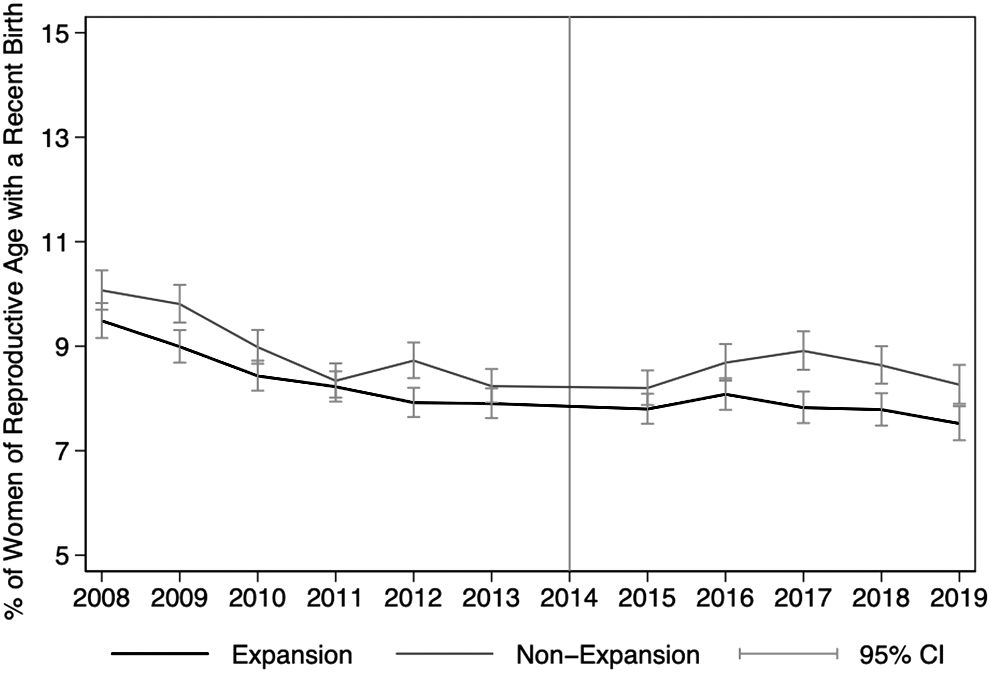
Unadjusted Trends in Percent of Low-Income Women of Reproductive Age with a Recent Birth, 2008–2019. Notes: Authors' analysis of data from the ACS. Data are weighted using ACS-provided person weights. ACS, American Community Survey; CI, confidence interval.
Exploratory analysis
Following previous analyses of the association between insurance expansions and births, we additionally explored if the ACA Medicaid expansions were associated with any change in abortions as an exploratory outcome, as abortion is a potential pathway through which insurance could affect births. 6,19 We used state-level abortion data from the Centers for Disease Control and Prevention (CDC) Abortion Surveillance System for the years 2009–2018, which included all years of data available (Supplementary Table S4). 20 These data are requested by the CDC from central health agencies for all states, and include the number of legal induced abortions by maternal state residence. 20 CDC natality data were used to calculate the abortion ratios for each state and year, measured as the number of abortions per 1,000 live births. 21
State abortion data were flagged as potentially unreliable or missing for California, Delaware, the District of Columbia, Florida, Maryland, and New Hampshire for one or more of the years 2009–2018 (additional explanation available in Supplementary Table S4). As a result, we presented results with and without these states for the abortion analyses to present results from analyses limited to states with data consistently available for the 2009–2018 study period. Following main analyses, we limited expansion states to those that expanded Medicaid in 2014 (thereby excluding Alaska, Indiana, Louisiana, Montana, New Hampshire, and Pennsylvania) and excluded 2014 as a policy transition year. We included state and year fixed effects and adjusted for all state-level covariates previously described for the main models.
Sensitivity analysis
First, as research indicates that the ACA-dependent coverage provision was associated with reductions in childbearing among young adults, we conducted a sensitivity analysis, excluding respondents 26 years of age and younger, who may have gained coverage under the dependent coverage provision (Supplementary Table S5).
Second, to verify that our results were not driven by differences between Medicaid expansion and nonexpansion states, we included a sensitivity analysis limiting the states to geographically similar expansion and nonexpansion states, with a more balanced total of 12 expansion and 13 nonexpansion states (Supplementary Table S6). Third, we replicated our main analysis among women of reproductive age with incomes above 400% of the FPL, whose coverage eligibility would not be affected by the ACA as a placebo check (Supplementary Table S7).
Finally, previous research using the ACS found that reports of a birth in the past year did not perfectly align with reports of women living with an infant of their own who is <1 year old in their household. 9 These researchers attribute these discrepancies to infants not living with their mothers as well as potential confusion regarding the survey question. 9 To confirm that our results are robust to both approaches of identifying recent births, we conducted a sensitivity analysis using the outcome of women reporting living with an infant of their own who is <1 year of age in the household (Supplementary Table S8).
Results
We identified a total of 1,096,043 women of reproductive age with household incomes at or below 138% of the FPL. Table 1 exhibits the baseline prepolicy characteristics of low-income women of reproductive age residing in Medicaid expansion and nonexpansion states. In the prepolicy period, a lower proportion of women were non-Hispanic black (17.06 compared to 27.96) and a higher proportion of women were Hispanic (18.98 compared to 13.89) in expansion states than in nonexpansion states. In addition, more women in expansion states lived in central metropolitan areas (23.90 compared to 14.22) and noncentral metropolitan areas (24.02 compared to 16.23) than in nonexpansion states, where more women lived in areas that were not metropolitan or mixed.
Baseline Characteristics of Low-Income Women of Reproductive Age, by State Medicaid Expansion Status
Notes: Authors' analysis of data from the ACS. Data are weighted using ACS-provided person weights. The baseline period represents the prepolicy years 2008–2013. Chi-square tests are presented to assess differences in characteristics.
ACS, American Community Survey.
Figure 1 shows the unadjusted trends in the percent of low-income women of reproductive age with a recent birth by state Medicaid expansion status. There were similar levels in expansion and nonexpansion states before the 2014 Medicaid expansions, with recent births occurring among 8.45% of low-income women of reproductive age in expansion states and among 8.98% in non-expansion states.
Table 2 presents the estimated changes in the percent of low-income women of reproductive age having a recent birth associated with Medicaid expansion. There was a small, but significant decrease of 0.45 percentage points (95% confidence interval [CI]: −0.84 to −0.05) in the percent of low-income women of reproductive age having a recent birth associated with Medicaid expansion, representing a 5.33% decrease from the prepolicy baseline of 8.45% in expansion states.
Difference-in-Difference Estimate of the Association Between Medicaid Expansion and Percent of Low-Income Women of Reproductive Age with a Recent Birth, 2008–2019
Notes: Authors' analysis of data from the ACS. Data are weighted using ACS-provided person weights. The baseline period represents the prepolicy years 2008–2013. All models include state and year fixed effects. Adjusted models include age, marital status, race, Hispanic ethnicity, educational attainment, household number of own children (including children from the recent birth), residence in a metropolitan area, presence of a Medicaid Family Planning Waiver, Medicaid abortion coverage, the unemployment rate, maximum welfare benefits, and state mandates for private contraceptive coverage. Heteroskedasticity-robust standard errors are clustered by state. 95% CIs and p-values are presented.
p < 0.05.
CIs, confidence intervals.
In subgroup analyses by race and ethnicity, we find significant decreases in the percent of low-income women of reproductive age having a recent birth associated with Medicaid expansion among Hispanic women, with a decrease by 0.98 percentage points (95% CI: −1.69 to −0.26), a 9.10% decrease from the baseline mean, and among American Indian or Alaska Native women, with a decrease by 2.78 percentage points (95% CI: −5.38 to −0.02), a 23.38% decrease from the baseline mean (Table 3). In subgroup analyses by age group, there were significant decreases in the percent of women having a recent birth among women 25–29 and 35–39 years of age, with more sizeable reductions of 1.57 percentage points associated with Medicaid expansion (95% CI: −2.62 to −0.52) among women 25–29 years of age, a 11.83% decrease from the baseline mean (Table 4).
Difference-in-Difference Estimates of the Association Between Medicaid Expansion and Percent of Low-Income Women of Reproductive Age with a Recent Birth by Race and Ethnicity, 2008–2019
Notes: Authors' analysis of data from the ACS. Data are weighted using ACS-provided person weights. The baseline period represents the prepolicy years 2008–2013. All models include state and year fixed effects. Adjusted models include age, marital status, educational attainment, household number of own children (including children from the recent birth), residence in a metropolitan area, presence of a Medicaid Family Planning Waiver, Medicaid abortion coverage, the unemployment rate, maximum welfare benefits, and state mandates for private contraceptive coverage. Heteroskedasticity-robust standard errors are clustered by state. 95% CIs and p-values are presented.
p < 0.05, ** p < 0.01.
Difference-in-Difference Estimates of the Association Between Medicaid Expansion and Percent of Low-Income Women of Reproductive Age with a Recent Birth by Age Group, 2008–2019
p < 0.10, * p < 0.05, ** p < 0.01.
Among women who were not married, there were significant decreases in the percent having a recent birth by 0.46 percentage points associated with Medicaid expansion (95% CI: −0.81 to −0.10), a 6.43% decrease from the baseline mean (Table 5). There were significant decreases in the percent of women with more than three children having a recent birth by 3.10 percentage points associated with Medicaid expansion (95% CI: −4.97 to −1.21), a 16.86% decrease from the baseline mean.
Difference-in-Difference Estimates of the Association Between Medicaid Expansion and Percent of Low-Income Women of Reproductive Age with a Recent Birth by Education, Marital Status, and Number of Children, 2008–2019
Notes: Authors' analysis of data from the ACS. Data are weighted using ACS-provided person weights. The baseline period represents the prepolicy years 2008–2013. All models include state and year fixed effects. Adjusted models include age, marital status, race, Hispanic ethnicity, educational attainment, household number of own children (including children from the recent birth), residence in a metropolitan area, presence of a Medicaid Family Planning Waiver, Medicaid abortion coverage, the unemployment rate, maximum welfare benefits, and state mandates for private contraceptive coverage. Heteroskedasticity-robust standard errors are clustered by state. 95% CIs and p-values are presented.
p < 0.10, * p < 0.05, ** p < 0.01.
Exploratory and sensitivity analyses
In exploratory analyses, we did not find evidence of significant changes in abortions associated with Medicaid expansion (Supplementary Table S4). In our sensitivity models examining births only among women older than 26 years, only among geographically matched states, and using living with an infant of their own who is <1 year of age in the household as the outcome rather than a report of a birth in the last year, we find decreases associated with Medicaid expansion that were largely similar to main models in magnitude and statistical significance (Supplementary Tables S5, S6, and S8).
In our placebo check among women with incomes 400% of the FPL or higher, who would not have been eligible for any subsidized insurance under the ACA, we found no evidence of significant changes in births among women who were not eligible for the ACA Medicaid expansions (Supplementary Table S7).
Discussion
In our difference-in-difference analysis for the years 2008–2019, we found that Medicaid expansion was associated with a small reduction in births among low-income women of reproductive age. Recent analyses of 2017–2019 Behavioral Risk Factor Surveillance System data indicated that almost one-third of women with ongoing or potential needs for contraceptive services were not using any contraceptive method, suggesting unmet needs for family planning services. 22
Our estimate indicates that Medicaid expansion was associated with an almost 5% decrease in births among low-income women, which could potentially stem from reductions in unintended pregnancies associated with Medicaid expansion, which prior research has suggested. 23 It is estimated that 30.4% of pregnancies were unintended as of 2018, 24 with research showing considerably higher rates of unintended pregnancies among low-income women. 25
Our results suggest that the reductions in births among low-income women that we observe were occurring among some groups with higher unintended pregnancy rates, including Hispanic women, American Indian or Alaska Native women, young women, and unmarried women. 25,26
We did not find any evidence that the ACA Medicaid expansions were associated with a reduction in births among women with no prior children of their own in the household, which is consistent with the prior research examining the ACA Medicaid expansions and births found no associated changes in the birth rate among women without previous children. 10 In addition, we find no evidence of changes in abortions associated with Medicaid expansion, which is consistent with research on earlier insurance expansions. 6,19 Under the Hyde amendment, federal money cannot be used to fund abortion access under Medicaid unless there are extreme circumstances, but states can use their own money to fund abortions in their Medicaid programs. 27
As of 2021, 16 states cover all or most medically necessary abortions in their Medicaid programs. 14 Prior research found that the ACA Medicaid expansion in one state that covers abortions in their Medicaid program, Oregon, was associated with increases in Medicaid-financed abortions. 28 Although we considered exploring abortions only among states that cover abortions in their Medicaid programs, there was only one state that covered abortions and did not expand Medicaid, so our results would have been too limited to make any conclusion with this dataset and approach.
The reductions in births associated with Medicaid expansion that we observe could suggest that expanding Medicaid addressed previously unmet reproductive health care needs among low-income women of reproductive age. Other research has found that Medicaid expansion decreased uninsurance among low-income women of reproductive age by ∼13 percentage points, 1 increased use of long-acting reversible contraception by 1.2 percentage points, 4 and increased access to birth control and family planning services among 35.5% of reproductive-aged women enrolled in Medicaid among respondents surveyed in Michigan. 2
Through these pathways, our findings could indicate that the previously documented increased access to contraceptive services 2 –5 and the reduction in unintended pregnancies 23 led to a reduction or delay in births among low-income women.
These results have implications for coverage policies, highlighting the effects that improved access to contraception through insurance coverage can have on births. Research on the effects of coverage policies is especially important in light of the July 2020 Supreme Court decision to uphold broader exemptions to the ACA contraceptive coverage mandate for private insurance, which could leave more women without coverage for family planning services and with less control over their births.
Limitations
This study had several limitations. We are unable to identify the specific mechanism leading to the reduction in births that we observe in this study. The ACS does not measure contraceptive use, abortions, or pregnancy intention. As a result, we could refer to existing ACA Medicaid expansion literature for the pathways through which births could be reduced by Medicaid expansion, but we could not conclude the exact causal pathways for our sample. On this note, we explored abortions as one potential pathway through which births could have been affected using additional CDC Abortion Surveillance System data and CDC natality data to calculate the state-level abortion ratio per 1,000 live births.
These abortion estimates were not restricted to women with Medicaid-eligible incomes, which could underestimate potential effects of Medicaid expansion on abortions among low-income women. In addition, we could not limit abortion analyses in these data to only states that cover abortions in their Medicaid programs, which is where any effect of Medicaid expansion on increased abortions would be expected to be. However, we found no evidence of an association between Medicaid expansion and increased abortion overall, with negative point estimates that were not statistically significant in our difference-in-difference analyses. Because of the limitations of our abortion analyses, we considered this to be an exploratory analysis.
In addition, although the ACS allowed us to use a large sample of low-income women of reproductive age (N = 1,096,043), we may still have remained underpowered for some subgroup analyses.
Finally, the ACA contraceptive coverage mandate, which required all new health insurance plans to cover contraception without costs, was issued in 2012 during the study period. Effects of this 2012 mandate should be absorbed by year fixed effects; however, it is possible that any privately insured individual in the comparison group gaining contraceptive access through this mandate could dampen effects of the ACA Medicaid expansions on births, as contraceptive access would increase among insured individuals in these nonexpansion states.
Conclusions
This study suggests new evidence that the ACA Medicaid expansions were associated with a small reduction in births among low-income women of reproductive age, with reductions among Hispanic women, American Indian or Alaska Native women, women 25–29 years of age, unmarried women, and women with more than three children, many of whom are groups that experience higher rates of unintended pregnancies. 25,26 These reductions in births could suggest that reproductive health care needs were going unmet among low-income women of reproductive age before Medicaid expansion, and Medicaid expansion enabled women to better control their family planning.
We found no evidence of increased abortions associated with the ACA Medicaid expansions, suggesting pregnancy prevention efforts as a more likely pathway through which Medicaid expansion could be associated with reductions in births overall. The findings in this study underscore the importance of reproductive health care access through insurance coverage on empowering women to have control over their reproductive decision-making and timing.
Footnotes
Acknowledgments
These authors acknowledge Julien Teitler, Kristen Underhill, and Jane Waldfogel for feedback on earlier drafts of this article.
Authors' Contributions
All authors meet the requirements of authorship, including substantial contributions to the conception and design of the analysis, drafting and revising the article, and final approval of the article.
Author Disclosure Statement
The authors have no competing interests or conflicts of interest to declare.
Funding Information
This work was supported by the Horowitz Foundation for Social Policy, the Social Work Healthcare Education and Leadership Scholars Fellowship, and the Center on Poverty and Social Policy at Columbia University.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.