
Abstract
Objectives:
The HEART Pathway is a diagnostic protocol designed to identify low-risk patients with chest pain who can be safely discharged from the emergency department (ED) without hospitalization. Studies have reported a negative bias in identifying myocardial ischemia in females versus males and a different clinical pattern of cardiac ischemia across genders. This study sought to determine if the HEART Pathway recommendations are affected by negative bias in females.
Materials and Methods:
A retrospective cohort study was conducted in the ED of an academic tertiary medical center. Admission/discharge decisions made by physicians in male and female patients presenting with chest pain in 4/2014–7/2019 were compared with HEART Pathway protocol predictions. Probabilities were estimated with logistic regression analysis, and odds ratios and 95% confidence intervals were calculated.
Results:
The cohort included 772 patients, 485 male (63%) and 287 female (37%), of median age 54 years. On the basis of their presenting symptoms, 278 patients (36%) were admitted by the ED physician and 494 (64%) were discharged. Using the HEART Pathway protocol, 227 patients (29.4%) would be expected to be admitted and 545 (70.6%) discharged. The real-life admission rate was higher than possible with the HEART Protocol (p = 0.001). In a regression model, male sex was a significant factor favoring admission among the patients for whom the HEART Pathway predicted admission (p = 0.007).
Conclusions:
As the HEART Pathway is a validated risk-stratification tool, there is a high likelihood that serious coronary artery disease may be overlooked in women, even those who seek timely medical assistance.
Introduction
Chest pain is associated with a high morbidity and mortality burden and is one of the leading reasons for emergency department (ED) visits in developed countries. 1,2 A recent multicenter study of patients presenting to the ED with chest pain, left arm pain, shortness of breath, epigastric pain, or other complaint suggestive of ischemic heart disease found that 17% were ultimately diagnosed with myocardial ischemia. Of these, more than 2% were erroneously discharged from the hospital. 3 Thus, the daily task of identifying patients at risk of myocardial ischemia while trying to avoid redundant hospital admissions and workup is a major challenge of ED physicians.
The HEART Pathway is a diagnostic protocol designed to facilitate the early discharge of patients presenting with chest pain who are at low risk of a major adverse cardiac event in the following 6 weeks. The protocol combines a clinical HEAR score (history, electrocardiography [ECG] changes, age, and cardiovascular risk factors) and with two consecutive high-sensitive troponin T levels (<13 ng/L) at presentation and 3 hours later. The HEART Pathway has been found to be safe for the identification of patients requiring admission or discharge. Use of the protocol led to a 6% decrease in admission rates without an increase in myocardial-infarction-related deaths. 4,5
Various studies have reported a negative bias in identifying myocardial ischemia in females versus males and a different clinical pattern of cardiac ischemia across genders. 6 –10 Reasons suggested for the bias included varying presentation of myocardial ischemia among females and the tendency of both patients and physicians to attribute the various symptoms to causes other than myocardial ischemia. 10
The aim of this study was to determine if the HEART Pathway recommendations are affected by negative bias in females.
Materials and Methods
Study design
A retrospective cohort study was conducted to compare real-life physician admission and discharge decisions in men and women presenting to the ED with chest pain with the expected outcomes using the HEART Pathway diagnostic protocol. Patients were retrospectively accrued by search of the health care database of Rabin Medical Center, a tertiary university-affiliated hospital. The study was approved by the Institutional Review Board of Rabin Medical Center with waiver of informed consent (IRB -0140-19-RMC).
Study setting and population
Visits to the ED of Rabin Medical Center number about 100,000 per year. The population of this study included adult patients who presented to the ED between April 2014 and September 2019 with chest pain but without evidence of ST-segment-elevation myocardial infarction and who underwent two consecutive high-sensitive troponin T blood tests (<13 ng/L) at presentation and after 3–4 hours with negative results.
Patient and public involvement
No patient involved.
Data collection
Data on complaints at presentation, findings on medical history, laboratory tests, and ECG, and presence of risk factors were extracted from the Rabin Medical Center electronic patient record system.
HEART Pathway assessment
The HEART Pathway algorithm 4 is depicted in Figure 1. HEART scores were retrospectively determined on the basis of the patients' electronic records.
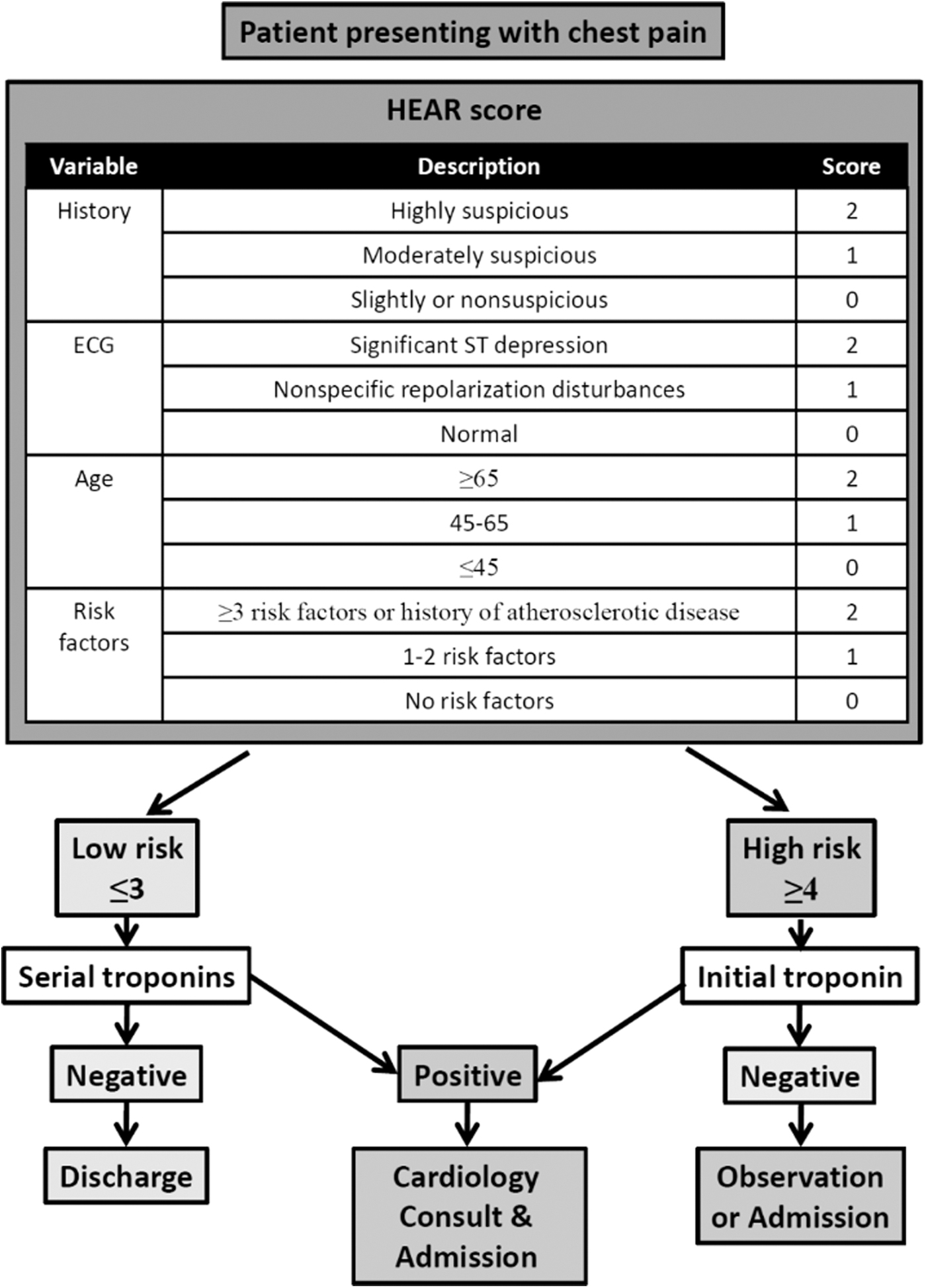
HEART Pathway protocol.
Patient history was scored according to the description of the hospital case manager physician during the ED visit. If HEART terms or similar not used, the history was scored as highly suspicious if the patient presented with typical pain symptoms (left sided or retrosternal chest pain, pain radiating to the jaw, neck or left arm, and exercise-induced pain), and as nonsuspicious, if the patient presented with atypical pain symptoms (pain worsening on palpation, breathing, or change in posture, right-sided pain, no radiation of pain to other sites, and no relation of pain to exercise). In patients presenting with both typical and atypical symptoms, the history was scored as moderately suspicious.
Admission ECG results were scored according to the description of the hospital case manager physician during the ED visit. If HEART terms or similar were not used, the ECG was scored 2 points if it showed new significant ST-segment depression or 1 point if it showed nonspecific ST-segment or T wave changes or other changes not diagnostic of ischemia.
Cardiovascular risk factors were taken into account if previously recorded in the patient's electronic medical record or stated during the ED visit.
High-sensitive Troponin T blood levels were tested in the Rabin Medical Center Biochemistry Laboratory, and the results were derived for the study from each patient's electronic medical record. The cutoff level for a negative result was set at <13 ng/L.
End points
The main end point of this study was the discharge/admission decision of the physician at termination of the ED visit. The Rabin Medical Center ED does not have an observation unit, but patients may be referred for coronary computed tomography (CT) instead of being admitted for further workup. For this study, patients immediately referred for coronary CT were grouped together with patients who were admitted, as were patients who refused admission despite the physician's advice.
Statistical analysis
All data were analyzed with SAS, version 21.0. Student's t-test was used to compare admission and discharge rates between men and women, and chi-square test was used to assess the relationship between sex and pain intensity and attribution. Data are presented by number and percentage or mean and standard deviation. Univariate and multivariate logistic regression analysis was applied to estimate the odds ratio (OR) (and 95% confidence interval [CI]) of a man or woman with chest pain being discharged/admitted according to the HEART Pathway protocol and traditional cardiovascular risk factors.
Results
Patients
Of 3450 patients assessed for eligibility during the study period, 772 were included in the cohort, 485 male (63%) and 287 female (37%). Median patient age was 54 years (range 18–90 years). The characteristics of the patients stratified by gender are summarized in Table 1. After evaluation in the ED, 494 patients (64%) were discharged and 278 (36%) were admitted.
Characteristic of Patients Presenting with Chest Pain
BMI, body mass index; CVA, cardiovascular accident; IHD, ischemic heart disease; PVD, peripheral vascular disease.
ED visit outcome by sex
There was no significant difference in rates of admission and discharge between men and women (P = 0.407, Fig. 2).
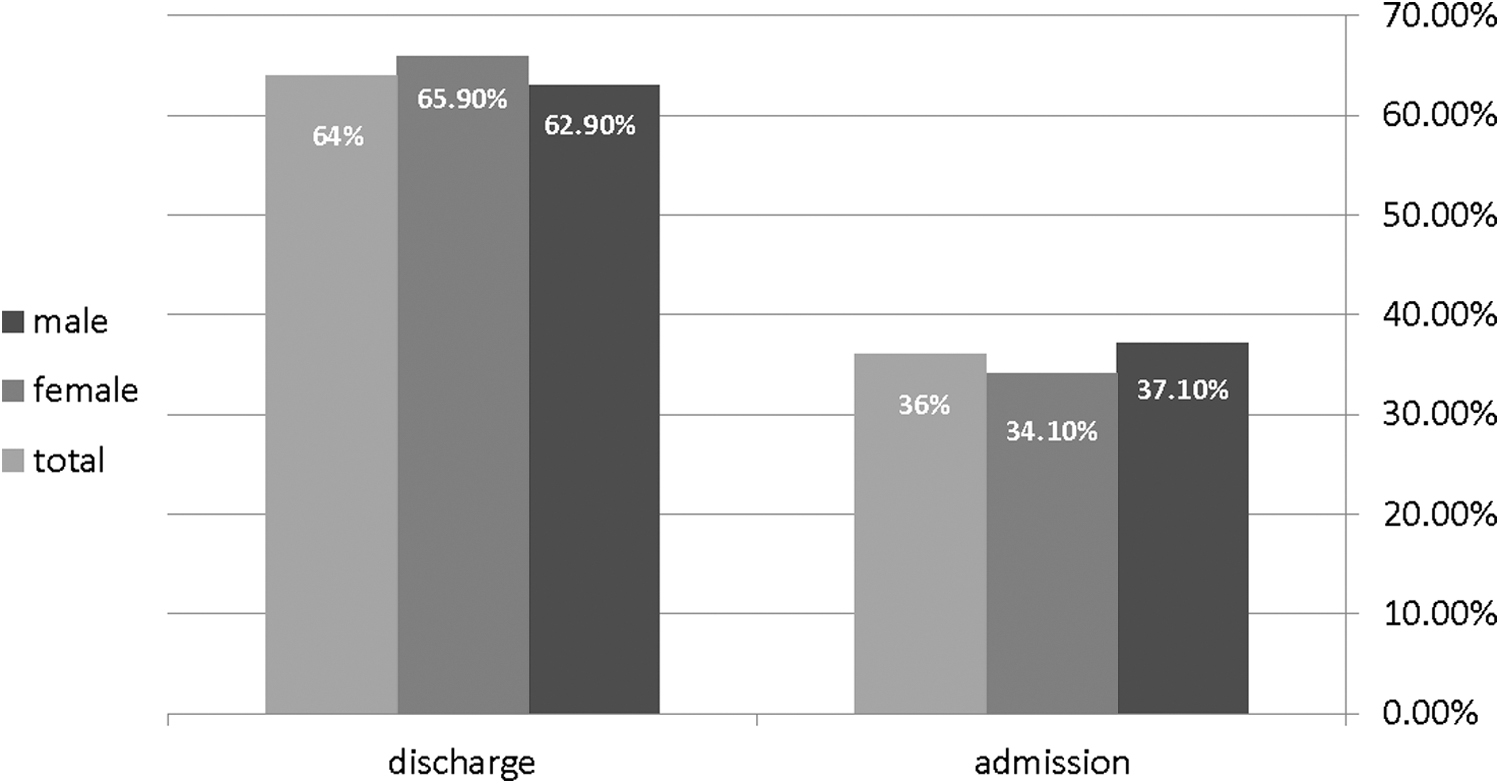
ED visit outcome by gender. No significant difference was found in ED visit outcome between genders (p = 0.407). ED, emergency department.
ED visit outcome by risk factors
On univariate regression analysis of discharge/admission decisions by cardiovascular risk factors, total cohort and by sex, all risk factors were significant for admission in the cohort and in male patients, except family history of ischemic heart disease and past history of cerebral vascular accident. In female patients, only hypertension and personal history of ischemic heart disease were significant predictors of admission (OR 0.5, 95% CI 0.30–0.83 and OR 0.5, 95% CI 0.26–0.95, respectively; Table 2 and Fig. 3). On multivariate regression analysis, of discharge/admission decisions by cardiovascular risk factors and by sex, all risk factors were significant for admission in the cohort and the risk kept in male patients (p = 0.017).
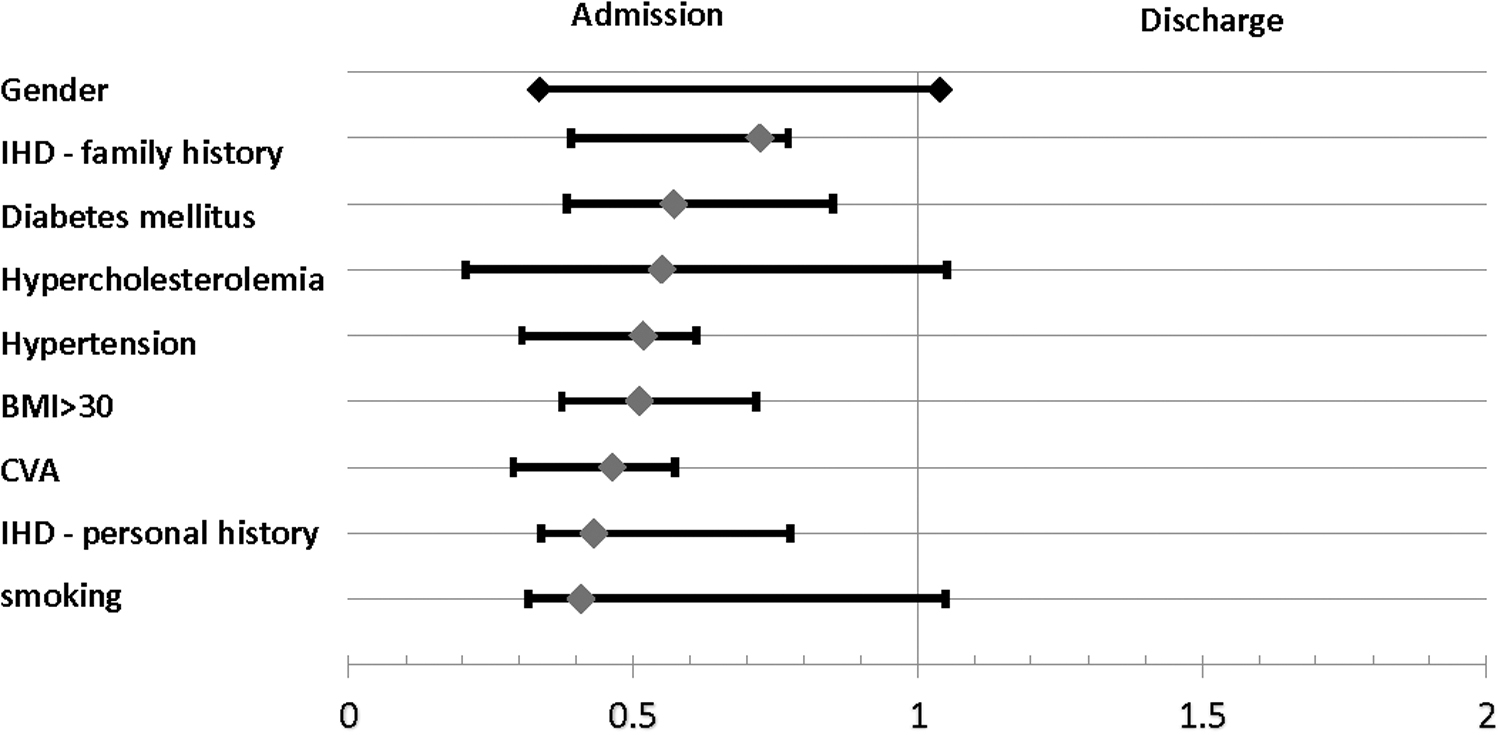
ED visit outcome: odds ratio by cardiovascular risk factors.
Odds Ratios for Discharge Outcome by Cardiovascular Risk Factor
CI, confidence interval; OR, odds ratio.
HEART Pathway-based analysis
According to the HEART Pathway protocol, 227 patients (29.4%) were expected to be admitted and 545 (70.6%) were expected to be discharged. The corresponding real-life decisions by the ED physicians were 278 patients (36%) admitted and 494 (64%) discharged. The real-life admission rate was significantly higher than possible by application of the HEART Pathway protocol (p = 0.001, Fig. 4).
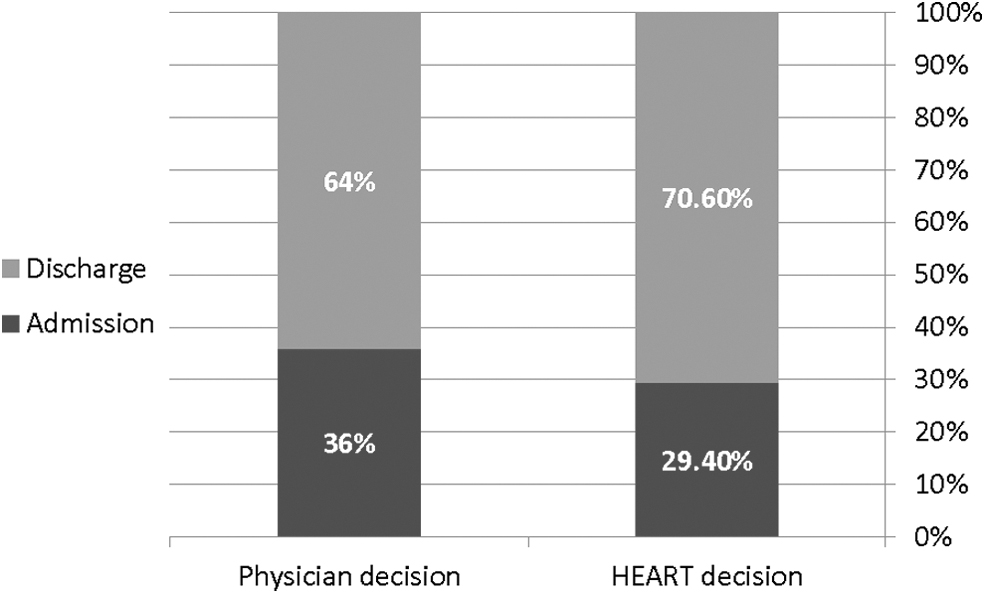
HEART Pathway prediction versus physician decision. Admission rates are significantly higher (P = 0.001) than possible using the HEART Pathway.
The cohort was then divided on the basis of the HEART Pathway recommendation for admission or discharge (Table 3), and a logistic regression model was applied. Male sex was found to be a significant factor favoring admission among the patients who would be expected to be admitted according to the HEART Pathway protocol (P = 0.007, Fig. 5).
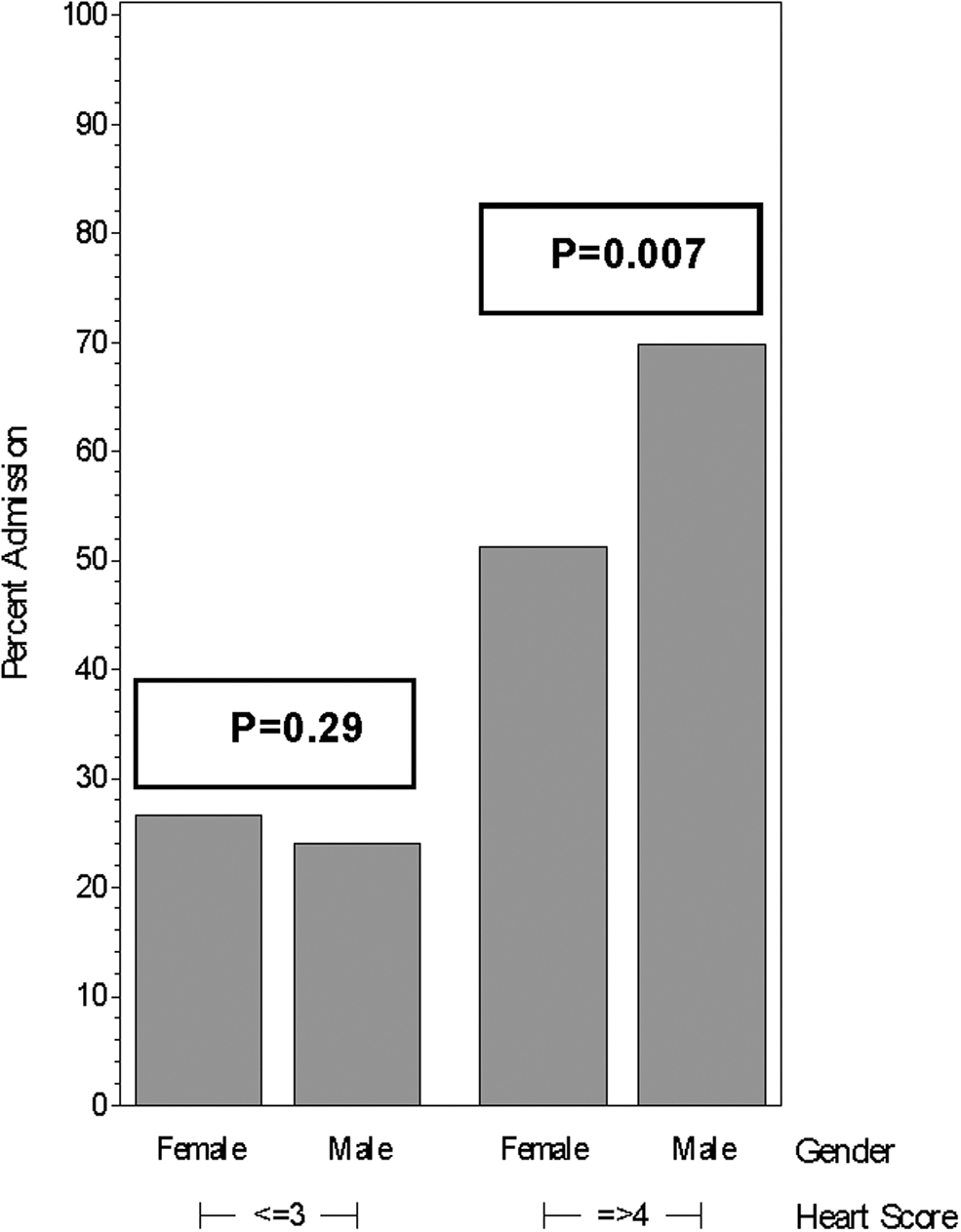
HEART score and admission rate stratified by gender.
Emergency Department Visit Outcome by Decision of the Emergency Department Physician Compared with the HEART Pathway Recommendation
Discussion
This study found that compared with men, there is a bias favoring discharge in women with clinical signs and risk factors suggesting coronary artery disease.
The overall admission and discharge rates were not significantly different in men and women. However, comparison with the expected rates using the HEART Pathway protocol yielded a significantly higher-than-expected proportion of patients admitted by decision of the ED physician. On subgroup analysis, male sex proved to be a significant independent factor favoring admission in the subgroup of patients in whom the HEART Pathway recommended admission.
Our results agree with previous studies reporting a negative bias in identifying myocardial ischemia in females compared with males. Various reasons for this bias have been suggested. 6 –10
Leifheit-Limson et al., 6 as part of the VIRGO program (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients), investigated 3501 patients aged <55 years with acute myocardial infarction for self-perceived risk of heart disease alongside the health care provider's report of cardiovascular risk factors. They found that although both sexes had a high risk-factor burden, fewer women than men perceived themselves as being at risk (52.2% vs. 55.8%, P < 0.05). Moreover, examination of the health care providers' actions revealed that women were less likely to be told they were at risk (45.1% vs. 49.2%, P < 0.05) and less likely to be advised about heart disease and risk modification (45.9% vs. 54.7%, P < 0.001).
In another VIRGO study, Lichtman et al. 8 interviewed 2009 women and 976 men admitted with acute myocardial infarction to investigate presentation patterns and perception of cardiac-related symptoms. They found that chest pain was the predominant presenting complaint in both men and women. However, a greater proportion of men than women sought medical care because of concerns about a heart problem (49.8% vs. 41.6%, p < 0.001). Among those who sought medical care before the myocardial infarction, more women than men reported that their health care provider did not think the symptoms were heart related (53.4% vs. 36.7%, P < 0.001).
Our findings of a higher admission rate in men/higher discharge rate in women within the subgroup of patients expected to be admitted according to the HEART Pathway recommendations is in line with these previous studies and suggests a bias in attributing heart disease symptoms to a noncardiac origin in women. To our knowledge, this is the first study to use the HEART Pathway as a validated risk-stratification tool to evaluate inter-gender bias.
This study was limited by the retrospective design and our reliance on the accuracy and depth of the descriptions in the patients' medical records. The ED physicians may have used terms and descriptions that fit the decision they had already made regarding the patient's risk of having coronary artery disease, thereby creating a bias on analysis of the patient's risk according to the HEART Pathway. The overall study population was relatively large, but for subgroup analysis, a larger number of women and of admitted patients would be beneficial in future studies.
One of the main strengths of the study was our use of the validated HEART Pathway risk-stratification tool. This made it possible to retrospectively calculate the coronary artery disease risk as the reason for the patient complaints in the same manner as a practitioner could have at the time of the ED visit, without being influenced by the actual outcome. As a result, we were able to pinpoint where the practitioners' decision did not meet the HEART Pathway validation. We also applied strict inclusion criteria and excluded patients with vague complaints that were later attributed to coronary artery disease.
Conclusion
Our study reaffirms the negative bias in suspected coronary artery disease as the cause of chest pain in women. As the HEART Pathway is a validated risk-stratification tool, there is a high likelihood that serious coronary artery disease may be overlooked in women despite their seeking timely medical assistance.
Footnotes
Authors' Contributions
Writing and editing of the article by A.G. and S.S., supervisions of the study and editing by M.D., A.G. was responsible for collecting patient's data, and S.S. did statistical interpretations.
Ethics Statement
This study involves human participants and was approved by an Institutional Review Board.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.