
Abstract
Background:
Although men and women who misuse substances have different needs, no rigorous systematic literature review has been conducted examining psychosocial substance use interventions for women across a broad range of types of therapeutic approaches and populations.
Materials and Methods:
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were used to guide this review. English language, peer-reviewed research articles indexed in PubMed, PsycINFO, CINAHL Complete, and Web of Science through May 6, 2021, were searched. Peer-reviewed articles were included in the review if they were written in English; described a randomized controlled trial of a psychosocial intervention to reduce substance misuse and related problems in women; and reported quantitative data on alcohol or illicit drug use as an outcome that was linked to the interventions.
Results:
A total of 51 articles met eligibility criteria, reflecting a broad array of interventions with different levels of methodological rigor. Several, but not most, interventions were tailored to meet the needs of specific subgroups of women, but evidence regarding the efficacy of tailoring was inconclusive. Overall, 61% of studies reported one or more positive substance-related intervention effects, with target substance (alcohol only vs. other drugs only or both alcohol and other drugs) and intervention dosage associated with intervention success.
Conclusions:
Fewer studies targeting alcohol only reported one or more positive intervention outcomes. This warrants further study, given that polysubstance use is the norm, not the exception. Future research might also focus on reducing treatment barriers to women, as this has the potential to improve overall treatment outcomes for this population.
Introduction
Globally, alcohol, tobacco, and other drug use disorders are recognized as a major public health problem with increased morbidity and mortality. 1 In the United States, substance misuse and use disorders are prevalent and contribute to development of physical and mental health problems, accidents, and reduced quality of life. 2
Worldwide, tobacco use is one of the largest preventable causes of premature death, with attributable death rates three times higher for smoking than for alcohol, and more than 15 times higher than for illicit drug use. 3 The World Health Organization (WHO) Report (2019) 4 estimated that globally, 19% of adults were current smokers, with prevalence five times higher in men (33%) compared to women (6%). Tobacco accounts for more than 8 million deaths annually, of which 1.2 million are caused by second-hand smoke exposure. 5 The impact is greater on people in low- and middle-income countries, with an annual cost of over $1.4 trillion to the global economy.
Alcohol also contributes to significant morbidity and mortality. The WHO 6 estimates that worldwide, alcohol alone contributes to more than 200 illnesses and injuries (e.g., violence, accidents, and suicides), and is responsible for 3 million deaths annually, making it the ninth leading global risk factor for morbidity and premature death. 7 In the United States, while the 12-month prevalence of harmful alcohol use and dependence in persons 15 years of age and older is higher for males (17.6%) than females (10.4%), alcohol use disorder (AUD)-related risks to maternal and child health (e.g., fetal alcohol effects and alcohol-related violence) are of particular concern and were identified as a global priority by the WHO. 6
Latest data from the World Drug Report 2021 indicate that in 2019, it was estimated that more than 275 million people between the ages of 15 and 64 reported past year psychoactive substance use. 8 Of these, 36 million met criteria for a drug use disorder, with 11 million endorsing intravenous drug use. Substance use disorders (SUDs) contribute to increased morbidity and mortality, in part, because of concomitant medical (e.g., HIV and Hepatitis B and C) and psychiatric (e.g., depression and post-traumatic stress disorder [PTSD]) disorders and psychosocial problems (e.g., trauma, homelessness, and incarceration). 1,9
As cogently noted in the World Drug Report 2021, treatment for drug use often is not tailored to the specific needs of women, who face significant stigma and marginalization as a result of their use. 8,10,11
While rates of alcohol and other drug use are lower in women than in men, females progress more rapidly than males from substance use to dependence to first treatment episode. 8,12,13 Furthermore, women who use alcohol or other drugs, relative to men, are at greater risk for developing medical and psychological problems. 14 Because women progress more rapidly than men from alcohol and other drug use to dependence, early screening and intervention are critical to prevent the development of SUDs. In addition, early screening and intervention can prevent adverse fetal consequences arising from unintended pregnancies, 15 and victimization that occurs at a higher rate among women, versus men, who use alcohol or other drugs. 16
Despite male-female differences in the initiation and progression of substance use to problems and dependence, decades of research comparing SUD treatment outcomes for programs serving both males and females have yielded mixed results. 13 A review by Greenfield et al. 12 found that, while SUD treatment retention generally did not differ for men and women, women were less likely than men to seek SUD treatment. 17,18
One of the reasons for disparity between men and women is the differential rate of psychiatric co-morbidities. Women are two to three times more likely to have a co-morbid psychiatric diagnosis (depression, anxiety, and post-traumatic stress), which is recognized as a barrier to both engagement and retention in SUD treatment. 19,20 Practical barriers such as lack of transportation, housing, and childcare, 21 –25 as well as involvement in violent relationships and greater social stigma 14,26 also can hinder a woman's ability to initiate SUD treatment.
Factors that have impeded women's engagement and retention in SUD treatment have led to the development of women-centered drug treatment services. Terplan et al., 27 in a study of the availability of women-centered drug treatment services in the USA, describe programs designed to address practical barriers to care for women and tailored to meet the needs of women. While they indicate such programs have lower rates of treatment dropout and less drug use, 28 in the absence of randomized controlled trials (RCTs), interpretation of such data is limited.
Despite the fact that scholars have suggested that substance use interventions should be adapted specifically to the needs of women, 29,30 which could involve tailored content or women-only treatment delivery, the overall body of SUD intervention research continues to report on programs that are not specific to women. This is problematic because the efficacy of intervention content that is not tailored to women or intervention delivery that includes a predominantly male or mixed male and female sample may be very different from the efficacy of intervention approaches that take the unique needs of women into account.
Of course, the efficacy of female-specific interventions may not differ from interventions that are not specific to women. 19 However, unless tailored intervention content is compared with nontailored content, or researchers report the effectiveness of interventions separately for men and women, scholars are unable to access this information.
Although there have been recent reviews of interventions for very specific populations of women (e.g., women who are pregnant 31 and women who are incarcerated 32,33 ), no rigorous systematic literature review has been conducted to date examining substance use interventions for women that are psychosocial in nature across a broad range of types of therapeutic approaches and populations. Because the literature tends to be fragmented, the lack of such a comprehensive review and synthesis makes it difficult to identify gaps in research. The purpose of this systematic review, therefore, was to summarize original, quantitative reports of RCTs evaluating the efficacy of psychosocial interventions targeting alcohol and/or drug misuse and use disorders in women.
Materials and Methods
Sources
To ensure transparent reporting, this systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines, 34 which include a 27-item checklist and a 4-phase flow diagram illustrating identified, screened, eligible, and included studies. A literature review was conducted using the following electronic databases: PubMed, PsycINFO, CINAHL Complete, and Web of Science. Searches were conducted between February 28, 2017, and March 17, 2017, and then updated on May 6, 2021. In each database, a combination of keywords joined using Boolean operators was used to represent the concepts of substance use, psychosocial interventions, and females/women.
Substance use was described using a combination of broad and specific terminology, including substance use, drug use, alcohol use, illicit drugs, substance abuse, substance use disorders, opiates, hashish, heroin, cocaine, crack cocaine, marijuana, morphine dependence, and amphetamines. Psychosocial intervention terminology included broad terms for interventions as well as for specific psychological, social, and educational interventions, as well as terminology related to recovery and harm reduction strategies. A validated search filter was used to limit results to RCT. 35 Please see Supplementary Appendix SA1 for a list of the specific search terms used. To ensure that our search was as comprehensive as possible, databases also were searched for key authors' names and frequently employed interventions (e.g., Seeking Safety).
Eligibility criteria
Articles were included in the review if they met the following inclusion criteria: (1) described an RCT that employed a psychosocial intervention designed to reduce or eliminate substance misuse and/or associated harms, (2) reported quantitative data on alcohol or illicit drug use as a primary or secondary outcome that was linked to the intervention, (3) was published in a peer-reviewed journal with a full-text copy of the article available, (4) was written in English, and (5) included only women in the randomized conditions in the study design. Thus, studies that compared women receiving couple-focused treatment or a combination of couple-focused and individually focused treatment as one or more of the intervention arms were included if men in these studies were not part of the randomization process, and data on women were the focus of the report.
All studies that were not RCTs were excluded, including studies that described an intervention or the study design, but did not report outcome data, or only reported qualitative findings. RCTs were excluded if the randomization was something other than the psychosocial intervention component (e.g., living location 36 ). RCTs that focused solely on tobacco use were excluded. RCTs that focused solely on prevention of substance use among adolescents or young adults, and had no risky substance use criteria for inclusion in the intervention also were excluded.
We did not restrict the types of psychosocial interventions included in the review, and included interventions that targeted physical and mental health outcomes, or aimed to improve or modify behavior if they also reported alcohol or drug use outcomes linked to the intervention. Because there have been several recent reviews with very specialized populations, 31 –33 we excluded studies if they focused on women who were incarcerated or pregnant.
Study selection
To select studies, the article titles and abstracts were screened for eligibility by two independent researchers, at least one of whom was one of the study authors. The vast majority of articles screened out during this process did not meet the sampling criteria (e.g., the randomized sample was not 100% female). Other common reasons for exclusion during this phase included presentation of study protocols only and non-RCT studies. Following this process, the unique articles that remained were full text reviewed for inclusion/exclusion criteria by at least two of the study authors. Additional articles were screened out during this process, leaving a final sample for analysis. Figure 1 describes the study selection process and the results from each stage of review.
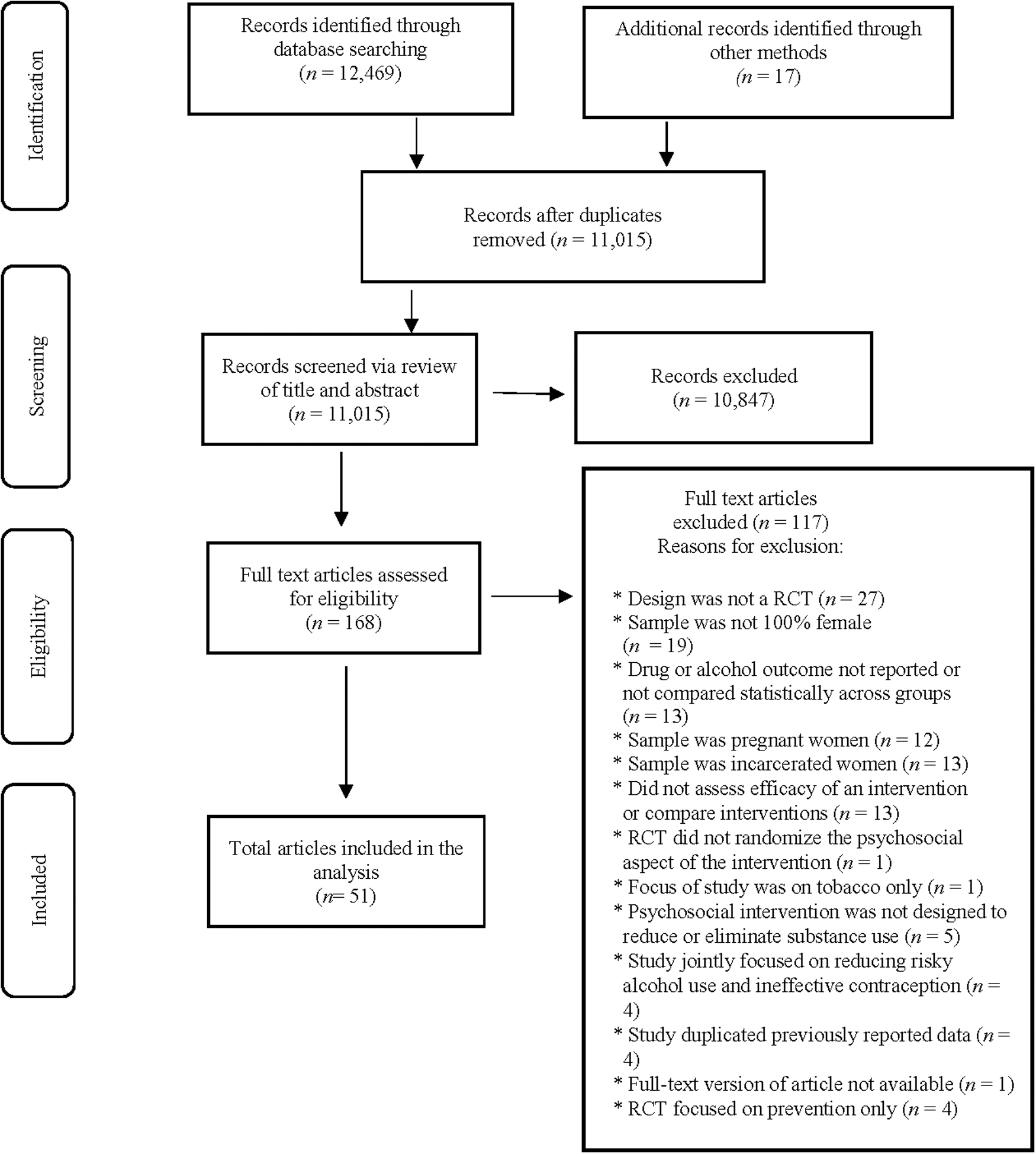
PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data abstraction, assessment of risk of bias, and analysis
Data were abstracted from the selected articles by two of the study authors using a standardized form that captured information on study design, population, the nature of the intervention, measures utilized to assess alcohol or drug use, and findings. Abstracted data were compiled, reviewed, and summarized in table form by study authors.
Consistent with recommendations by Cochrane, 37 risk of bias assessments, but not assessments of study quality, were conducted to examine limitations in design and implementation using the Cochrane Collaboration Risk of Bias Tool. 37 Assessments were made in the areas of sequence generation (Was the allocation sequence adequately generated?), allocation concealment (Was allocation adequately concealed?), blinding of participants, personnel, and outcome assessors (Was knowledge of the allocated intervention adequately prevented during the study?), incomplete outcome data (Was incomplete outcome data adequately addressed?), and selective outcome reporting (Are reports of the study free of suggestion of selective outcome reporting?).
Judgments of “Yes (low risk of bias),” “Unclear,” and “No (high risk of bias)” were applied to each question and then summarized across studies. These assessments were independently conducted for each article by at least one of the study authors; 20% of the articles were assessed by two of the study authors to assess inter-rater reliability, which was >90%.
Results
As seen in Figure 1, the search strategies yielded 12,486 articles for review. After eliminating duplicates, 11,015 studies remained. After reviewing the titles and abstracts, 168 articles were full text reviewed for inclusion/exclusion criteria, and 117 additional articles were eliminated, leaving a final sample of 51 articles.
All articles included in the final review are summarized in Table 1. As seen in the table, a range of samples and types of interventions was utilized across the 51 studies. It should be noted that studies were not classified by intervention type or intensity. This was because some of the interventions contained novel elements, making it difficult to categorize them accurately. Other interventions combined features from multiple evidence-based treatments (e.g., motivational interviewing [MI] plus cognitive behavioral therapy [CBT]) adding to the dilemma.
Summary of Articles Included in the Review
All study participants identified as female. All studies included in the review were either 2-arm or 3-arm RCTs. If session length was not noted, it was not reported. The term “alcohol dependence” appears if study authors used DSM-IV criteria to screen or diagnose participants.
In the column, “Significant Effect(s)” indicates that at least one substance use effect hypothesized by the study authors was significant. Generally, this involved improvement in the intervention condition relative to the comparison or control condition.
The term “Pure comparison” was used when the authors of a study specified no difference between treatment conditions. This typically occurred when a standard treatment was compared to a variation (e.g., ABCT vs. ABIT) (Sobell et al., 2009). 100
AA, African American; ABCT, alcohol behavior couples' therapy; ABIT, alcohol behavior individual therapy; AUD, alcohol use disorder; BCT, behavioral couples therapy; CBT, cognitive behavioral therapy; CM, contingency management; CPT, cognitive processing therapy; DBT-CM, dialectical behavioral therapy case management; EBFT, ecologically based family therapy; EMP, Engaging Moms Program; ER, emergency room; FS-CBT, female-specific cognitive behavioral therapy; GDC, group drug counseling; G-FS-CBT, group-based female-specific cognitive behavioral therapy; HG, health group; HP, health promotion; IBT, individually based therapy; ICM, intensive case management; ICMS, Intensive Case Management Services; I-FS-CBT, individual female-specific cognitive behavioral therapy; MABT, mindful awareness in body-oriented therapy; MDPO, mean number of drinks per occasion; MI, motivational interviewing; MIO, mothering from the inside out; MM, mindfulness meditation; MTP, Mothers and Toddlers Program; NIDA, National Institute on Drug Abuse; PBSs, protective behavioral strategies; PCP, primary care provider; PE, parent education; PIRI, pleasant imagery and relaxation instruction; PPRS, prevention of postrape stress; PTSD, post-traumatic stress disorder; RBT+WC, Reinforcement-Based Treatment and the Women's CoOp; RCT, randomized controlled trial; RD, risky drinking session; RMCs, recovery management check-ups; RPMG, relational psychotherapy; RPT, relapse prevention training; SA, sexual assault; SAMFE, Sexual Assault Medical Forensic Examiner; SB, spring break; SET, structural ecosystems therapy; SN, social network; SUD, substance use disorder; TANF, temporary assistance for needy families; TAU, treatment as usual; TIARAS, Trauma Intervention for Affect Regulation, AIDS, and Stimulants; TSF, 12-step facilitation; WHC, Women's Health CoOp; WHE, Women's Health Education; WIC, Women Infant and Children; WPR, Woman's Path to Recovery; WRG, Women's Recovery Group.
Instead, we grouped the studies on the basis of two factors. The first was substance use severity for the target population in each clinical trial. Studies were categorized as having participants with either high- (N = 28), moderate- (N = 17), or low- (N = 6) severity substance use. Studies assigned to the high-severity group only enrolled women who met diagnostic criteria for one or more SUDs. In contrast, the moderate-severity group studies recruited women with heavy or at-risk alcohol use or heavier drug use, as well as comorbid mental health or psychosocial challenges. While some women in the moderate severity group would likely meet the criteria for SUD, no diagnosis was required for study enrollment. Finally, low-severity studies were those with no inclusion criteria for heavy or problem substance use. As a result, these studies enrolled women both with and without heavy or problem substance use.
Second, within each severity group, studies were classified based on the type(s) of substance(s) that were the focus of each RCT. Specifically, studies were labeled as targeting: alcohol use and problems only (alcohol only; N = 15); other drugs, but not alcohol (drugs only; N = 14); and both alcohol and other drugs (alcohol and drugs; N = 22). This nomenclature acknowledged the historical separation in the United States of treatment services for AUD from services for other drug use disorders. It also recognized that alcohol treatment research has been funded by a different National Institutes of Health (NIH) Institute (National Institute on Alcohol Abuse and Alcoholism [NIAAA]) than drug treatment research (National Institute on Drug Abuse [NIDA]), and that each institute has guided research based on its own funding priorities.
In addition, there is research to support use of this classification method, with both epidemiological 38 and clinical 39 studies finding differences in treatment outcomes for patients with alcohol only, drug only, and both alcohol and drug problems. Taken together, this classification system allowed us to characterize the type and intensity of the interventions both within and across participant substance use and problem severity subgroups.
Risk of bias ratings
Risk of bias ratings varied across the 51 studies reviewed, with most studies revealing no apparent risk of bias in selective reporting, very little risk of bias in incomplete outcome data, and unclear risk of bias in blinding of outcome assessment, allocation concealment, and random sequence generation. The greatest risk of bias observed in these studies was failure to blind outcome assessments: nearly one-fifth of the studies (24%) demonstrated high risk of bias in this category, with another 45% failing to provide enough information to provide a judgment about this risk. Some risks of bias are to be expected, given the psychosocial nature of the interventions. The majority of studies reported low risk of selection bias through random sequence generation (71%), but a sizable percentage (29%) did not report sufficient detail to make a judgment in this category or regarding allocation concealment (65%). Please see Figure 2 for complete risk of bias information.
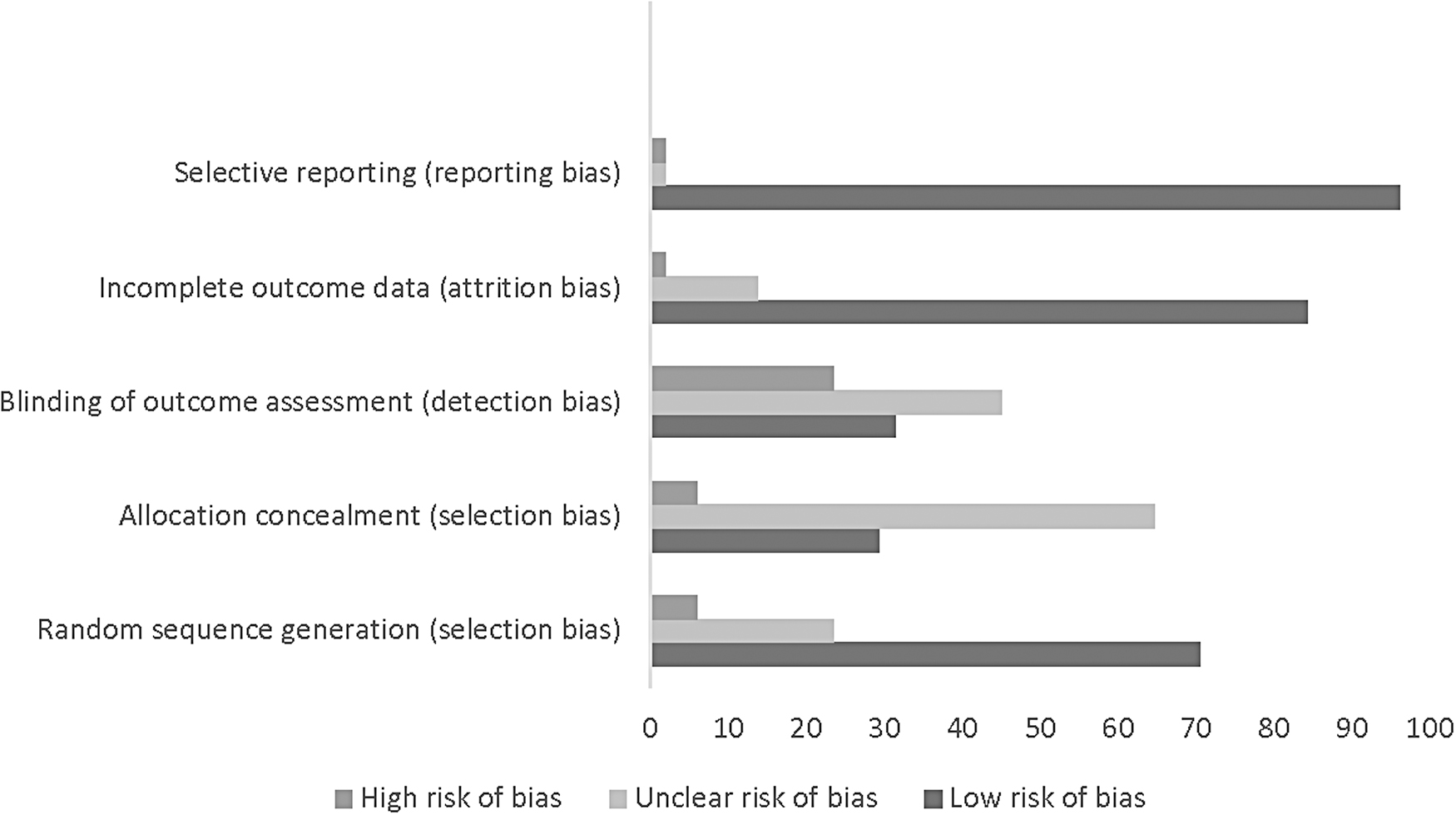
Risk of bias graph.
Studies targeting low-severity samples
Six of the 51 studies targeted low-severity participant samples; 4 of the 6 (67%) studies reported one or more positive substance-related intervention effects (Table 2).
Percentage of Studies with At Least One Positive Intervention Effect by Severity Status of the Sample and Substance Targeted
N = 51.
Alcohol-only studies
Two of the six low-severity studies focused on alcohol only, 40,41 but only Dvorak et al. 41 reported intervention effects on at least one outcome. Both studies used a single session, web-based intervention, but they differed substantively in sample size, target population, outcome measures, and follow-up period. Dvorak et al. 41 focused on reducing drinking among women who indicated they intended to party during spring break (SB) and found reductions in alcohol-related problems during the SB period. In contrast, Delrahim-Howlett et al. 40 recruited women with children from WIC (Women Infant and Children) clinics who reported drinking at moderate levels and followed them for 2 months postintervention. Neither RCT reported changes in alcohol consumed, and Delrahim-Howlett et al. 40 reported no change in any alcohol-related outcome.
Drugs-only studies
Two low-severity studies targeted drugs other than alcohol. Both focused on marijuana use, and both reported one or more intervention effects. 42,43 While the two studies differed dramatically in sample size (N = 34 and 332), both evaluated two-session interventions and followed participants for at least 3 months postintervention.
Alcohol and drug studies
Two low-severity studies targeted both alcohol and other drugs, with one reporting positive outcomes on at least one measure 44 and the other finding no substance-related intervention effects. 45 Both studies evaluated a single-session intervention and both focused on early intervention and prevention of a progression in alcohol or drug use among adolescents. Mason et al. 44 used MI and social networking and delivered their intervention in a primary care setting. They measured substance use and negative consequences of use and reported a significant intervention effect on trouble due to alcohol use before sex. In contrast, participants in Walsh et al.'s 45 study were recent victims of sexual assault, who may or may not have had a history of risky drinking or drug use. Participants received a 9-minute intervention (watching a video) and no significant intervention effect was reported.
Studies targeting moderate-severity samples
Seventeen of the 51 studies in this review targeted moderate-severity samples; 9 of these, studies (53%) reported one or more positive substance-related intervention outcomes.
Alcohol-only studies
Eight of the 17 studies in this category targeted heavy/problem drinking. Three reported positive findings, 46 –48 and five indicated no significant intervention result. 49 –53 When studies with positive outcomes were compared to those with no significant alcohol-related intervention effects, one notable difference centered on baseline levels of alcohol use. For the three studies with intervention effects, 46 –48 women were enrolled, who reported recent (past month) heavy drinking, which provided an opportunity to observe group differences in change from baseline to follow-up assessment. For example, 92% of participants in Manwell et al.'s 48 study reported recent binge drinking, with an average of 5+ episodes in the past month.
In contrast, inclusion criteria for the five studies with no group differences tended to survey participants about more distal (past year) drinking 51 or used screening tools such as the AUDIT that combined quantity and frequency measures with adverse consequences. 50 Still others 49 lacked detail such that baseline drinking patterns could not be determined. The importance of this methodological issue was illustrated in the Connors and Walitzer report. 52 While testing of primary hypotheses yielded no intervention effect, a post hoc analysis focused solely on the heavier drinking women at baseline did in fact find a differential effect by intervention group.
Drugs-only studies
Of the four studies in this category, two 54,55 reported significant differences in drug use-related outcomes, while two 56,57 found no significant intervention effect. All four interventions in this group were relatively brief, ranging from a minimum of one 32 to a maximum of four sessions. 33,34 Two of the four studies contained MI elements; intervention components of the other two studies included expressive writing and women-focused HIV prevention. Studies with positive outcomes differed from those with nonsignificant findings in several ways. First, the two studies with positive outcomes had much larger sample sizes than the two studies with nonsignificant findings. Second, both studies with positive outcomes recruited women who were not engaged in other substance-related treatment. 54,55 The two studies with negative outcomes examined brief interventions delivered as adjuncts to ongoing treatment for substance use and targeted women with stimulant 56 or primarily cocaine 57 use.
Alcohol and drug studies
Four of five moderate-severity studies targeting both alcohol and other drugs reported one or more positive substance-related outcomes. 58 –61 The four articles with positive findings described interventions that varied by type and amount, ranging from two 2-hour Women's Health Co-op sessions 61 to 12 sessions of dialectical behavior therapy (DBT) and case management 58 to 13 sessions of a culturally adapted cognitive processing therapy 59 to 14 check-up interviews over a 3-year time period. 60 Sample sizes ranged from a low of N = 7359 to a high of N = 480. 60 In addition, sample recruitment and target groups also varied widely from Native American women with heavy drinking or illegal drug use and symptoms of PTSD 59 to women recently released from jail and referred to community treatment 60 to homeless women on probation or parole with past history of alcohol or drug use 58 to women living with HIV and reporting recent alcohol and drug use. 61
In contrast, the one study with negative results 62 was conducted in the Republic of Georgia and recruited women with a recent (past 30 day) history of injecting illicit drugs and heterosexual activity. While the majority of women in that study reported recent IV opioid use, in the absence of formal SUD diagnoses, the study was classified as moderate severity. Furthermore, substance use outcomes were limited to urine drug assays and breathalyzers for alcohol use, and the study occurred during what appeared to be a significant shift in policy concerning methadone and buprenorphine and the treatment of opioid use disorder (OUD).
Studies targeting high-severity samples
Twenty-eight of the 51 studies in this review targeted high-severity samples; 18 studies (64%) reported significant intervention effects on at least one substance-related outcome.
In these studies, all but one of the alcohol-only studies enrolled women with a diagnosis of AUD (past year) and self-report of recent use, typically defined as the past 60 days. For the drugs-only studies, all but one of the studies recruited from SUD treatment programs. These ranged from inpatient medical detoxification to residential to outpatient counseling or medication-assisted treatment programs. For those studies targeting both alcohol and drugs, half recruited from SUD treatment programs, with other studies focused on homeless women, women in family drug court, and women enrolled in a TANF (temporary assistance for needy families) welfare to work program, among others.
Alcohol-only studies
For the five studies targeting women with AUDs, two reported intervention effects on all alcohol-related outcomes, 63,64 while three reported no intervention effect on any alcohol-related outcome in the study. 65 –67
Polcin et al. 64 tested the effects of a nine-session intensive MI (IMI) intervention versus a single session of MI plus eight sessions of nutrition education on alcohol problem severity, percentage of drinking days, and percentage of heavy drinking days. At 2 months postintervention, the IMI intervention was superior to the control group on all outcome measures. The second study with positive intervention effects tested a variation of CBT, and compared women randomized to a 20-session alcohol behavioral couple therapy (ABCT) with women assigned to a 20-session alcohol behavioral individual therapy (ABIT). 63 McCrady et al. 63 found improvements in days abstinent and fewer days of heavy drinking among women randomized to ABCT versus ABIT.
Interestingly, McCrady et al. 63 and the three articles with no significant intervention effects were from the same research group. 65 –67 All four tested variations of CBT, comparing modes of delivery (individual or group format) and different target groups (couples, individuals, or a blend) with similar procedures and follow-up periods. McCrady et al. 67 had a smaller sample size than McCrady et al. 63 and found no difference in alcohol-related outcomes for women randomized to 12 sessions of ABCT compared to those receiving a combination of 5 individual CBT sessions and 7 ABCT sessions. Similarly, while women in both treatment conditions significantly reduced their percent drinking days and percent heavy drinking days by equivalent amounts, no difference was found when group-based female-specific CBT was compared to individually based female-specific CBT, 65 and no difference was found between CBT that was female specific versus neutral. 66
Drugs-only studies
Six of the eight studies in this category reported significant intervention effects on at least one outcome. 68 –72 All these studies focused on women with one or more drug use disorders, and in some cases, a comorbid diagnosis.
Among the six studies with at least one positive drug-related finding, the types of interventions tested varied widely, ranging from DBT 69 to faith-based community support 72 to relational psychotherapy. 70,71 Interestingly, all but one examined an intervention delivered in conjunction with treatment as usual (TAU). Four of the six studies with positive outcomes enrolled women with OUD; three recruited from medication-assisted treatment programs, and those participants received medication for Opioid Use Disorder (MOUD) 70,71,73 ; the fourth study 69 ; provided an opioid medication (no longer available) to all participants. The remaining two studies with positive outcomes either tested an intervention delivered to women in the context of longer term residential care (3–6 months) 72 ; or examined a nurse-delivered intervention for nontreatment-seeking women with SUD seen in a hospital Emergency Room. 68
The two studies with negative substance-related outcomes also tested interventions delivered as adjuncts to treatment, but one examined a lower intensity (two sessions) intervention and paired it with a shorter duration inpatient program (7 days–4 weeks), 74 and the other intervention was offered in tandem with a more heterogeneous network of outpatient SUD treatment options that included (but did not require) MOUD. 75 The Wechsberg et al.'s study 74 was conducted in Russia and targeted women with injection drug use, with many likely to have an OUD diagnosis in the absence of MOUD treatment.
Alcohol and drug studies
Ten of the 15 studies in this category reported significant intervention effects on at least one outcome. 76 –85 The interventions tested in this group of studies varied widely. While by definition all women met diagnostic criteria for one or more SUDs, many presented with comorbid conditions that put them at risk for continued alcohol and other drug use and problems. Such comorbidities included the following: a diagnosis of trauma exposure, HIV+ status, and homelessness, among others. As with the studies of high-severity samples that targeted drugs, many of the treatment periods were lengthy, ranging from 6 weeks to 15 months. Interestingly, none of the 15 studies enrolled women receiving MOUD.
Study outcomes were diverse, and included assessment of abstinence only, frequency of drug and alcohol use, and severity of use, or combinations of the above. Fourteen studies verified drug use with urinalysis. The time frames of substance use outcomes varied from the past week 86 to the past month 77 –80,87 –89 to the past 90 days. 76,81 –85,90
In the 10 studies with positive substance-related intervention effects, 3 described RCT inclusion criteria that may have restricted enrollment to women with some family and social support resources. Feaster et al. 77 only enrolled women who could identify a family member willing to participate in the required companion program. Similarly, a male partner willing to participate in Behavioral Couples Therapy was a requirement for both the O'Farrell et al. 81 and Schumm et al. 84 clinical trials. Another three of the 10 studies with positive intervention outcomes focused on women with additional incentives to participate in an intervention, including Dakof et al. 76 who recruited from family drug court and Morgenstern et al. 79,80 who enrolled women from welfare to work programs. The remaining three studies recruited from community outpatient SUD programs.
Two studies by Price et al. 82,83 tested mindful awareness in body-oriented therapy as an add-on to outpatient SUD treatment (TAU). Zhang et al. 85 tested ecologically based family therapy delivered either at home or in the office to a health education control group in a sample of women who had a child between the ages of 8 and 16 years living with them.
The last study with positive findings was one of two that compared a woman-only recovery group in combination with structured relapse prevention group therapy to a drug counseling group that included both men and women. While one study found at least one positive outcome (Greenfield et al. 78 ), the other reported no significant group difference for any substance-related outcome (Greenfield et al. 87 ). The first study 78 had a smaller sample (N = 23) than the second 87 (N = 100), and only the latter enrolled some women who were also receiving MOUD. Of the remaining four studies with negative findings, two were clinical trials of Seeking Safety and targeted women with SUD and either subthreshold or full PTSD (Hien et al. 86 and Schäfer et al. 89 ).
Another by Slesnick and Erdem 90 tested an ecologically based treatment in a sample of homeless women, and Najavits et al. 88 found no difference in outcomes for a woman-focused versus nonwoman-focused intervention in a sample of female military veterans with SUD.
Discussion
This article describes outcomes of 51 randomized clinical trials of psychosocial interventions targeting alcohol and/or drug misuse and use disorders in women. During our initial review of these studies, we found significant heterogeneity in the types of interventions examined, the substance(s) they centered on, and the baseline levels of use, misuse, and related problems needed to qualify for study enrollment. Because our primary focus was on the psychosocial interventions themselves, we sought to reduce some of this variability by first categorizing the studies into low-, moderate-, and high-severity groups based on participant substance use severity. Within each severity group, we further classified studies by substance(s) targeted in the intervention, namely alcohol only, other drugs (excluding alcohol), or alcohol and other drugs.
Participant severity risk groups
The proportion of studies reporting one or more positive outcomes ranged from 53% for moderate-severity studies to 67% for low-severity studies, with 64% of high-severity studies reporting one or more positive outcomes. As would be expected, brief, single-session interventions were more typical in the low-severity group of studies, while higher intensity and longer duration interventions predominated in the high-severity group. In fact, all the interventions with the low-severity samples used one or two sessions. Interestingly, the success rate in these low-severity studies was comparable to that found for high-severity samples.
In contrast to the stand-along interventions delivered in the low-severity studies, many of the interventions in this high-severity group of studies were delivered in conjunction with other ongoing services ranging from medication for Opioid Use Disorder (MOUD) and contingency management to housing and employment assistance. Notably, all the studies with high-risk samples in which women received MOUD did not target alcohol; all but one of these studies reported a positive intervention effect on one or more drug-related outcomes. In addition to all participants meeting criteria for SUDs, participants presented with comorbid conditions that included physical and/or mental health disorders and psychosocial challenges. Not surprisingly, the interventions in this group of studies were heterogenous, but notably, most reported intervention efficacy on at least one substance-related outcome. Participants in these studies were diverse in terms of race/ethnicity, rural-urban living location, and educational attainment.
The moderate-severity studies were the most variable in a number of ways. In terms of sample characteristics, participants varied on their baseline levels of substance use, their recency of problematic use, their use of illicit substances, and the presence of comorbid conditions. In addition, while a subgroup of participants might have had a diagnosis of SUD, this was not an inclusion criterion for participation, and therefore did not meet our criteria for a high-severity study. Overall, the wide range of participants in this group of studies may have accounted for the lower success rate relative to studies targeting low- and high-severity samples.
Target substance(s)
Classifying studies based on the substance(s) targeted revealed distinct differences in the pattern in outcomes. Fewer than half of the studies in the alcohol-only group reported one or more positive outcomes (40%) compared to three-fourths of the studies in the other drugs-only group (71%) and two-thirds of the studies (68%) in the alcohol and other drug use group. A variety of factors may have contributed to this difference in the alcohol-only group and warrant further study. First, a greater percentage of studies in the alcohol-only group compared intervention modalities (e.g., group vs. individually focused CBT) than either the drugs-only or both alcohol and drugs groups.
In addition, different interventions were tested across the three targeted substance groups, and there was a greater reliance on self-report versus objective biological measures for outcome assessment in the alcohol-only group (although this is changing with real-time ability to collect breathalyzer data through cell phones and PeTH). 92 From a research perspective, alcohol-related treatment research is funded by a separate agency (NIAAA vs. NIDA) and it is not illegal for adults to consume alcohol in moderation. Across severity groups, studies that focused on drugs other than alcohol or both alcohol and other drugs tended to show that intervention success, defined as at least one positive intervention outcome, increased with dosage. This was true regardless of the nature of the intervention.
However, direct comparisons by intervention dose should be avoided, given the myriad methodological issues likely to impact substance-related outcomes such as sample size, types of control or comparison group(s), outcome variables assessed, and follow-up assessment points. For example, McCaul et al. 93 found that patient demographics predicted outpatient SUD treatment better than substance type (alcohol only, drugs only, or both).
Methodological limitations of studies included in the review
Although all the studies included in this review were RCTs, they varied in quality. For example, 20% of the studies had no follow-up after the end of treatment, and an additional 24% of studies followed participants less than 6 months after the end of treatment. Other common concerns included vague descriptions of the intervention content and low intervention dosage. Some low-dosage studies were pilot investigations and were meant to be brief, but other studies reported low dosage for moderate- and high-severity samples, many of whom had comorbid conditions. While many studies analyzed data using an intent-to-treat approach, other studies used listwise deletion in their analyses. This may have skewed results in a positive direction.
Methodological limitations of our review strategy
Although our search strategy yielded over 11,000 unique studies to review, resulting in 51 studies that met all criteria, several limitations of our approach should be noted. First, although we took care to specify appropriate terms in our search, some relevant studies may have been missed due to terminology. For example, our study was not focused on co-occurring disorders per se, so this was not one of our search terms. Second, we did not include RCTs specific to women who were pregnant or who were serving time in jail or prison. We made this decision due to recent reviews targeting these populations and based on our observations that many interventions for women who are pregnant are pharmacological, and many interventions for women who are incarcerated use quasi-experimental designs due to the limitations of the setting.
However, by excluding RCTs for these populations we may have missed unique insights into treatment for women. Interestingly, several studies included in our review focused on women who were at risk for pregnancy or were postpartum; likewise, there were several studies in our review that focused on women after their release from jail or prison. A third limitation of our review strategy was that we did not specifically compare intervention effects for men versus women. A fourth limitation was our decision to classify studies as having at least one substance-related intervention effect that was hypothesized, but not calculating a percentage of positive results for each study. We classified studies as having at least one, versus no, intervention effect, for simplicity, but this decision could have inflated the assessment of intervention effectiveness.
Finally, we included psychosocial intervention studies with substance use as either a primary or secondary outcome. This meant that a study focused on HIV risk behavior, which also assessed substance use, for example, was evaluated using the same criteria as a study whose primary aim was to reduce substance use. While we have no evidence to suggest any difference in substance use outcomes using this differentiation, it may have been useful to systematically differentiate these foci in our results.
Implications for future research
Our review suggested that future RCTs focused on evaluating psychosocial interventions to reduce substance use (SU) and SUDs in women might be improved in several ways. First, additional research is needed to determine whether content tailored to women or delivered to women only is more efficacious than generic content or other delivery modes. These were some of the questions that we wanted to answer in this review, and also were raised by McCrady et al. 94 in a recent review of treatment for women with AUD. We were unable to conclusively answer these questions, as few studies included in our review compared tailored and generic intervention content, or delivery to women only versus other designs.
However, more impactful research efforts might focus on reducing the structural barriers to treatment, a topic our review did not address, but has been noted as a significant issue for women. 8,19 –25 Exposure to trauma, psychiatric comorbidities, and family responsibilities, including child care, are examples of barriers that impede women from seeking or remaining in treatment.
Second, RCTs might focus on polysubstance use rather than single substances, as use of multiple substances is more normative than use of one. 95 None of the studies with high-severity samples that included women receiving MOUD, for example, assessed alcohol use. Although women may respond differently to RCTs based on the substances they predominantly misuse, it is important to characterize the full scope of women's SU at baseline and follow-up. Variability of baseline SU, particularly in low-severity samples, likely contributed to the variability in intervention efficacy.
Third, the dosage delivered in RCTs should match the risk level of samples recruited. Many women present with comorbid mental health conditions or psychosocial impairment, necessitating a coordinated care approach to SU reduction. Several studies with moderate- and high-severity samples in our review, for example, included women with comorbid mental health conditions, but delivered a low intervention dosage.
Fourth, future research should assess interventions implemented with sexual minority women, who have higher trauma and stress exposure than other populations. 96 Fifth, based on several of the studies with low-severity samples included in this review, additional RCTs that utilize MI to reduce marijuana use may be promising. Cannabis use disorders are on the rise 8 ; thus, the potential impact of such RCTs could be quite high. Finally, assets that women have should be evaluated, as these promotive or protective factors may play a critical role in treatment efficacy. Attending to these recommendations will improve our understanding of women's responses to SU treatment.
Implications for clinical practice
Our review suggested that a range of psychosocial interventions across groups of women with different SU and risk levels is effective. This is good news. Thus, having multiple evidence-based approaches on which to draw is important versus relying on a single therapeutic approach. Selection of a specific intervention can be guided by practical issues. Individual-, group-, or web-based approaches can be effective, depending on the individual's circumstances.
Our review of studies targeting low-severity samples in particular revealed the importance of screening for problematic SU patterns to prevent progression to misuse or dependence. Screening for problematic SU patterns is less common for women than men. 97 For moderate- and high-severity populations of women, initial evaluation with standardized assessment should include items that capture the unique needs of women as well as recent and lifetime patterns of use. Although tailoring interventions may not affect treatment outcomes, a recent review by Milward et al. 91 suggests that tailoring is an effective strategy for promoting engagement in substance use interventions, and thus a tool that clinicians might use.
Conclusion
We began this review intending to evaluate the efficacy of psychosocial interventions targeting alcohol and/or drug misuse and use disorders in women, given that men and women who misuse or who are dependent on substances have different needs. Previous research has tended to summarize interventions targeting specific populations or specific intervention approaches. By choosing to cast a wider net, we discovered substantial diversity in these RCTs targeting women. By looking across a range of types of interventions, sample severity, and substances targeted, we found that regardless of severity level or intervention type, most approaches for women had at least one positive outcome.
While many studies recognized the importance of targeting both alcohol and other drug use in interventions, this was not the case for the majority of studies in our review. Strikingly, none of the studies conducted in a MOUD context assessed alcohol use, despite the high rates of co-morbid alcohol use and problems reported in the literature. 98,99 Conversely, many of the studies focused on alcohol only did not report other drug use. Researchers and clinicians who invested in reducing SU and SUDs in women should recognize and address barriers to treatment engagement that disproportionally affect women, as this has the potential to improve treatment outcomes for this population.
Footnotes
Acknowledgments
The authors thank Dr. Anna W. Wright for her assistance with setting up the database and for reviewing search procedures for this review, while completing her PhD in clinical psychology at Virginia Commonwealth University. The authors also thank Ms. Daniela Ocana-Gordillo, a 2016-17 VCU Hubert H. Humphrey Fellow, and the undergraduate students in Dr. Kliewer's Prevention Research Lab who assisted with article title and abstract screening. We are grateful to the Hubert H. Humphrey Program, a Fulbright exchange activity, who supported Ms. Yousaf during 2016-17 year, during which time this project was initiated and partially completed.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.
Supplementary Material
Supplementary Appendix SAP1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.