
Abstract
Background:
Breastfeeding has many positive effects on the health of infants and mothers, however, the effect of breastfeeding on maternal mental health is largely unknown. The goal of this systematic review was to (1) synthesize the existing literature on the effects of breastfeeding on maternal mental health, and (2) inform breastfeeding recommendations.
Materials and Methods:
A literature search was conducted in electronic databases using search terms related to breastfeeding (e.g., breastfeeding, infant feeding practices) and mental health conditions (e.g., mental illness, anxiety, depression), resulting in 1,110 records. After reviewing article titles and abstracts, 339 articles were advanced to full-text review. Fifty-five articles were included in the final analysis.
Results:
Thirty-six studies reported significant relationships between breastfeeding and maternal mental health outcomes, namely symptoms of postpartum depression and anxiety: 29 found that breastfeeding is associated with fewer mental health symptoms, one found it was associated with more, and six reported a mixed association between breastfeeding and mental health. Five studies found that breastfeeding challenges were associated with a higher risk of negative mental health symptoms.
Conclusions:
Overall, breastfeeding was associated with improved maternal mental health outcomes. However, with challenges or a discordance between breastfeeding expectations and actual experience, breastfeeding was associated with negative mental health outcomes. Breastfeeding recommendations should be individualized to take this into account. Further research, specifically examining the breastfeeding experiences of women who experienced mental health conditions, is warranted to help clinicians better personalize breastfeeding and mental health counseling.
Background
The World Health Organization (WHO) and numerous professional societies, governmental and nongovernmental organizations, recommend that infants should be breastfed for at least the first 6 months of life. 1 –5 Evidence supporting breastfeeding includes positive effects on infant immune systems, 3,4,6 –16 reduced risk of sudden infant death syndrome, 4,6,17,18 protection against obesity and diabetes, 4,6,9,19 –22 decreased risk of some pediatric cancers, 6,23,24 and positive effects on cognitive development. 6,25 –27 There are also benefits of breastfeeding to women, including postpregnancy weight loss, 6,28 –31 protection against type 2 diabetes, hypertension, and cardiovascular disease, 3,4,6,31 –36 and lowered risk of breast and ovarian cancer. 3,6,35,37 –39 In addition, breastfeeding can facilitate bonding between mother and baby. 40 –42
Given these benefits and the general cultural sentiment around the world that ‘breast is best,’ many new mothers feel pressured to breastfeed. 42,43 However, some individuals are unable to do so for a variety of reasons, including insufficient milk supply, 3,6,41,44 –46 nipple or breast pain, 3,6,42,44 –46 inadequate latching, 3,4,45,46 and employment needs or obligations, along with lack of accommodations. 9,45,46 Some may make the personal choice to not breastfeed. 46 Regardless of the reason, judgment, and stigma are often experienced by those who do not breastfeed 47,48 ; the judgment can come from others or oneself. If women are unable to breastfeed or choose not to, this can cause a great deal of stress and guilt, which may potentially contribute to a higher incidence of postpartum depression and anxiety. 4,7,41 –43,47,49
Even if women are not experiencing difficulties with feeding or stress from associated expectations, the challenges inherent to breastfeeding, such as lack of sleep, can trigger the onset or exacerbation of mental health conditions. As postpartum mental health conditions have significant negative consequences for mothers and their offspring, including stunted growth, 50 negative effect on children's cognitive and social development, 51,52 and psychological problems and temperament, 51,52 maternal mental health effects associated with the pressure to breastfeed may be more detrimental and outweigh the potential physical benefits of breastfeeding itself.
The goal of this review was to synthesize the existing literature and examine to what extent breastfeeding is associated with symptoms of mental health conditions for women within a year of delivery. We seek to provide information to best inform counseling for individuals experiencing breastfeeding challenges and mental health conditions.
Methods
Database search strategy
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 53 In consultation with a health sciences librarian, we conducted searches in PubMed/Medline (NCBI), PsycINFO (Ovid/Wolters Kluwer), Scopus (Elsevier), CINAHL (EBSCOhost), and Google Scholar in June 2019. The search terms included words related to breastfeeding (e.g., breastfeeding, infant feeding practices, human milk, lactation, breast milk expression) and mental health conditions [e.g., psychosis, psychiatric, mental illness, posttraumatic stress disorder (PTSD), mood disorders, anxiety, depression, maternal mood]. The full search strategy can be found in the Supplementary Appendix SA1.
Inclusion and exclusion criteria
After duplicates were removed, articles of interest were those that reported on the effect of infant feeding method or duration on maternal mental health outcomes. Articles were included or excluded for further review as outlined in PRISMA diagram in Figure 1. Articles were included only if they were in English and were original research articles. The subjects of interest were human women over the age of 18 who were within 1 year postpartum. The mental health outcomes of interest included (1) depression, (2) anxiety, (3) PTSD, (4) obsessive–compulsive disorder, (5) bipolar disorder, (6) psychosis or other psychotic disorder, and (7) other mental health disorders, not including substance use disorders.
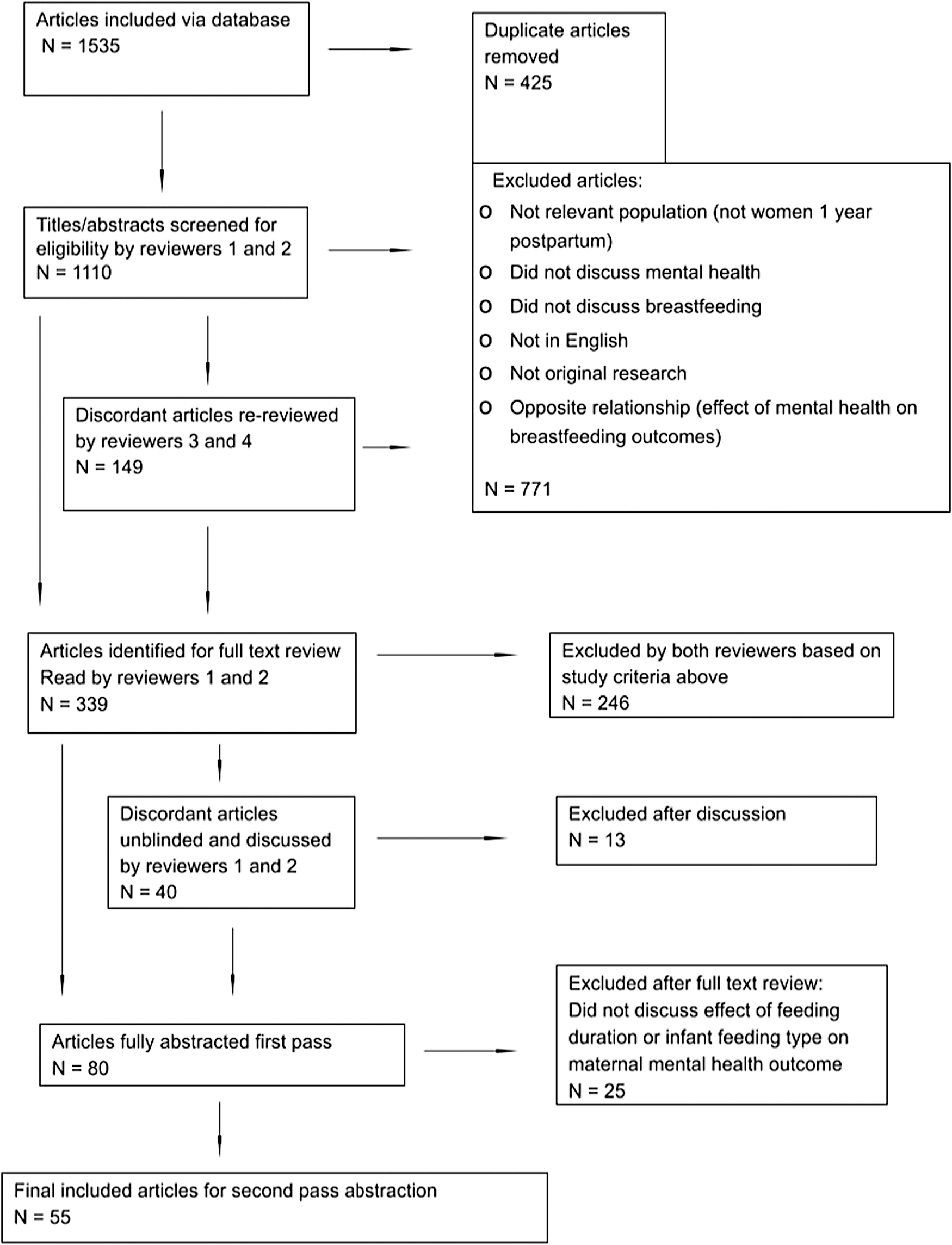
PRISMA diagram.
Articles were carefully reviewed for what was considered the exposure versus outcomes. Articles were included if infant feeding practices where the exposure and mental health symptoms were the outcome; those in which the exposure was mental health, and the outcome was infant feeding practice was excluded (Fig. 1), as we were not interested in the effect of mental health on breastfeeding in this analysis.
Screening phase 1
Reviewers 1 (O.M.) and 2 (M.Y.) reviewed 1,110 titles and abstracts independently on Rayyan 54 for initial eligibility criteria and were blinded to the other reviewer's responses. Articles for which inclusion seemed likely, or exclusion could not be determined based on title and abstract alone, were advanced to the second screening phase. Articles for which Reviewers 1 and 2 were discordant (N = 149) were rereviewed by Reviewers 3 (B.N.) and 4 (F.P., see acknowledgement) for the same determinations. In this phase, 339 of 1,110 articles (30.5%) were sent to screening phase 2 for review of the full text (Fig. 1).
Screening phase 2
Citations for full-text review were entered into Research Electronic Data Capture (REDCap), hosted at the University of Massachusetts Chan Medical School. 55
Reviewers 1 and 2 independently read each article. Reviews resulted in concordance for 246 of 339 articles (72.6%) being excluded and 53 of 339 (15.6%) being included by both reviewers. Forty articles, which had discordant decisions on independent review were unblinded and discussed by Reviewers 1 and 2 until consensus was reached and 27 of those (67.5%) were included (Fig. 1).
Data abstraction
The 80 included articles from screening phase 2 were each fully abstracted using a standard abstraction form by either Reviewers 1, 2, 3, or 5 (G.M.). Abstracted data included study aims, study design, population demographics (race, ethnicity, insurance, age, education), geographic location, time point at which infant feeding method was gathered and approach, time point at which mental health outcome was gathered and type, a summary of pertinent results, and study strengths and limitations.
At this stage, articles that did not explicitly report on the effect of infant feeding method on a specific maternal mental health outcome were excluded. Twenty-five articles were excluded at this stage. Articles that reported on the effect of infant feeding challenges, but not infant feeding method or duration were excluded. This left 55 articles included in final analyses (Table 1).
Characteristics of Included Studies, Breastfeeding, and Mental Health Outcomes
Exclusive breastfeeding: breast milk was the main or only form of infant nutrition, whether or not method of delivery (e.g., at breast vs. pump/bottle) was reported by the authors; Mixed breastfeeding: combination of breast milk through any delivery method and formula or other liquids; Any breastfeeding: used when the authors did not separate exclusive breastfeeding and mixed breastfeeding; No breastfeeding: breast milk was not given as a form of infant nutrition.
Early postpartum: weeks 1 through 6 of the postpartum period; Late postpartum: week 7 through month 12 of the postpartum period.
EPDS, Edinburgh Postnatal Depression Scale; PHQ, patient health questionnaire; DSS, panic disorder severity scale; PSS-SR, posttraumatic symptom scale, self-report version; NIMH, National Institute of Mental Health; CES-D, center for epidemiologic studies depression scale; STAI, State-Trait Anxiety Inventory; DASS, depression anxiety stress scale; PDPI-R, postpartum depression predictors inventory – revised; PTSD, posttraumatic stress disorder; MADRS, Montgomery–Asberg depression rating scale; SCL, symptom checklist.
Each study included in the final analyses was given a quality score based on the revised Downs and Black Checklist. 56 Given the majority (54 of 55) of included articles were observational, the Downs and Black items 3, 4, 8, 9, 11, 14, 15, 19, 23, and 24 were removed, as they were not applicable.
Definitions of breastfeeding as exposure
Breastfeeding was broadly considered as human-made milk provided to an infant whether directly from the breast or expressed and provided through a bottle or similar receptacle. The abstracted articles had heterogeneous definitions of infant feeding, which were operationally categorized to facilitate comparisons. The categories were: (1) exclusive breast milk: breast milk was the main or only form of infant nutrition, whether or not method of delivery (e.g., at breast vs. pump/bottle) was reported; (2) mixed breastfeeding: combination of breast milk through any delivery method and formula or other liquids; (3) any breastfeeding: used when the authors did not separate exclusive breastfeeding and mixed breastfeeding; and (4) no breastfeeding.
Following the initial complete abstraction of data, reviewers identified that several studies reported results on the likely relationship between breastfeeding challenges and maternal mental health. 57 –64 Breastfeeding challenges included poor latch, poor milk supply, painful nipples, breast infection, or negative feelings during breastfeeding, among others. As this was deemed likely highly relevant, each article included at this stage was rereviewed to abstract these data where they existed.
The majority of the authors of the included literature used the terms “woman,” “mother,” and “breastfeeding,” thus this is the language we use throughout the article. However, we acknowledge that not all childbearing or breastfeeding individuals identify as “woman” or “mother.” We recognize historical and contemporary efforts to advocate for reproductive and mental health justice and acknowledge and support these efforts to be more inclusive of perinatal individuals who do not identify as women.
Mental health outcomes
Mental health outcomes of interest included symptoms of depression, anxiety, PTSD, bipolar disorder, psychosis, or other mental health conditions (Table 1). Studies, which discussed only “maternal distress” or similar outcomes, but did not connect this to a mental health disorder, were excluded. For each article, we abstracted the method used by the researchers to determine a mental health outcome, noting that a variety of approaches were utilized. Many used validated screening tools such as the Edinburgh Postnatal Depression Scale (EPDS) for depression or the Panic Disorder Severity Scale (PDSS) for panic disorder. If a measurement tool was utilized, the name and the cutoff score applied by the authors of that article were abstracted. Rather than using screening tools, some articles reported on other mental health-related outcomes, such as admission to hospital for psychiatric illness.
Self-efficacy
A few articles discussed the role of self-efficacy, 63,65 –68 or a person's confidence in being able to breastfeed, in mediating the relationship between infant feeding method and maternal mental health outcomes. For those that discussed self-efficacy, we abstracted relevant results.
IRB statement
This study was reviewed by the Institutional Review Board (IRB) at the University of Massachusetts Chan Medical School and was determined to be a nonhuman subjects' research, and therefore exempt from full review.
Results
Overview of studies
Study characteristics are outlined in Table 1. Of the 55 studies included, there were 34 prospective cohort studies, 58 –60,62,64 –93 nine cross-sectional studies, 94 –102 seven retrospective cohort studies, 61,63,103 –107 three randomized control trials, 108 –110 one retrospective case–control, 57 and one prospective case–control. 111
Twenty-five different countries are represented in this review (Table 1). Sample sizes ranged from 29 participants 91 to 186,452 participants. 73
Table 1 also depicts the definition of breastfeeding and the mental health symptom(s) studied with the screening tool and cutoff score used for each study. It depicts when breastfeeding data were gathered and at what time point mental health was assessed, such as before hospital discharge, early postpartum (up to six weeks postpartum), and late postpartum (between six weeks and 12 months postpartum).
Postpartum depression symptoms were the most represented maternal mental health outcome in this review (52 studies). 57 –61,63 –70,72 –104,106 –111 This was followed by postpartum anxiety symptoms (nine studies). 63,64,66,73,74,81,105,109,111
Effect of breastfeeding on mental health
Nineteen studies 57,60,61,63 –65,67,68,71,74,76 –78,84,90,93,99,105,106 reported no statistically significant relationship between breastfeeding and mental health. Thirty-six studies 58,59,62,66,69,70,72,73,75,79 –83,85 –89,91,92,94 –98,100 –104,107 –111 found a statistically significant relationship, 29 of which found that breastfeeding was associated with fewer mental health symptoms, 58,59,62,66,69,70,72,75,79 –82,85,88,89,92,94 –97,100,102 –104,107 –111 one of which found that breastfeeding was associated with increased maternal mental health symptoms, 91 and six of which described a mixed association between breastfeeding and mental health. 73,83,86,87,98,101
Effect of breastfeeding on postpartum depression symptoms
The majority of studies, 52 in total, examined the relationship between breastfeeding and symptoms of postpartum depression 57 –61,63 –70,72 –104,106 –111 (Table 2). Of these, 34 studies identified a statistically significant relationship. 58,59,66,69,70,72,75,79 –83,85 –89,91,92,94 –98,100 –104,107 –111
Effect of Breastfeeding on Postpartum Depression Symptoms
Inverse: breastfeeding decreased the risk of postpartum depressive symptomatology. Direct: breastfeeding increased the risk of postpartum depressive symptomatology
PSE, present state examination; PPD, postpartum depression; MINI, Mini International Neuropsychiatric Index.
A total of 28 studies 58,59,66,69,70,72,75,79 –82,85,88,89,92,94 –97,100,102 –104,107 –111 found that breastfeeding was associated with a decreased risk of postpartum depression symptomatology. A single study 91 reported that breastfeeding increased the risk of depressed mood during the first week postpartum. Five studies 83,86,87,98,101 identified both positive and negative effects of breastfeeding on mental health, either between different subgroups 86,98,101 or at different time points 83,87 For example, one study found bottle feeding was associated with the highest risk of depression symptoms, followed by exclusive breastfeeding, and mixed breastfeeding with the lowest risk. 101
The final study 73 is reported separately given its large sample size and that its primary endpoint was postpartum hospital admission with psychiatric diagnosis; this would indicate more severe disease than the other studies. There were 186,452 included participants and no statistically significant relationship between breastfeeding status and postpartum depression symptoms was found. However, since hospitalization was used as the endpoint, this article did not report data on women who had depression symptoms but were not hospitalized. This article will continue to be reported on separately given its large sample size compared with other studies, its markedly different endpoint compared with other studies, and questionable directionality of the association between breastfeeding and mental health.
Effect of breastfeeding on postpartum anxiety symptoms
Of the nine studies in which the mental health outcome was postpartum anxiety symptomatology (Table 3), four 66,73,81,109 identified a statistically significant relationship. Three studies 66,81,109 reported that breastfeeding was associated with a reduced risk of postpartum anxiety symptoms. One study 73 found that nonbreastfeeding reduced the risk of hospitalization from anxiety disorder. However, as reported above, this study used hospitalization as its endpoint and, therefore, is not comparable to the remainder of studies.
Effect of Breastfeeding on Postpartum Anxiety Symptoms
Inverse: breastfeeding decreased the risk of postpartum anxiety symptomatology. Direct: breastfeeding increased the risk of postpartum anxiety symptomatology.
PMQ, panic manifestation quotient.
Effect of breastfeeding on other mental health symptoms
Three studies 62,71,73 looked at a variety of other mental health outcomes (Table 4). Two of these studies 62,73 reported statistically significant results. The large aforementioned study 73 found no effect of breastfeeding on hospitalization with adjustment disorder or a personality disorder. They did however, find that non-breastfeeding was associated with an increased risk of hospitalization with bipolar disorder or schizophrenia within 1 year postpartum. Another study 62 found that exclusive breastfeeding was associated with a decreased risk of symptoms of postpartum PTSD. The final study 71 reported no relationship between breastfeeding and postpartum psychosis symptoms.
Effect of Breastfeeding on Other Postpartum Mental Health Symptoms
Inverse: breastfeeding decreased the risk of postpartum mental health disorder symptomatology. Direct: breastfeeding increased the risk of postpartum mental health disorder symptomatology.
PSS-SR, posttraumatic symptom scale, self-report version; PHQ, patient health questionnaire.
Breastfeeding difficulties, breastfeeding self-efficacy, and maternal role attainment
Eight studies 57 –64 reported on the effect of breastfeeding difficulties on postpartum mental health outcomes (Table 5). Breastfeeding difficulties had varied definitions, including latching problems, nipple pain, negative emotions during infant feeding, breast infection, and lack of milk supply. Five studies 57 –60,62 found that breastfeeding challenges or noninitiation of breastfeeding despite intention to do so was associated with higher risk of symptoms of maternal mental health conditions, including depressive symptomatology or posttraumatic stress symptoms. For example, Beck et al. found that women with more physical challenges to breastfeeding and women who did not breastfeed as long as they desired had higher PTSD symptomatology. 62
Effects of Breastfeeding Challenges and Self-Efficacy
Maternal Role Attainment, Women who had high Maternal Role Attainment (MRA) have strong beliefs about the importance of breastfeeding for fulfilling the maternal role; MADRS, Montgomery–Asberg Depression Rating Scale.
Five studies 63,65 –68 examined the effects of breastfeeding self-efficacy, or a woman's confidence in breastfeeding, on mental health outcomes (Table 5). Four of these 65 –68 found that worry about breastfeeding or dissatisfaction with breastfeeding progress was significantly associated with higher depressive symptomatology at various time points. The fifth study 63 reported that higher maternal self-efficacy was associated with durations of exclusive breastfeeding greater than six months postpartum.
Two studies 63,68 investigated the interplay between breastfeeding difficulties and self-efficacy, and how these factors combined contribute to maternal mental health outcomes. Henshaw et al. found no significant relationship between self-efficacy, ease of breastfeeding, and mood outcomes when examined together, although breastfeeding problems had an independent effect on depression. 68 De Jager et al. reported that women who had higher levels of breastfeeding self-efficacy and fewer breastfeeding difficulties were more likely to exclusively breastfeed for six months or more. 63
Cooke et al. explored the concept of Maternal Role Attainment (MRA) in the context of breastfeeding using the MRA subscale of the Maternal Breastfeeding Evaluation Scale (MBFES), which describes the extent to which a woman views successful breastfeeding as an important part of her identity as a mother. 64 Women who had higher MRA subscale scores were less likely to stop breastfeeding at three months postpartum than women with lower scores, however, if they did stop breastfeeding, they had higher EPDS scores. 64 Women with low MRA and no breastfeeding difficulties were more likely to stop breastfeeding than those with higher MRA who experienced breastfeeding challenges.
Discussion
This systematic review synthesized heterogeneous literature regarding the effects of breastfeeding on postpartum maternal mental health. The mixed results suggest there is a complex relationship influenced by numerous factors. The majority of studies concluded that breastfeeding is associated with fewer mental health symptoms or there was no relationship between breastfeeding and maternal mental health. However, when breastfeeding challenges and low self-efficacy were present, there was an association with increased mental health symptomatology.
Biological effects of breastfeeding
There is biologic plausibility for breastfeeding to have protective effects on perinatal mental health through release of oxytocin. In their systematic review, Uvnäs Moberg et al. concluded that breastfeeding resulted in an immediate release of oxytocin, especially in multiparous women, and was associated with decreased maternal cortisol levels and anxiety. 112 This suggests that breastfeeding may have immediate short-term effects on maternal mood. These positive effects of breastfeeding are likely mediated by the robust activation of the reward pathway by oxytocin, dopamine, and the overall neural response to the act of breastfeeding. 113,114
These beneficial effects of oxytocin and related maternal hormones are maximized in positive breastfeeding environments, where there are synergistic benefits to the mother and child due to the transmission of oxytocin through breast milk and synchronicity in diurnal endocrine rhythms and behavior. 115
Breastfeeding challenges can be an intense, chronic stressor for mothers, which is likely to disrupt the typical role of oxytocin in the modulation of maternal mood. Disruptions in the oxytocinergic system have been associated with postpartum depression, 116,117 and symptoms of anxiety in mothers have been associated with low levels of oxytocin. 118 However, clinical trials with intranasal oxytocin administration in depressed mothers have had conflicting results, with acute oxytocin increasing general sadness but improving positive perceptions of the maternal-infant relationship. 119
Breastfeeding challenges
There are misconceptions that breastfeeding is “natural” and is thus easy and intuitive. In reality, many women perceive and/or experience inadequate support from their community, including health care providers, not only during breastfeeding, but also with cessation. 42,43,120 In this review, we found that breastfeeding difficulties, including nipple pain, latching difficulties, diminished milk supply, or unsuccessful breastfeeding initiation are associated with an increased risk of negative mental health symptoms. As Williams notes, “seldom do we willingly encourage others to picture their future breastfeeding experience to include traumatized nipples, screaming, back-arching, breast-refusing infants, or hours spent in a love–hate relationship with the breast pump or other gadgets.” 121
These challenges may lead to a shorter duration of breastfeeding than intended or desired, and subsequent feelings of inadequacy or failure, which may increase the risk of postpartum depression symptoms. It is important to identify women with breastfeeding challenges and increase both lactation support and mental health counseling. Breastfeeding recommendations must be individualized and consider the potential negative impact of breastfeeding challenges on maternal mental health. In such situations, recommendations may include discontinuing breastfeeding.
MRA and the role of stigma
The results from Cooke et al., who reported on MRA, suggest that a woman who views breastfeeding as integral to her role as a mother may be more likely to continue breastfeeding despite difficulties. Those with higher MRA scores have greater expectations of themselves to breastfeed, and when this does not continue, may feel even more disappointed and guilty than those who view breastfeeding as less essential to their maternal role. 64
The extent to which a mother considers breastfeeding an integral factor in her maternal role may depend on the cultural importance placed on breastfeeding and the stigma associated with nonbreastfeeding. As noted in previous literature, 122 stigma negatively impacts mental health and prevents recovery from mental illness. The cultural support of breastfeeding may positively impact maternal mental health if initiation of breastfeeding is successful and continues, but may negatively impact maternal mental health if breastfeeding is unwanted or challenging. 123
Societal pressures to breastfeed may influence one's self-imposed pressure to do so as well. However, as described by Mozingo et al., women who stopped breastfeeding within two weeks of initiation consistently described an incongruity between their idealized thoughts of breastfeeding and the reality of their actual experience, resulting in a sense of failure, guilt, disappointment, or shame about breastfeeding cessation, and self-doubt. 120 This finding has been supported in related investigations. 42,43
Likely in relation to the cultural stigma associated with not breastfeeding, it is unsurprising that the literature suggests the interplay between infant feeding method and maternal mental health outcomes is impacted by factors, including maternal self-efficacy in breastfeeding, physical challenges with breastfeeding, and the extent to which a woman believes breastfeeding is an important part of her maternal identity. These factors may cause breastfeeding challenges to worsen mental health symptoms in some women.
Strengths
This review synthesizes associations between breastfeeding and multiple maternal mental health outcomes. While literature exists addressing the relationship between maternal mental health on breastfeeding, this review aimed to explore the relationship in the opposite direction. Importantly, we investigated the impact of breastfeeding challenges and breastfeeding self-efficacy on maternal mental health, which are relationships that merit further exploration in the literature.
This review includes a large number of studies and total participants. It is a multinational review with studies from 25 different countries from North America, Europe, Asia, and Australia, representing many cultures, which have differing views on mental health and breastfeeding practices. The wide representation of countries contributes to the generalizability of these study results across many populations globally.
Limitations
This review has several limitations, namely that our interpretive abilities are limited due to the very heterogeneous nature of the existing literature. The authors of the original included articles used diverse methods of defining and measuring breastfeeding, and at times, the definitions of breastfeeding were not always explicitly stated. Similarly, mental health outcomes were measured at different time points postpartum with various measurement tools, which impacted the ability to compare outcomes in a standardized way. Additionally, in the included studies, mental health before initiation of breastfeeding was reported in diverse ways.
Many studies excluded women with a history of mental illness, 57,58,71,78,79,88,94,97,103,105,109,111 however, the mental illnesses excluded were not consistent across studies, as some excluded women with a history of any mental illness and others excluded women with a history of only certain mental illnesses. Other studies excluded participants with current psychotropic medication use. 59,90,107
In more than one third of the included studies, 60 –63,69,70,75 –77,83,89,91,95,98,99,102,106,108 there was no assessment of mental health before initiation of breastfeeding. We did not formally abstract or analyze data specific to mental health conditions with preconception or pregnancy onset; this is an opportunity for future research.
It is possible that some of the protective effects of breastfeeding on maternal mental health described in this review are due to the stable or supportive psychosocial conditions in women who breastfeed compared with women who do not, leading to potential selection bias. However, the information gathered in these studies is not sufficient to address this limitation, and further understanding of the psychosocial conditions of women who do and do not breastfeed and their impact is warranted.
The preparation of this article was delayed due to the COVID-19 pandemic. It is limited by not including studies published after our original search was conducted and through the pandemic. However, given the impact of the pandemic on mental health, even with an updated search, we would choose to exclude articles published after the onset of the pandemic.
Additionally, it is worthy of noting that all systematic reviews are limited by publication bias, which references the decreased likelihood of studies with negative effects or nonstatistically significant findings to be published, resulting in peer-reviewed publications being skewed toward research with positive results. Outcome reporting bias also addresses the fact that many studies collect a wide range of outcomes yet often all are not reported. For example, the data presented on breastfeeding challenges were compelling. For the studies that did not report this, we do not know if it was not collected at all or was not reported.
Finally, the clinical significance of the results in the original articles was not always reported. Small differences in EPDS scores have unknown clinical significance. As breastfeeding can be challenging for mothers, it is imperative that mothers know the clinical, not only statistical, significance of exclusive breastfeeding on their risk of mental illness to make personal decisions about initiating or continuing breastfeeding in the context of experiencing breastfeeding challenges.
Future research should more clearly elucidate the relationship between breastfeeding and maternal mental health by measuring maternal mental health before and after breastfeeding onset to examine causality between breastfeeding and maternal mental health rather than mere association. Future studies should consistently examine outcomes within the DSM-5 definitions and criteria using validated tools, and researchers should comment on the clinical significance of their results.
To more fully understand the relationship between breastfeeding challenges and mental health, we need to more fully explore the actual breastfeeding experiences of people with perinatal mood and anxiety disorders, as well as conducting more focused research with people who intend to breastfeed but did or could not. Phenomenological approaches that capture women's own words would help to inform a future body of research that adequately addresses some of the limitations mentioned above, along with standardized data definitions.
Recommendations
Beyond research, there are practical recommendations that can be derived from the studies included in this review and the clinical experience of its authors. First and foremost, perinatal individuals should be asked how they are feeding, or planning to feed their baby (as opposed to being asked if they are breastfeeding). This simple, open-ended and nonleading question goes a long way toward destigmatizing lack of intention to breastfeed, breastfeeding challenges or cessation, and mixed or formula feeding.
If and when a woman shares her intention to breastfeed, and especially if it is her first time, she should be informed about the full range of possible experiences, including common challenges and stressors. 124,125 Honesty and transparency about breastfeeding will likely mitigate feelings of guilt or failure that many women feel when their breastfeeding experience does not match their plans and expectations. 126,127 Additionally, all perinatal mental health assessments should include questions about feeding intention and experience, so that women are not bearing the burden of bringing up a potentially difficult topic. 128
Any discussion about infant feeding should incorporate all aspects of the patient's life, including her partnership status, level of familial and social support, exposure to systemic racism and other structural stressors, work situation and financial status, and everyday logistics such as commuting, caregiving, and the ease of providing for her and her family's most basic needs. 129,130 Women who do present with significant breastfeeding challenges and perinatal mental health issues should be supported to make whatever decision is best for themselves and their families. Professionals should refrain from presenting all-or-nothing scenarios, given that many women combine breast and formula feeding in ways that allow them to enjoy successful, and if they so choose, long-lasting breastfeeding relationships with their children. 131,132
Conclusions
There is a complex relationship between breastfeeding and maternal mental health. When considering the impact of breastfeeding on maternal mental health, we need to take into account one's perception of breastfeeding and the breastfeeding experience. While we found that breastfeeding was often associated with fewer maternal mental health symptoms, this was not the case when breastfeeding difficulties or a discordance between maternal role expectations and actual experience were present. In fact, difficulties and discordance were associated with poorer mental health outcomes.
The effect of breastfeeding on maternal mental health outcomes appears to be dependent on the emphasis an individual person places on the importance of breastfeeding for motherhood. For some, breastfeeding is an important part of their maternal identity, and difficulties with breastfeeding may put them at risk for depression, anxiety, or other mental health conditions. For others, maternal identity is formed in other ways and stopping breastfeeding may not put them at similar risks.
With this review, we sought to decrease the stigma surrounding lack of breastfeeding or mixed feeding, as breast may not always be the best option. Further research is needed to elucidate the relationship between breastfeeding and maternal mental health so that clinicians can best individualize breastfeeding counseling for their patients, which at times, may include breastfeeding cessation in the event of negative maternal mental health outcomes.
Footnotes
Acknowledgment
The authors thank Florent Pittet for his assistance with the screening of articles for this review.
Authors' Contributions
The co-first authors on this article contributed equally at all stages of the review, including screening, data abstraction and analysis, and writing the article. All other authors met all four criteria for authorship, including substantial contributions to the design of the review, analysis and interpretation of data, drafting or revising the work, and final approval of the version to be published.
Author Disclosure Statement
Dr. Byatt has received salary and/or funding support from Massachusetts Department of Mental Health through the Massachusetts Child Psychiatry Access Program for Moms (MCPAP for Moms). She is also the statewide Medical Director of MCPAP for Moms and the Executive Director of Lifeline for Families. She has served on the Medscape Steering Committee on Clinical Advances in Postpartum Depression and the Behavioral Health Network of Excellence for the Kinetix Group. She received honoraria from Medscape, Mathematica, and the Global Learning Collaborative.
Dr. Moore Simas is a consultant for the Massachusetts Child Psychiatry Access Program for Moms (MCPAP for Moms), as Obstetric Engagement Liaison. She is also the Medical Director of Lifeline for Moms, which is part of the University of Massachusetts Chan Medical School.
None of the other authors has any disclosures to report.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.