
Abstract
Objective:
We assessed whether general practitioner (GP) delivery of a vaginal self-sampling kit was non-inferior to home-mailed delivery on cervical cancer screening (CCS) participation.
Methods:
Two hundred and ten French GPs from Indre-et-Loire French department were randomized into two groups, and their unscreened women patients aged 30–65 were included in February–March 2015. In the GP delivery group (n = 105 GPs; 1,806 women), women were sent a reminder letter inviting them to collect a vaginal self-sampling kit at their regular GP's practice. In the home-mailed delivery group (n = 105 GPs; 1,806 women), women were sent a reminder letter with a vaginal self-sampling kit directly at home. The primary outcome was participation in complete CCS within 9 months. A cost-effectiveness analysis was also performed.
Results:
At 9 months, 14.9% (95% CI: 12.9–16.9) and 27.9% (95% CI: 25.7–30.0) of women in the GP and home-mailed delivery groups participated in complete CCS. The absolute between-group difference was −13.0 percentage points (95% CI: −15.9 to −10.0) in favor of the home-mailed delivery group, crossing the non-inferiority pre-defined non-inferiority margin of 5%. The home-mailed delivery strategy cost 50.81€ more per additional woman screened.
Conclusions:
The GP delivery was inferior to home-mailed delivery in increasing participation in CCS. Home-mailed delivery of a vaginal self-sampling kit is a cost-effective way to increase CCS in that the additional cost of this strategy seems acceptable. This study is registered at
Introduction
Cervical cancer is the third female cancer worldwide, with 569,847 estimated new cases and 311,365 deaths in 2018. 1 In mainland France, 2,920 new cases and 1,120 deaths from cervical cancer were estimated in 2018. 2 Organized cervical cancer screening (CCS) programs based on Papanicolaou cytology (Pap smear) have shown their efficiency in reducing cervical cancer incidence and mortality in most developed countries. 3
When the study took place, France had no national CCS program, but 9 regions had a pilot program (based on Pap smear, as HPV test was not yet recommended in France at this time). During 2010–2012, the screening coverage was 62.3% over those 9 areas and 60.5% in Indre-et-Loire French department, 2 far from the national objective of 80%. 4 Because most cervical cancers occur in unscreened women, 5 we need complementary strategies to reach these women. 6
Persistent infection with high-risk papillomavirus (HR-HPV) is the necessary risk factor for cervical cancer. 7,8 For women 30–65 years old, HR-HPV-based tests are more sensitive to detect cervical intra-epithelial neoplasia grade 2–positive (CIN2+) lesions than is Pap smear, and the screening interval could be extended to 5 years for HR-HPV-negative women. 9 Using the HR-HPV-based test as a primary screening test opens the possibility of self-sampling. By offering an in-home test performed by women themselves, many adherence barriers to that screening could be lifted. HR-HPV tests of vaginal self-sampling with a PCR step show similar sensitivity as clinician sampling to detect CIN2+ lesions. 10
Several randomized controlled trials have shown greater participation when using a vaginal self-sampling kit mailed to unscreened women as compared with sending an invitation for a screening test performed by a health professional, whatever the self-sample device and the setting of the trial (pooled relative participation in intent-to-treat-analysis of 2.33, 95% confidence interval [CI] 1.86–2.91). 11 Offering a self-sampling kit to unscreened women could increase CCS coverage, but its weaknesses are lack of contact with a health professional and wasted resources.
The APACHE-3 trial aimed at assessing the noninferiority of general practitioner (GP) delivery as compared with home-mailed delivery of a vaginal self–sampling kit on CCS participation. As the cost of GP delivery is expected to be lower, a cost-effectiveness analysis was also performed to assess the efficiency of this strategy.
Methods
Study design
The APACHE-3 trial was a noninferiority two-parallel-group cluster randomized controlled trial. Randomization units were GPs from the Indre-et-Loire French department. A cluster design was chosen for logistical and economic considerations and to avoid contamination within general practices.
The study protocol was approved by the local ethics committee (n°2014-R30), and a waiver of individual participant-level informed consent was granted.
Settings and participants
The present study took place in the Indre-et-Loire French department where about 160,000 women are targeted for CCS. In the regional program, unscreened women aged from 25 to 65 years old are routinely identified by crossing information from different sources: target population file and Pap smear reimbursement data from health insurance organizations and the major part (∼90%) of Pap smear results from pathologists' labs.
By crossing the different sources of information, we considered that data on screening status were almost exhaustive. Unscreened women (no Pap smear in the past 3 years) receive an invitation letter from the Cancer Screening Department to have a Pap smear performed by their GP, gynecologist, or midwife. Nine months later, in the absence of Pap smear data, a reminder letter is sent.
Eligible women were 30–65 years old who declared one of the randomized GPs as referring GP and did not have a Pap smear within 9 months after an invitation letter. We included all women meeting first the inclusion criteria between February and March 2015 until reaching the target sample size of 3,612 women. The number of selected women could, thus, vary across the GPs.
Randomization and masking
The whole trial process with blinding at each step is described in Figure 1. 12 In October 2014, a random sample of 210 among the 527 GPs registered in the Indre-et-Loire area was included in the trial. There were no specific eligibility criteria for GPs. These 210 GPs were randomized with a 1:1 ratio to GP delivery or home-mailed delivery group. To avoid contamination, GPs practicing within the same medical practice were allocated to the same group. The allocation sequence was computer-generated and stratified on the practice size according to five strata (practices with 1, 2, 3, 4 or >4 GPs) by a statistician not further involved in the study.
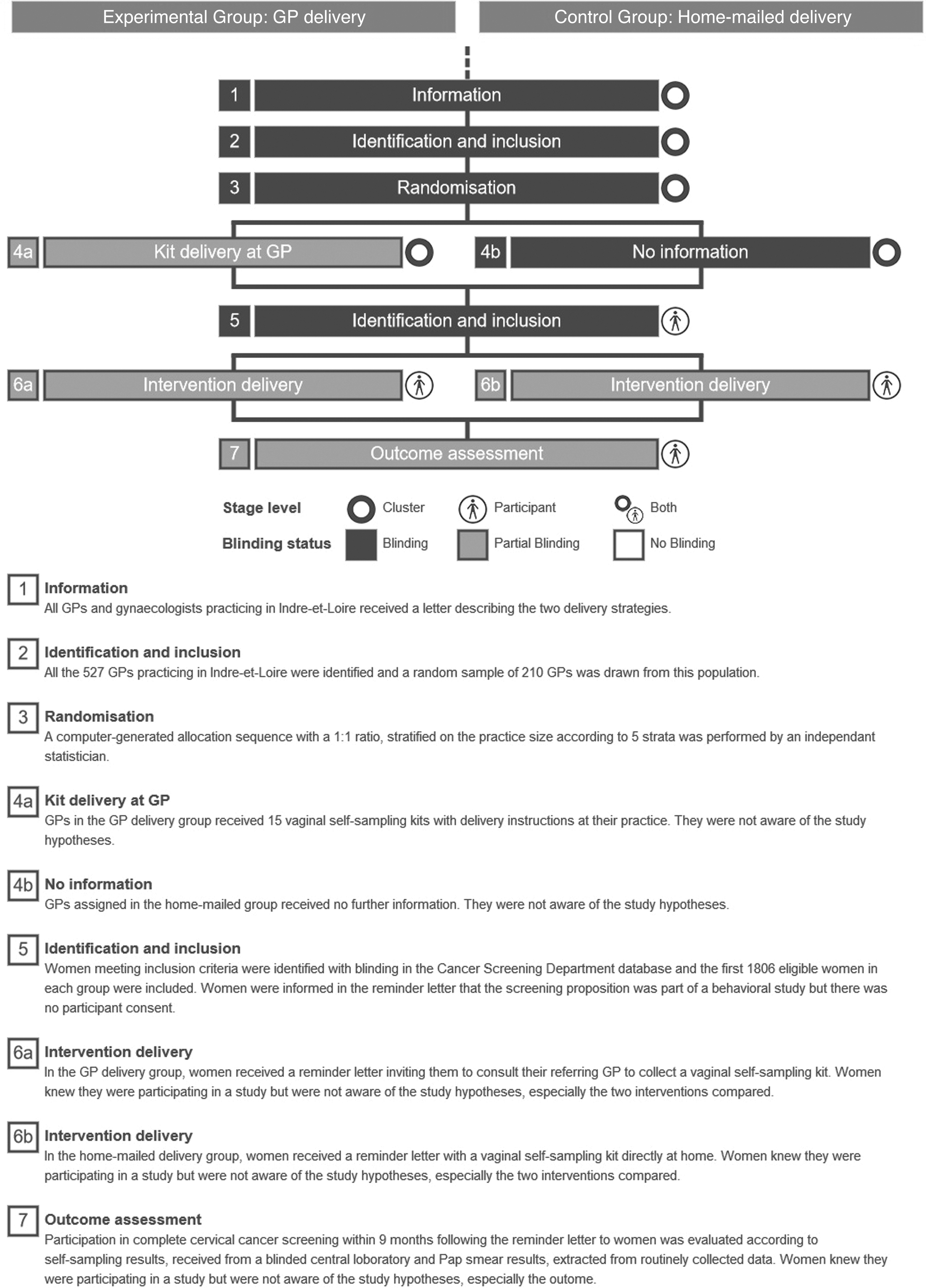
Timeline and blinding status of the cluster randomized trial process.
The selection of women was handled by an independent computer programming company that is in charge of the screening program management software routinely used in the Cancer Screening Department (Zeus, OsiSanté, Thury-Harcourt, France) and that was not further involved in the study.
Owing to the nature of the intervention, GPs in the GP delivery group and women in both groups were aware of their group allocation but they were not aware of the study hypotheses. The women were not aware of the alternative intervention. Moreover, risk of bias was limited by the fact that the primary outcome was collected from routinely collected data and laboratory results measured by a blinded staff.
Interventions
Before the start of the trial, every GP and gynecologist practicing in the Indre-et-Loire region received a letter to inform them about the two delivery strategies, to sensitize them about vaginal self-sampling, and to let them know they could receive results letters for their patients.
In the GP delivery group, GPs were provided with 15 vaginal self-sampling kits, instructions for their delivery, and a copy of the letter that would be sent to included women. Eligible women received a reminder letter inviting them to consult their referring GP to collect a vaginal self-sampling kit. They were asked to use the kit at home.
In the home-mailed delivery group, GPs received no further information. Eligible women received a reminder letter with a vaginal self-sampling kit directly at home.
In both groups, the vaginal self-sampling kit consisted of (1) a leaflet explaining how to perform the vaginal self-sampling (Supplementary Appendix SA), (2) a validated nylon flocked swab in a non-breakable dry sterile tube (52980C, Copan, Brescia, Italy), 13,14 (3) a resealable plastic bag, (4) an identification sheet, and (5) a pre-stamped, pre-addressed envelope to return the self-sampling to a centralized laboratory (Virology Laboratory of the University Hospital of Tours, France) for HR-HPV testing.
In both groups, women could opt for a pap smear instead of self-sampling.
Practical course
Definitions of success and failure of the screening procedures were standardized (Supplementary Fig. S1). In case of a second uninterpretable HR-HPV test result, women were advised by phone to have a Pap smear. Women with negative HR-HPV test results were advised to have a Pap smear 3 years later. Women with positive HR-HPV test results were recommended to have a triage Pap smear within 3 months; they were re-contacted at 3 and 6 months after the HR-HPV results if the Pap smear was not performed within the time limit. In case of abnormal results, follow-up data were collected according to the French guidelines. 15
Laboratory testing
The self-sampling device was first eluted in an adapted buffer (Abbott Cervi Collect specimen collection kit). HR-HPV detection was performed in a centralized laboratory (Virology Laboratory of the University Hospital of Tours, France) with a real-time PCR-based assay (Abbott RealTime High Risk HPV). 16,17 This assay is intended to detect 14 HR-HPV genotypes—16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68—and to genotype specifically type 16 and 18. An endogenous human beta globin sequence is detected as a sample validity control for cell adequacy, sample extraction, and amplification efficiency.
In case of negativity for this control, a diluted sample was analyzed to exclude the presence of inhibitors. If the second test was negative for this internal control, the test result was considered uninterpretable. The HR-HPV results were classified as positive for HR-HPV when at least one HR-HPV genotype was detected and negative when no HR-HPV genotype was detected. Pap smears were evaluated in cytology laboratories according to usual practices. Laboratory tests were performed by staff with blinding to the group.
Outcome measurement
The primary outcome was the woman's participation in complete CCS within 9 months after the reminder letter. In both groups, participation in complete screening was defined as having a Pap smear or performing the self-sampling, completed by a triage Pap smear in case of positive results (within 9 months after the HPV results) (Supplementary Fig. S1).
Secondary outcomes were: (1) participation in complete CCS via vaginal self-sampling within 9 months after the reminder letter and (2) participation in complete CCS with a Pap smear within 9 months after the reminder letter.
Cytology (Pap smear) and histology (biopsy) results were extracted from routinely collected data from the Cancer Screening Department database. Pap smear results were classified by the 2014 Bethesda system. 18 Histology results were classified as normal, CIN1, CIN2, CIN3, or cancer.
Data collection
Baseline characteristics for patients, GPs, and practices were extracted from the Cancer Screening Department database. HR-HPV test and Pap smear results were extracted from routinely collected data from the Cancer Screening Department database.
Statistical analysis
On the basis of results from a previous trial, 14 we assumed a 20% participation in complete cervical screening percentage in both groups. The noninferiority margin was fixed at 5%. Considering a power of 90% and a two-sided alpha of 5%, we needed 1,350 women per group. We applied a variance inflation factor because clusters (i.e., GPs) and not participants were randomized. By using the Cancer Screening Department database, we estimated an average number of eligible women per GP of 17.2, with a coefficient of variation of 0.9.
The inflation factor was calculated with the Eldridge et al. approach 19 : This factor is defined by 1 + [(CV 2 + 1) m-1] ρ, where CV is the coefficient of variation associated with the size of the clusters, m is the average cluster size, and ρ is the intraclass correlation coefficient (ICC). Considering an ICC of 0.01 (this value was chosen according to the nature of the primary outcome, which is an “outcome” variable as opposed to a “process” variable, reflecting an individual choice, probably moderately affected by the cluster effect), the inflation factor was 1.30, leading to a sample size of 1,755 women per group. We planned to include 105 GPs, each associated with 17.2 women, on average, for 1,806 women needed per group.
The aim of the trial was first to assess the non-inferiority of GP delivery versus home-mailed delivery and in case non-inferiority was shown a second analysis would determine whether GP delivery was superior to home-mailed delivery (switch to superiority objective). Each analysis was planned to be tested at a one-sided type I error of 2.5%. 20
The primary analysis was performed at the individual level, according to the intention-to-screen principle. The GPs who changed their practice after randomization (practice cessation, address modification) were excluded from the analysis. For the primary outcome, percentages were reported with their 95% CIs. The estimation of the two-sided 95% CI from the between-group difference in participation percentages involved using a normal approximation.
Variances were adjusted for clustering at the GP level by using a ratio-estimator approach. Noninferiority would be declared if the lower boundary of the 95% CI of the between-group difference in the percentage of women with complete CCS (percentage in the GP delivery group minus percentage in the home-mailed delivery group) was not less than −5 percentage points. The same approach was used for secondary outcomes. Pre-specified subgroup analysis (age <50 vs. ≥50 years old) involved using a mixed logistic regression model with intervention group, subgroup and group*subgroup interaction as fixed effects, and cluster as a random effect.
The ICCs were estimated with the Fleiss and Cuzick estimator in each group with their 95% CIs obtained with the Zou and Donner method, 21 with values truncated to zero in case of negative estimation. Analyses involved using SAS v 9.4 (SAS Institute, Inc., Cary, NC).
Health-economic evaluation
Cost-effectiveness analysis involved using TreeAge 2017 software, modeling the women's pathway in a decision tree based on observed data from the APACHE 3 study. Effectiveness data corresponded to the primary outcome (success or failure). Direct medical costs arising between randomization and evaluation of the primary outcome were included in the analysis. For both groups, costs considered in the analysis were: costs for the different reminder letters (stationery, printing, labor required to prepare the mailing and postage) according to the groups; costs of postal return of self-sample to laboratory; costs of laboratory analysis (HR-HPV test) and mailing tests results; in case of uninterpretable result, costs for sending a second vaginal self-sampling kit; costs of reminder letters and phone calls after a positive HR-HPV result on the vaginal self-sampling without triage Pap smear, costs of consultation to perform a Pap smear (GP, midwife or gynecologist) including potential extra fees and costs of Pap smear analysis (cytology analysis) and result sending.
In the home-mailed delivery group, the cost of a vaginal self-sampling kit was considered for each reminder. In the GP delivery group, specific costs considered were: GP's consultation, vaginal self-sampling kit and the sending of this kit to GP. All these costs are detailed in Supplementary Table S1. Costs have been valued from a societal point of view (i.e., costs covered by health insurance, Cancer Screening Department, and women). No discounting was applied.
Mean cost per woman and cost-effectiveness ratios were calculated for each group. The incremental cost-effectiveness ratio (ICER) per extra screened woman was calculated by dividing the between-strategy mean cost per woman difference by the between-strategy rate of screened women at 9 months. One-way and deterministic sensitivity analyses were performed to evaluate the extent to which the uncertainty in effect and cost data would change the ICER.
Results
GPs and participants
Among the 210 randomized GPs (Fig. 2), 4 GPs in the GP delivery group and one in the home-mailed delivery group had stopped their activity (retired or changed practice) before the inclusion of women. One GP in the home-mailed delivery group had no eligible patient. From February to March 2015, 3,612 women, patients of the randomized GPs, were included in the study (1,806 in each group). The mean (standard deviation) age of included women was 50.6 years (11.2) and 48.9 years (11.1), respectively.
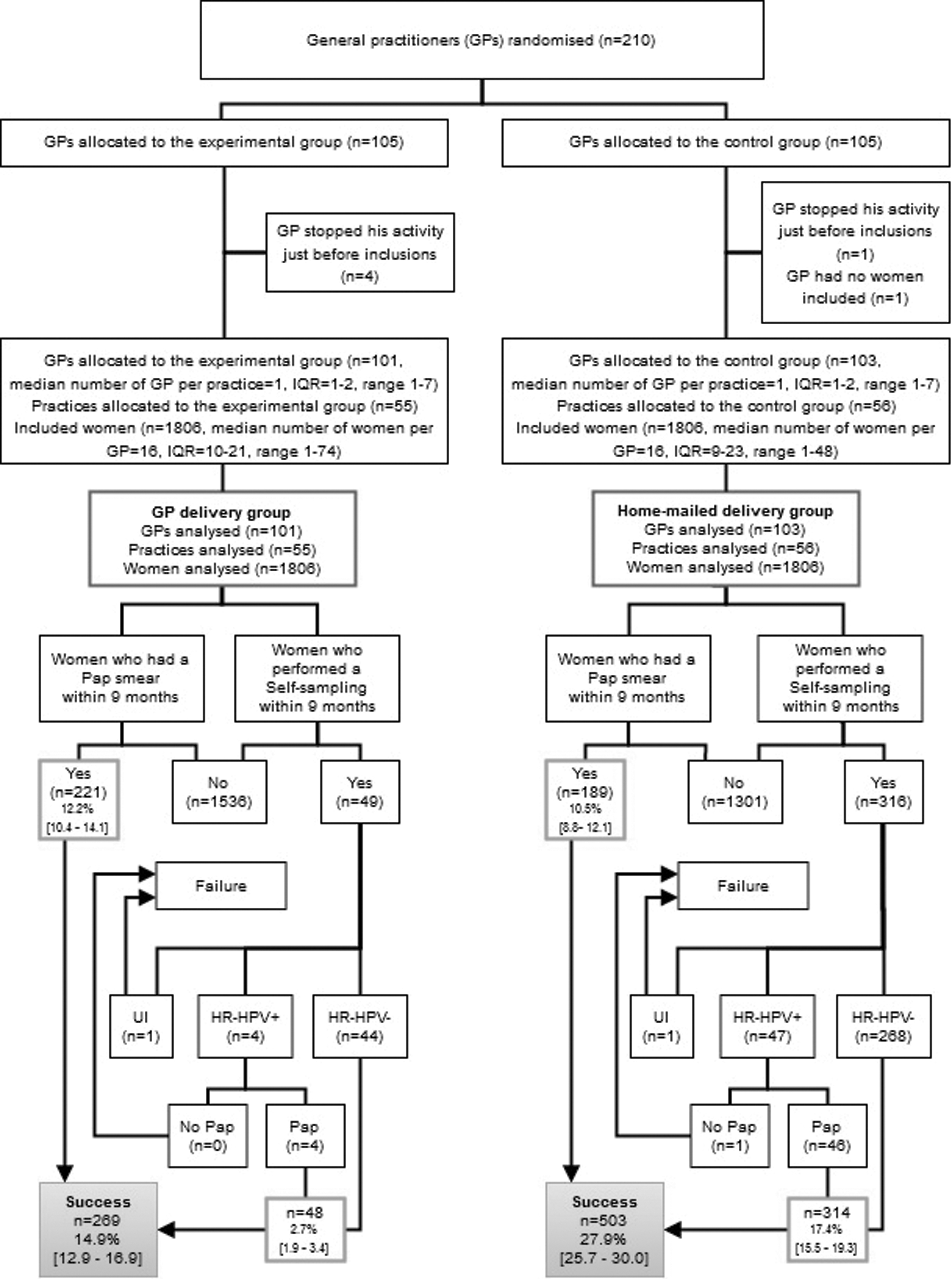
Study flow chart and results. HR-HPV+, positive for high-risk HPV; HR-HPV-, negative for high-risk HPV; UI, uninterpretable HPV test result; IQR, interquartile range; GP, general practitioner; PAP, Papanicolaou cytology. Ninety-five percent confidence intervals are presented in brackets.
Study conduct
In the GP delivery group, 2 women had an uninterpretable HPV test result; one performed a second self-sampling. In the GP delivery group, some GPs gave the self-sampling kit to women not included in the study. In that case, the self-samplings were not analyzed by the centralized laboratory. Those women were advised by the Cancer Screening Department staff to have a Pap smear performed by a health care provider. The GPs in this group received phone calls and a reminder letter about delivery conditions.
Participation in complete CCS
In the GP delivery group, 269 of the 1,806 women (14.9%) participated in complete CCS within 9 months versus 503 of the 1,806 women (27.9%) in the home-mailed delivery group (Fig. 2 and Table 1). The absolute risk difference was −13.0 percentage points (95% CI: −15.9 to −10.0): The lower boundary was smaller than the prespecified −5 percentage-point non-inferiority margin. Thus, the non-inferiority of GP delivery was not met. Although the trial was intended to assess the non-inferiority of GP delivery over the home-mailed delivery, our findings demonstrated that participation in complete CCS was significantly lower with GP delivery than with home-mailed delivery (p ≤ 0.001).
Participation in Complete Cervical Cancer Screening Within 9 Months After Sending Reminder Letters, by Trial Group
p values were obtained from a ratio estimator approach based on the standard Pearson chi-square statistic with adjustment for clustering
ICC, intraclass correlation coefficient; GP, general practitioner.
Participation in complete CCS was mostly achieved by the use of Pap smear in the GP delivery group. Among the 269 women with complete CCS, 48 (17.8%) used self-sampling and 221 (82.2%) a Pap smear performed by a health professional. However, in the home-mailed delivery group, among 503 women with complete CCS, 314 (62.4%) used self-sampling and 189 (37.6%) a Pap smear performed by a health professional.
Participation in complete CCS by self-sampling was significantly lower in the GP delivery group as compared with the home-mailed group (2.7% vs. 17.4%; p < 0.001; Table 1). Participation in complete CCS by the use of Pap smear did not differ between groups (12.2% vs. 10.5%; p = 0.13).
Subgroup analysis according to age (35–49 vs. 50–65 years) consistently favored home-mailed delivery (pinteraction = 0.2831) (Supplementary Fig. S2).
Test results and women's follow-up
In the GP delivery group, 49 women performed self-sampling within 9 months, and 48 test results were interpretable, with 4 (8.3%) samples positive for HR-HPV (Fig. 2); the 4 women underwent the recommended triage Pap smear. A Pap smear test result was available for the 4 samples, and 1 was abnormal (25% of known results) (Supplementary Table S2).
In the home-mailed delivery group, 316 women performed self-sampling within 9 months, and 315 test results were interpretable, with 47 samples (14.9%) positive for HR-HPV; 46 (97.9%) of these women underwent the recommended triage Pap smear. A Pap smear test result was available for 44 of 46 samples, and 5 (11.4% of known results) were abnormal (Supplementary Table S2).
Finally, among women who participated in complete CCS at 9 months after the reminder letter, 4 had CIN2 grade cancer or worse: 1 CIN3 in the GP delivery group among women who had a Pap smear, 1 CIN2 in the GP delivery group among HR-HPV-positive women, 1 CIN2 in the home-mailed delivery group among women who had a Pap smear, and 1 CIN3 in the home-mailed delivery group among HR-HPV-positive women. In both groups, the CIN2+ detection rate among included women was 1.1‰.
Cost-effectiveness analysis
The mean cost per woman included was higher in the home-mailed than the GP delivery group (15.60€ vs. 9.01€) (Table 2). Nevertheless, the cost-effectiveness ratio favored the home-mailed delivery group (56.00€ vs. 60.52€) (Table 2). As compared with the GP delivery strategy, with the home-mailed delivery strategy, the gain in effectiveness generated an additional cost (ICER) of 50.81€ per extra screened woman. Costs of resources engaged per screened women for each intervention group are detailed in Supplementary Table S1.
Cost-Effectiveness Results
Base value.
Regarding the sensitivity analyses (Supplementary Table S3), the variable most affecting the ICER was the cost of home-mailed delivery. If this cost was 5€ instead of 1.559€, the ICER would be 77.36€ per extra screened woman. A 50% reduction in the cost of HR-HPV test analysis and mailing results (20.00€ instead of 37.80€) and a doubling of the probability of returning the test within 9 months in the GP delivery group (5.43% instead of 2.71%) would decrease the ICER (30.57€ and 45.93€). The other variables did not significantly affect the ICER.
Discussion
In a large sample of 3,612 women, we did not show the non-inferiority of GP delivery of a vaginal self-sampling kit and conversely, we found that participation in complete CCS was significantly higher in the home-mailed group. The substantial increase in participation with the home-mailed delivery strategy offset its higher mean cost, leading to a lower cost-effectiveness ratio as compared with the GP delivery strategy. Sending a kit directly to the home so that the women can take the sample themselves improved adherence to CCS.
Our study is the first to compare home-mailed delivery versus the delivery by the GP. In Italy, a similar trial assessed delivery by another health professional, the pharmacist. As for our study, participation was almost halved as compared with directly mailing the self-sampling kit to the women's home (21.6% vs. 11.9%). 22 This lower participation rate with health professional delivery could have several explanations. This strategy requires an additional step that consisted, in our study, of making an appointment with a GP.
Women may have felt embarrassed by this type of proposal or the autonomy offered by the kit may have frightened some of them, especially without seeing it. It would have been interesting to do subgroup analyses according to socioeconomic status and educational levels, but such information is not part of the Cancer Screening Department database. In addition, health professionals may not have been well informed about this new type of sampling.
Owing to the higher participation rate with the home-mailed than GP delivery strategy, the cost-effectiveness ratio was lower with the former strategy. Numerous studies have shown that offering a self-sampling kit to under-screened women is an effective or cost-effective strategy under certain conditions. 23 In our study, the home-mailed delivery strategy was more expensive, with an ICER of about 50€ per extra screened woman as compared with the GP delivery strategy.
However, the final ICER for the home-mailed versus GP delivery strategy depends on the total number of women targeted and the expected success rate of the strategy. To reduce this additional cost while maintaining the increased participation, the cost of the HR-HPV test must be reduced while ensuring that the cost of the vaginal self-sampling kit remains low.
Since the end of our study, many high-income countries, including France, have switched to or are in the process of switching to first-line HR-HPV testing. Some countries such as The Netherlands 24 and Australia 25 have already included home-mailed self-sampling kits as an option in their national screening programs. The French authorities recommended in 2019 to switch from the Pap smear to the HR-HPV test for women aged 30–65 and to offer the vaginal self-sampling kit to under-screened women. 26
At the same time, the national CCS program has been set up in France. For future implementation of self-sampling kits, the context will be more favorable. Communication with the health professionals and women will be strengthened. More strategies to improve the efficiency of the home delivery need to be explored: opt-in, online ordering, SMS recall etc. Opt-in strategies (self-sampling kit sent on demand) have not been tested in France, and we lack sufficient studies to determine whether this strategy would be cost-effective. 23 In addition, it would be interesting to evaluate the GP delivery of the vaginal self–sampling kit in an opportunistic approach. This kind of delivery experiment would require a study over a period of several years, and a qualitative evaluation about GP workload and the obstacles faced by women may complement such an approach.
In conclusion, we showed that GP delivery of a vaginal self-sampling kit resulted in significantly lower participation in complete CCS as compared with home delivery of the kit in France. Thus, offering a vaginal self-sampling kit could be an effective way to improve the CCS participation, but we cannot recommend the GP delivery strategy as implemented in our trial. More strategies based on self-sampling need to be evaluated to identify optimal and efficient strategies for national programs.
Footnotes
Acknowledgment
The authors thank all GPs and women who participated in the study.
Authors' Contributions
J.B. and K.H. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: J.B, S.S, B.G., and K.H.
Acquisition of data: Cancer Screening Department, Virology Laboratory.
Analysis and interpretation of data: J.B., A.C., S.B.-H., S.S., and K.H.
Drafting of the article: J.B., A.C., S.B.-H., C.G.-G., and K.H.
Critical revision of the article for important intellectual content: J.B., A.C., S.B.-H., B.G., H.M., E.R., C.G.-G., and K.H.
Statistical analysis: A.C.
Cost-effectiveness analysis: S.B.-H.
Obtained funding: J.B., S.S., B.G., and K.H.
Virology analysis: C.G.-G.
Help with writing intervention letters: G.R.-L.
Study supervision: J.B., S.S., and K.H.
Data Availability
Datasets are available from the corresponding author (subject to the applicable regulations: General Data Protection Regulation). Data will be made available to researchers whose proposed use of the data has been approved and with a signed data access agreement.
Author Disclosure Statement
The authors declare that they have no known competing interests, personal financial interests, funding, or employment that may inappropriately influence or affect the integrity of the work reported in this article.
Funding Information
This work was supported by a French National Cancer Institute INCa subvention (grant number: INCa no. 2013–120).
Supplementary Material
Supplementary Appendix
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.