
Abstract

Case Report
A33-
She has exhausted nonsurgical modalities including evaluation by a gynecologist and a psychologist. On physical examination, she has bilateral elongated labia minora with the anterior portion extending 2 cm beyond the labia majora, and right labia minora is longer than her left labia minora. She requests evaluation for surgical reduction for improvement of discomfort and aesthetics.
What are potential recommendations?
Continue nonsurgical modalities
Labiaplasty
Refusal of surgery
Psychiatric evaluation
Labia minora hypertrophy is elongation or protuberant tissue of the labia minora (Fig. 1). 1 Diagnosis is typically clinical; however, there is no formal consensus on diagnostic criteria among gynecologists, plastic surgeons, or pediatricians. Although there is variable normal anatomy, labia minora typically measure 3 to 5 cm (measured from sulcus to labial edge). 2

Female genital anatomy and hypertrophy of the labia minora.
Some define labial hypertrophy when “stretch width” of the labia minora is >6 cm or asymmetry of labia is >3 cm. 1,3 Some report labial hypertrophy measurements are less important and rather focus on symptomatology as an indication for treatment. 4 Labial hypertrophy is also variable from birth to later adulthood, and can be due to congenital causes, exogenous hormones, chronic irritation, pregnancy, childbirth, aging, and external physical causes from irritation, trauma, or chronic infections. 1,2
Management of labial hypertrophy typically starts with counseling and self-care instructions. Many of the recommendations from the gynecological literature are focused on reassurance and education about the variability of normal anatomy. 5 –7 It is recommended that functional symptoms be managed first by counseling of vulvar hygiene such as use of mild soaps, adjustments to types of sanitary pads, avoidance of tight clothing, and padding (such as bike shorts) when doing aggravating activities. 1 In addition, psychological counseling and or psychiatric care may be warranted. 3
Surgical reduction of the labia, labiaplasty, has significantly increased in the past decade for either improvement in cosmesis, discomfort related to hypertrophy, or both. 2 Reasons for interest in these procedures are variable. Some patients seek the procedure for purely cosmetic reasons, whereas others seek to alleviate discomfort, irritation, visibility through clothing, dyspareunia, hygiene issues, or difficulty with self-catheterization. 2,4
Labiaplasty is defined as surgery to reduce the size of the labia minora so that it is externally flush with the labia majora (outer part of the female genitalia). 8 Surgical procedures typically include procedures to reduce the length and volume of the tissues. Trim, wedge, and de-epithelialization of a segment are the primary surgical procedures and the approach is dependent on the blood supply and area of excess tissue (Fig. 2). Labiaplasty is typically an outpatient procedure and can be performed either in the office setting under local anesthesia or in the operating room under general anesthesia.
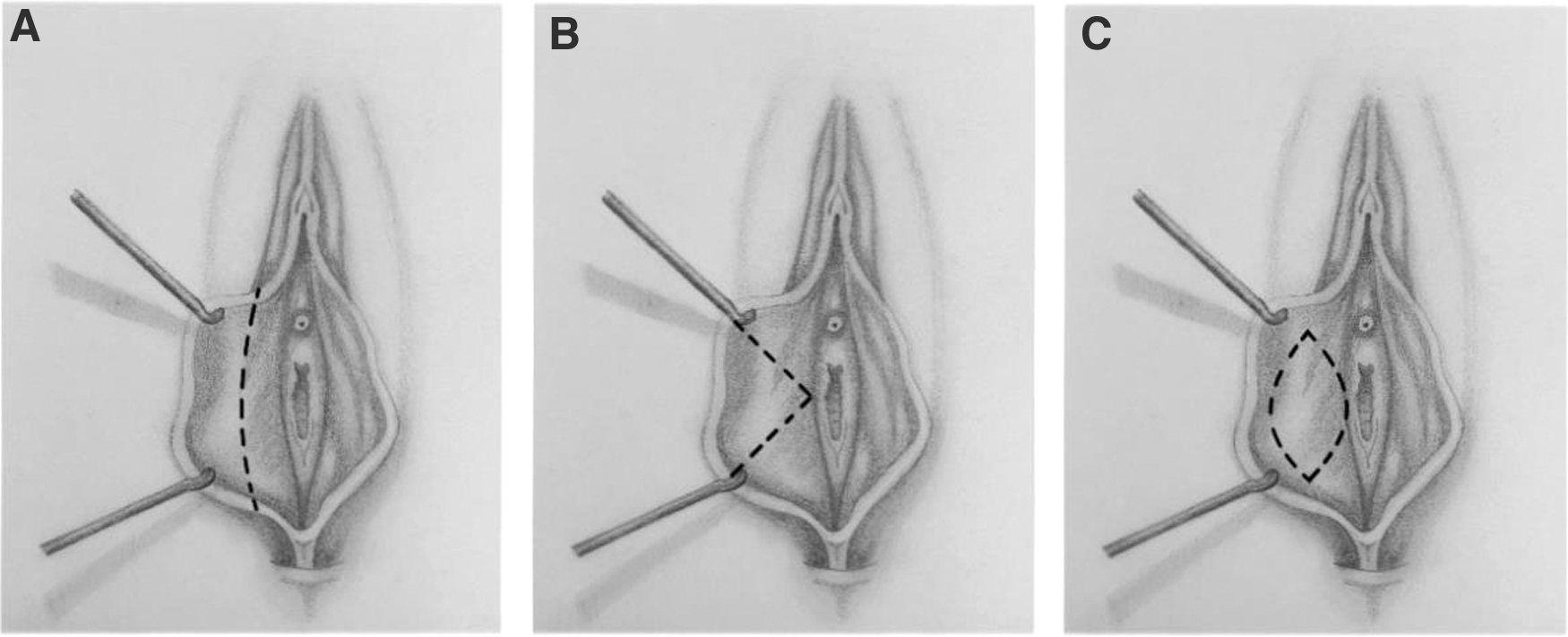
Surgical technique for reduction of the labia minora.
Postoperatively, patients are encouraged to elevate and ice frequently after surgery. Gentle wound care is typically recommended with use of a peri bottle and sanitary napkins. Patients are typically swollen and tender for the first 1 to 2 weeks. Preoperative antibiotics are standard in these procedures, and postoperative topical or antibiotic treatment is often done. Postoperative appointments are generally seen at 1 to 2 weeks for a skin check and evaluated at 4 to 6 weeks for complete healing. Patients can resume activities ∼1 month after surgery and sexual activity around 6 weeks.
Answer: The Best Answer Is B
Ethics behind labiaplasty have previously been tenuous due to the illegal female genital mutilation in some areas of the world, influence of social media, and concern for patients with body dysmorphic disorder. In the 2007 and 2019 Committee Opinion, the American College of Obstetricians and Gynecologists (ACOG) published a formal article that vaginal rejuvenation and cosmetic vaginal procedures lacked data and efficacy to support these procedures. 7 ACOG also expressed that procedure risks were too high and instead suggested reassurance to women for the wide variability of female genital appearance.
In 2017, the committee on adolescent health care allowed consideration of surgical procedures on genitalia if the patient has significant congenital malformation, or persistent symptoms that the physician believes are caused directly by labial anatomy, or both. 9 Despite this, the number of women seeking labiaplasty has significantly increased and satisfaction rates are high. 4,10 –12 The American Society for Aesthetic Plastic Surgery began tracking labiaplasty procedures in 2011, and the number of labiaplasties performed has increased 539% over the past decade with 2,142 procedures performed in 2011 to 13,697 procedures performed in 2020. 13
Careful preprocedural evaluation is critical when considering a labiaplasty to determine suitability for the procedure by carefully discussing patient goals, motivation, and expectations. Lowenstein et al. showed that self image is a major predictor in requesting labiaplasty and suggests that evaluation by a counselor, psychologist, or psychiatrist is important in the work-up for the procedure. 3,14
Some studies suggest that social media has played a significant role in patient motivation for these procedures and that careful counseling about the wide variability in normal anatomy plays an important role in educating patients before undergoing a surgical procedure as, after education, some might not pursue surgery. 15,16 Although some argue that social media negatively influences women who seek out labiaplasty, other studies find few view pornographic images before labiaplasty and rather women look to the internet to find out how to address their concern rather than the other way around. 17,18
Option A with all body altering procedures such as tattoo, body piercing, and cosmetic/elective surgery (breast augmentation), women have a right to exercise bodily autonomy and alterations to their body given adequate informed consent. 3 The ethical challenges surrounding labiaplasty are significant given the wide variability of acceptable anatomy, difficult determination of abnormal anatomy, varying surgical committee stances on treatment, and the history of genital mutilation of women. Most agree, however, that labiaplasty can be considered after careful evaluation of goals, motivations, and expectations.
Complications generally for surgery include, but are not limited to, bleeding, infection, damage to surrounding structures, pain, poor cosmetic outcome, sensory changes, and need for revision surgery. Labia minora reduction specifically can have edge separation or stretching of the labium, notching, dehiscence, over-resection of the mucosal portion resulting in a “coin slot” deformity, and possible inferior displacement of the clitoris. 19 In addition, patients must be counseled that labiaplasty might not resolve physical and sexual complaints. 3
Despite its controversy, the data show that overall complications are low and satisfaction is high. 4,10 –12 Labiaplasty has been found to increase confidence and have a high satisfaction rate (>90%). 12,20 Many studies have evaluated the safety and efficacy of labiaplasty. One study notes 93.5% of patients were symptom free after labiaplasty with improvement in self-consciousness, tugging, clothing restriction, negative impact on intimacy, and visibility in clothing and swimsuits. 2 Another study evaluated the impact of labiaplasty on sexuality and found that labiaplasty improved pain and enjoyment of the patient's sexual life. 21 Most studies report low incidence of complications. 2,21
At present, labiaplasty is not routinely covered by insurance and is considered a cosmetic procedure. Insurance coverage may be provided with transgender surgery for gender dysphoria and for patients who have had recent trauma with the need for reconstruction, or in some cases of congenital deformity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.